“Kurdistan” Technique for the Treatment of Unprotected Trifurcation Left Main Stem Coronary Artery Lesion: Case Report ()
1. Introduction
Significant unprotected left main coronary artery disease (LMCA) occurs in 5% - 10% of patients undergoing coronary angiography [1] [2] . Serruys reported that revascularization with PCI has comparable safety and efficacy outcomes to CABG for patients with LMCA disease [3] .
The LMCA is generally divided into three anatomic regions: The ostium or the origin of the LMCA from the aorta, amid portion and the distal portion. Left main trifurcating coronary artery disease (LMTCAD) is a complex and challenging anatomy to treat percutaneously.
The clinical indicators of LMCA stenosis are easily recognized and include a crescendo pattern of angina pectoris, an electrocardiogram ECG with ST-segment depression with pain or with simultaneous anterior or inferior ST segment changes and fluoroscopic calcification of the LMCA [4] . These indicators are not specific and the gold standard for treatment is coronary angiography.
Several recent large registries and randomized controlled trials such as the MAIN-COMPARE (Revascularization for Unprotected Left Main Coronary Artery Stenosis: Comparison of Percutaneous Coronary Angioplasty Versus Surgical Revascularization) registry, SYNTAX (Synergy between PCI with TAXUS and Cardiac Surgery), and PRECOMBAT (Premier of Randomized Comparison of Bypass Surgery versus Angioplas Ty Using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease) randomized trials have demonstrated that LMCA stenting yields comparable mortality and morbidity rates to CABG. [5] -[7] , in addition several observational studies revealed that the early clinical events of LMCA stenting were similar or superior to those of CABG because of significant increase in periprocedural myocardial infarction (MI) or stroke in CABG patients, and that mortality between 30 days and 3 years was similar in both the Groups [8] . However, the risk of target vessel revascularization was higher with PCI than CABG [9] -[11] .
Several modifiable procedural factors need to be addressed to achieve better outcomes of LMCA stenting, the intravascular ultrasound (IVUS) provides accurate information about stent sizing and helps to detect suboptimal stent deployment or stent-related complications, thereby making LMCA PCI safer and more effective. Previously, the MAIN-COMPARE registry, and more recently, the de la Torre Hernandez et al. [12] study, demonstrated that IVUS-guided LMCA stenting is associated with less mortality [12] [13] . Second, for the distal left main disease, the PCI strategy may affect the prognosis. In general, the single-stent technique clearly shows more favorable long-term clinical outcomes compared with the 2-stent technique, even in true bifurcation stenosis [14] .
Physiological assessment fractional flow reserve (FFR) of the lesion is also to be considered during LMCA PCI. Several studies already demonstrated that FFR-guided decision making for the treatment of LMCA is associated with favorable prognosis and the intermediate LMCA lesion with FFR 1/4 0.75 to 0.80 could be safely deferred [15] .
In addition, for LMCA stenosis, if FFR measurement is not feasible, the IVUS minimal lumen area (1/4 4.8 mm2) could be used as a definition of significant functional stenosis [16] .
For risk stratification for procedural and long-term outcomes combination of SYNTAX and the Euro SCORE into a common risk model (Global Risk Classification) was correlated with a significant improvement in predicting cardiac mortality in patients undergoing PCI for LMCA [17] . Another score, the New Risk Stratification Score showed a higher sensitivity and specificity to predict clinical outcome [18] .
Kurdistan technique consist of simultaneous stent implantation for LMS-ramus intermedius branch & LMS-left circumflex (LtCx) artery both should be localized ostialy with 1 mm protrusion to the LMS, meanwhile keeping balloon in LMS—left anterior descending (LAD) artery after LMS-LAD stenting, then simultaneous inflation of three balloons to variable atmospheres.
2. Case
A 56-year-old hypertensive, non-diabetic, ex-smoker male patient presented with Canadian Cardiovascular Society (CCS) class III-IV angina, his baseline ECG & trans-thoracic echocardiography were non-significant for ischemia. Angiography demonstrated diseased distal left main stem( LMS) with about 40% - 50% stenosis, critical ostial & proximal LAD lesion, significant ostial left circumflex (LtCx) & 95% ostial ramus intermedius lesion, the LMS was 4.1 mm in diameter & proximal LAD was 3.8 mm (Figure 1(a) & Figure 1(b)).
The LAD, LtCx & ramus intermedius were wired with floppy wires (Balance Middle Weight Universal (BMW) Abbott Vascular, Santa Clara, USA), the LMS-LAD pre-dilated with 3.0 × 15 mm balloon at 16 atm. Ramus intermedius was predilated with 2.5 × 15 mm non-compliant (NC) at 14 atm.
The LMS-LAD was stented with Resolute Integrity stent (Zatrolilimus-Eluting, Medtronic, Minneapolis, USA) 4.0 × 18 mm at 14 atm (Figure 2). Second stent Resolute Integrity stent (Zatrolilimus-Eluting, Medtronic, Minneapolis, USA) 3.5 × 26 mm at 14 atm implanted distally with 1 mm overlap with proximal stent, ballooning done in-between two stents at 16 atm (Figure 3 and Figure 4).
Re-wiring done for the LMS-ramus intermedius & LMS-LtCx through stent struts with floppy wires (Balance Middle Weight Universal (BMW), Abbott Vascular, Santa Clara, USA) & kissing ballooning done for LMSLAD, LMS-ramus Intermedius & LMS-LtCx with balloons (3.5 × 15 mm, 2.75 × 15 mm & 2.75 × 15 mm) consecutively with simultaneous inflation at first between LMS-LAD Vs. LMS-ramus intermedius 14 Vs. 12 atm, then LMS-ramus intermedius & LMS-LtCx 12 Vs. 12 atm simultaneous inflation & then between LMS-LAD Vs. LMS-ramus intermedius Vs. LMS-LtCx at 14 Vs. 12 VS 12 atm simultaneous inflations (Figure 5).
Angiography done shows dissection in the ostium of ramus intermedius (Figure 6) & proven by IVUS (Figure 7).
 (a)
(a) (b)
(b)
Figure 1. It shows critical distal LMS, ostial & proximal LAD lesion, critical ostial & significant ostial LtCx lesion in LAO-CAU & PA-CAU projections.

