Seroprevalence of and Risk Factors for Cytomegalovirus among HIV-Infected Patients at University of Maiduguri Teaching Hospital, Nigeria ()
1. Introduction
Cytomegalovirus (CMV) is a ubiquitous infection with estimated seropositivity among adults ranging from 40% - 79% in western countries to 96% - 100% in Africa and Asia [1] . Human CMV may be transmitted from a variety of sources, including saliva, urine, blood, cervical secretions, and semen [2] . Although primary CMV infection is usually benign, the virus remains latent within the host, this characteristic is also exhibited by other herpesviruses [3] [4] . Under conditions of immune compromise, especially impairment of cell-mediated immunity as seen in HIV infected patients, latent virus may reactivate to produce a variety of clinical syndromes, including chorioretinitis, oesophagitis, colitis, pneumonia, encephalitis, and adrenalitis [5] [6] .
Autopsy and clinical studies indicate that 90% of patients with AIDS develop active CMV infection during their illness, with life or sight-threatening complication in about 25% attributable to direct effect of the virus [6] [7] . Dual infections may thus provide the potential for adverse virus-virus interaction including increase in sexual transmission.
The prevalence of infection in a given population can only be reliably estimated by laboratory testing as clinical symptoms are usually absent. Cytomegalovirus seropositivity is considered as the best laboratory measure of past infection [8] .
Determination of local CMV seroprevalence is important especially in regions where the infection is perceived to be common. This will assist identifying risk factors for its acquisition and developing prevention strategies. To the best of our knowledge, there are hitherto no seroepidemiological data available on the prevalence of CMV infection in HIV patients in north east Nigeria. We carried out a serological screening for IgG antibody to CMV (antiCMV) and determined the risk factors associated with acquisition of CMV infection in a population of HIV positive patients.
2. Methods
One hundred and eighty subjects including 100 newly diagnosed ART naïve, HIV-positive patients and 80 apparently healthy HIV negative individuals were consecutively recruited into the study. Consent was obtained from the participants, participation was voluntary, the benefits and risks if any were explained to the patients. Detailed history and information on socio-demographic characteristics were obtained using a structured questionnaire. A thorough clinical examination was done on each participant. Human IgG antibody to human CMV was detected using enzyme-linked immunosorbent assay (ELISA) (Calbiotech®). Human immunodeficiency virus infection was screened for and confirmed using ELISA and Western blot techniques respectively. Diagnosis of AIDS was established by the CDC clinical criteria and/or CD4+ cell count of <200 cells/µL [9] . SPSS version 11.0 (SPSS, Chicago, Illinois, USA) was used for statistical analysis. Continuous variables were expressed as mean ± standard deviation. Differences were determined using Chi-square test with Yates correction. A p value of <0.05 was considered significant.
Ethical approval for the study was obtained from the Research and Ethics Committee of the University of Maiduguri Teaching Hospital.
3. Results
Among the 100 HIV-positive subjects 34 were males and 66 females, (male to female ratio = 1:1.9). Amongst the 80 controls, 40 were males and 40 females (male to female ratio = 1:1).The mean age of the subjects and controls were 31.82 ± 8.25 years and 29.00 ± 8.03 years respectively. Majority of the study population were less than 40 years (Figure 1).
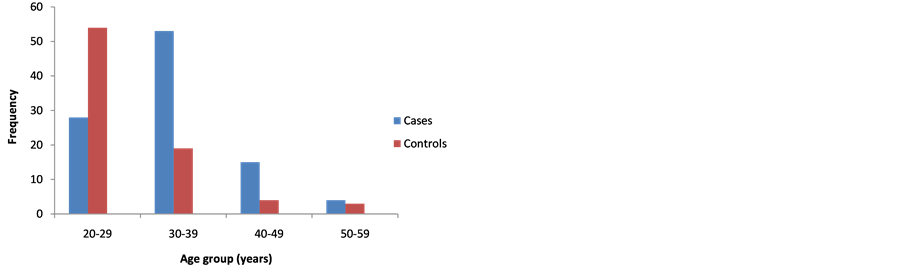
Figure 1. Age distribution of cases and controls.
The unschooled constituted the largest group among both cases (37%) and controls (60%). Many of the cases were unemployed (46% cases vs. 30% controls, p = 0.042) and from rural areas (60% cases vs. 44% controls, p = 0.044) (Table 1).
The mean CD4+ cell count of the HIV-positive cases was 223.5 cells/µL. Majority of the HIV positive patients had CD4+ counts < 200 cells/µL (Table 2).
The prevalence of anti-CMV IgG antibody was found to be 100% in the cases and 98.6% in the controls.
The distribution of risk factors for the acquisition of CMV infection between cases and controls in the study population is illustrated in

Table 3. Having multiple sexual partners, traditional practices such as tattooing and cupping, and blood transfusion were significant risk factor among the cases.
4. Discussion
We determined the seroprevalence of CMV among HIV positive patients and controls in a tertiary health institution north east Nigeria through detecting IgG antibody to CMV in the serum of participants. Seroprevalence of anti-CMV IgG was 100% among our HIV-infected cohort. This is in agreement with report from the Lagos University Teaching Hospital, south west Nigeria and Burkina Faso by Akinbami et al. [10] at and Ledru et al. [11] respectively that documented a prevalence of anti-CMV IgG antibody of 100% among HIV-infected patients.
Table 1. Characteristics of CMV seropositive cases and controls.
Table 2. CD4+ cell count and anti-CMV IgG antibody amongst HIV cohort.
Table 3. Risk factors for the transmission of CMV among studied participants.
However Adjei et al. [12] reported a lower seroprevalence of 59.2% in Ghana. The higher mean CD4 count of their population may have contributed to this difference.
The reported seroprevalence rate of 98.6% for CMV IgG among HIV-seronegative healthy controls is comparable to the rates of 97%, 96%, and 92% reported in Tunisia [13] , India [14] and north central Nigeria [15] respectively. These prevalence rates are higher than the figure recorded in another study by Olaleye et al. [16] in Ibadan, Nigeria where the authors found a prevalence of 54.6% among healthy blood donors. This may be attributed to differences in screening technique used. The prevalence rates reported in the aforementioned studies are higher than those reported in Western populations [17] .
The high CMV seropositivity rate in this study is suggestive of widespread past exposure to infection and may explain the lack of statistically significant differences in the seroprevalence of CMV in HIV-seronegative healthy individuals and HIV-AIDS patients. The hyperendemicity of CMV infection in both HIV-seronegative individuals and HIV-seropositive patients poses a major threat to individuals at risk of CMV disease like HIV/AIDS patients. The reasons for the high prevalence may be an increase in the distribution of epidemiological risk factors prevalent in these areas, as well as lack of access to health information, education and communication.
Majority of the subjects were either unschooled or had only primary education. This may be a reflection of the present poor state of education in Nigeria, which is more prevalent in these areas perhaps due to lack of proper commitment as well as poor governance at the local and state government levels [18] . Studies have shown lack of education or ignorance as one of the factors responsible for the acquisition of CMV infections [19] [20] .
Having multiple sexual partners and blood transfusion were found to be significantly more in the cases than controls. Studies have shown sexual promiscuity and STDs to be associated with both HIV and CMV [21] [22] because of the shared route of transmission. The prevalence of risk factors like traditional circumcision, scarifications, barbing, uvulectomy, and nail cutting was relatively high. These practices have been found to be common among individuals belonging to the low socio-economic status [23] who constituted the vast majority of subjects in this study. The findings in this study highlight the role of non-sexual transmission as additional primary modes of transmission of CMV in Nigeria, similar to that suggested in previous reports from other endemic areas [21] [24] [25] .
5. Conclusion/Recommendation
The high seroprevalence of CMV antibodies among both HIV-positive and HIV-negative individuals suggests endemicity of this infection in our environment. Sexual transmission and traditional practices plays a significant role in acquisition of CMV infections in this part of Nigeria, therefore health education on preventive measures is expedient with emphasis on identified risks of acquisition of CMV infection from this study.
Acknowledgements
We wish to acknowledge and thank the management of University of University of Maiduguri through its Research and Ethics committee for granting us permission to conduct this research and Mr Baba Sanda Bukar of the Immunology Department, University of Maiduguri Teaching who assisted in conducting ELISA and Western Blot tests on the samples.
Competing Interests
None.
Author Contributions
IMK, BAD, BB MAT, BGW, IU, ISK, SAK HY conceptualized the study, collected data and carried out the statistical analysis. IMK, BAD and BB wrote the manuscript.
NOTES
*Corresponding author.