Figure 2. It shows stenting for LMS-LAD with (4.0 × 18 mm) DES 16 atm. with 1 mm overlap with the proxymal stent.

Figure 3. It shows ballooning in-between 2 stents after implantation of (3.5 × 26 mm) DES in proximal LAD.

Figure 4. It shows LMS & proximal LAD after stenting. LtCx to variable atmospheres.

Figure 5. It shows simultaneous kissing stenting between LMS-LAD Vs. LMS-ramus intermedius & LMS.
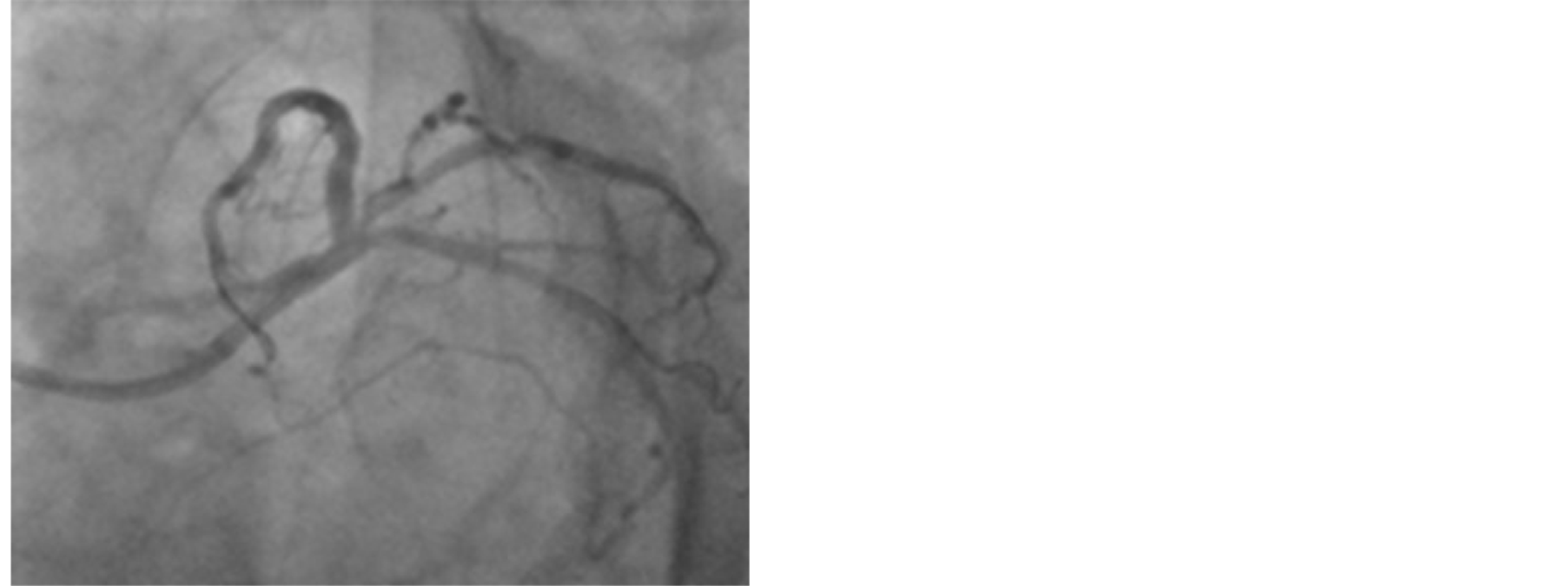
Figure 6. It shows dissection of ostial ramus intermedius after ballooning.

Figure 7. IVUS showing the ostial ramus intermedius.
Technique:
A new technique (Kurdistan technique) was used for trifurcation ULMCA stenting, Resolute Integrity stent (Zatrolilimus-Eluting, Medtronic, Minneapolis, USA) (2.75 × 15 mm) localized in the ostial ramus intermedius with 1 mm protrusion to the LMS & another stent Resolute Integrity (Zatrolilimus-Eluting, Medtronic, Minneapolis, USA) (3.0 × 15 mm) localized in the ostial LtCx with 1mm protrusion to the LMS, meanwhile (3.5 × 20 mm) non-compliant balloon placed in the LMS-LAD after stenting for LMS-LAD, simultaneous inflation for both stents done at 14 atm both (Figure 8), after that both balloons were withdrawn to the LMS-ramus intermedius & LMS-LtCx consecutively, then simultaneous inflation done between LMs-LAD Vs. LMS-ramus intermedius Vs. LMS-LtCx at 14 Vs, 12 Vs. 12 atm simultaneously (Figure 9) with good final results (Figure 10(a) and Figure 10(b)).
3. Discussion
True distal bifurcation lesions may be treated by either a single-stent or by a two-stent strategy. Choice of strategy is based on vessel and lesion characteristics.
Choice of strategy is based on vessel and lesion characteristics (plaque distribution, the diameter of the branches and the angle between them, anatomy of the side branch) but also on operator’s experience.
For distal left main stenosis, stenting across the bifurcation toward the left anterior descending was performed

Figure 8. It shows Kurdistan technique; simulta-neous 2 stent implantation in the ostial LtCx & ostial ramus intermedius with 1 mm protrusion to LMS both, meanwhile keeping NC balloon in LMS-LAD.

Figure 9. It shows kissing inflation between LMs-LAD Vs. LMS-ramus intermedius Vs. LMS-LtCx to variable atmospheres.
 (a)
(a)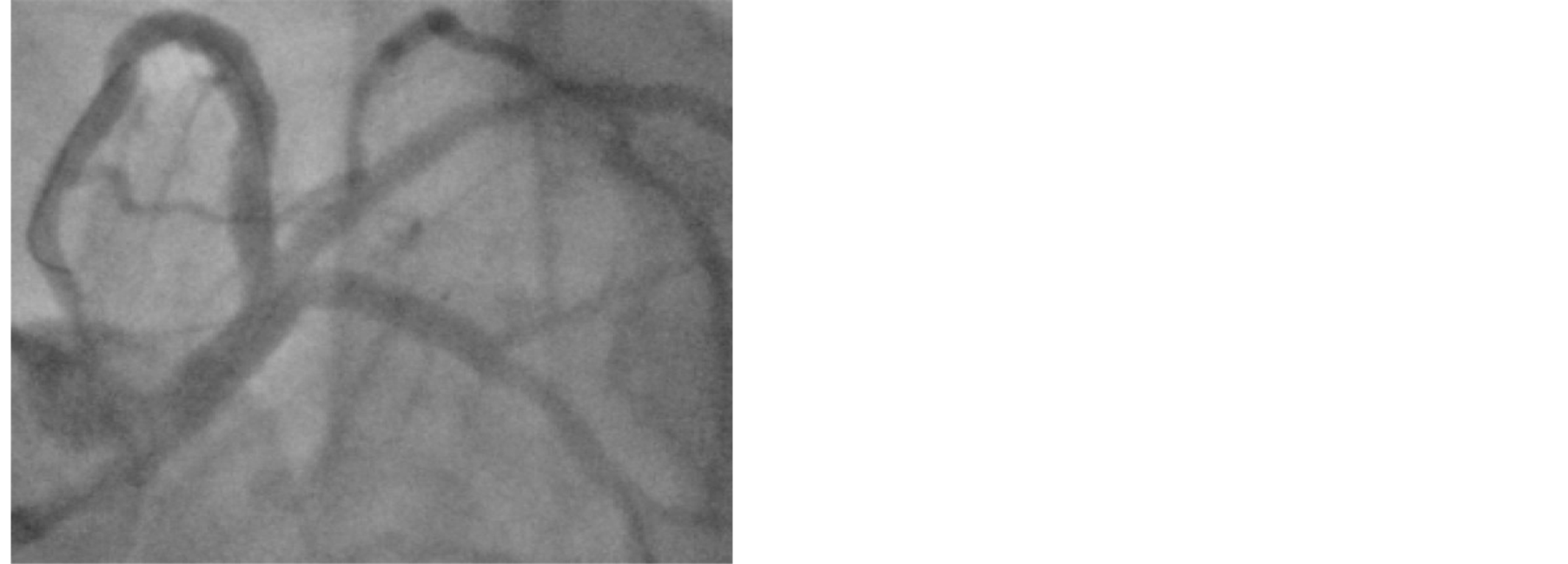 (b)
(b)
Figure 10. It shows final results.
first, and then provisional stenting of the circumflex artery with T-stenting or “culotte” technique was preferred.
Post-dilation with kissing balloon angioplasty was always used to finish the distal left main stenting procedure [19] .
The provisional stenting is a single-stentstrategy, although it allows the placement of a second stent if required [T, T and protrusion (TAP), culotte techniques]. More complex lesions may require double-stent strategy (T stenting, TAP, crush, culotte, V stenting).
3.1. Double-Stent Strategies
3.1.1. The Culotte Stenting
This is a strategy suitable for lesions where the ostium of the LtCx is diseased, the angulation between the vessels is 60 - 80 (higher risk of plaque shift), and the two vessels are of similar diameter.
This technique provides an optimal reconstruction of distal LMS bifurcation but with a significant area of stent overlap.
3.1.2. The T Stenting
The T stent is used when a two-stent strategy is required but the angulation between the two vessels approached 90.
This technique provides a good reconstruction of T shape distal LMS bifurcation but with the risk of leaving the side branch ostiumun covered (side branch stent to distal) or of placing the side branch stent to proximal protruding in the LM stent.
3.1.3. The T and Protrusion (TAP) Technique
This technique can be used in the majority of the bifurcation lesions. It can provide a good reconstruction of distal LMS bifurcation with minimal stent overlap.
3.1.4. The Crush Stenting
The crush technique can be used when the diameter of the main vessel is greater than the side branch and the angulation is favorable (approximately ≤ 60%). The side branch is stented first, positioning the stent to allow 1 - 2 mm (mini-crush) to protrude into the LM.
3.1.5. The V Stenting
The V stent technique (or “kissing stent” technique) is mainly used inMedina 0, 1, 1 lesion that can be treated with a minimal and very shortneo-carina [20] .
LM trifurcation disease is typically treated surgically, particularly when the LM artery is involved, therefore its percutaneous treatment is generally reserved to high-volume centers performing complex coronary interventions.
There are 2 types of left main trifurcation diseased:
Type A, involving the main trunk with extension to one or more of the origin of the branches;
Type B, involving the origin of one or more of the main branches without extension to the main trunk (MT) [21] .
In our cases, special new technique is used for treatment of Trifurcational LM lesion, the initial steps were similar to traditional stenting which is stenting LMS-LAD, then rewiring of 2 side branches and then kissing ballooning between three (main trunk & two side branches) with simultaneous inflations between all three, when decision for stenting of the side branches is taken then two stent will be placed in the ostium of both side branches with minimal protrusion to the LMS, with concomitant placement of a balloon in the LMS-LAD, both stents are inflated simultaneously, then both balloons are withdrawn to the LMS & simultaneous kissing inflation done between all three.
4. Conclusions
LM trifurcation stenting carries an overall high rate of adverse events, mostly driven by a high target lesion revascularization (TLR) rate. Type A lesions and the number of stents placed predicted a higher combined endpoint of death, nonfatal MI and TLR. By logistic regression analysis, Type A lesions are the only independent predictors of the primary outcome.
This technique (Kurdistan technique) for treatment of unprotected trifurcation LMS lesion seems to be promising provided that it is conducted by experienced operator in high-volume centers performing complex coronary intervention. Intravascular imaging is a key for successful and optimum final results.