Posterior Mediastinal Mature Teratoma: A Case Report and Literature Review ()
1. Introduction
Teratomas are encapsulated tumors derived from the three primary germ layers; Mesoderm, Endoderm and Ectoderm. These are rare tumors in young patients and their location in the posterior mediastinum has not been the subject of many publications [1] . We report a case of a posterior mediastinal mature teratoma (MMT) in a patient of 37 years.
2. Case Presentation
Mr. I. S. smoked for 14 years, weaned, presents with a right chest pain, progressively worsening over month. Except a right chest effusion syndrome, clinical examination was unremarkable. The routine laboratory tests were normal. A chest X-ray radiograph (Figure 1(a)) showed a well-circumscribed rounded homogeneous post
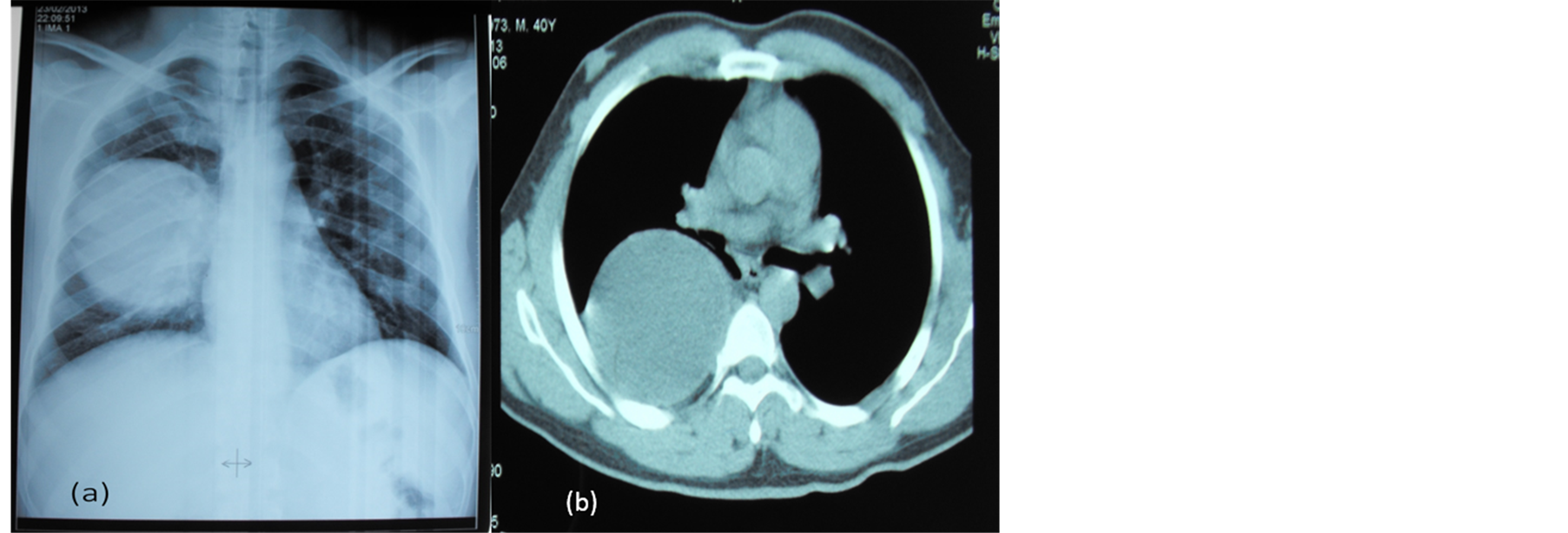
Figure 1. (a) Chest X-ray showed a well-defined rounded opacity of the right hemi thorax. (b) CT with injection of contrast showed a heterogeneous cystic lesion with fat, fluid levels on the right costovertebral groove.
erior opacity of the right hemithorax. The computed tomography (CT) scan with injection of contrast showed a heterogeneous cystic lesion with fat, fluid levels on the right costovertebral groove with regular lung interface. There were no signs of invasion (Figure 1(b)). The diagnosis of posterior mediastinal teratoma was retained not excluding a neurogenic tumor or a liposarcoma. A right postero lateral thoracotomy was decided. Intraoperatively we found a cystic mass containing brownish liquid in the posterior mediastinum. The mass was in intimate contact with the esophagus, the right main bronchus, the right atrium and the right lower pulmonary vein. Complete excision of the mass was performed with extreme caution. The final histopathological examination confirmed the diagnosis of a mature cystic teratoma without mediastinal immature or malignant tissues (Figure 2). The immediate post-operative evolution was simple, chest catheter was off at day 3 and patient was discharged at day 5 after surgery. The clinical and radiological control was satisfactory at three months later.
3. Discussion
A mediastinum location of a teratoma is uncommon 4% - 10% [1] . It represents however 60% of embryonic mediastinal tumors and it is mature in 80% to 88% of cases [2] . The posterior mediastinum is the usual site of neurogenic tumors (80% - 90%), para oesophageal cysts, and mesenchymal tumors including liposarcomas. Only 3% - 8% of mediastinal teratoma [3] is located in the posterior mediastinum. In adults, the discovery of a mediastinal teratoma is often accidental, when performing a routine chest radiograph. It is a large mass, well-circumscribed and lobulated, with calcifications in 20% of cases [4] . A CT scan is the choice investigation, it specifies the location of the mass, and highlights a combination of fluid density, fat and calcifications in 40% of cases, highly suggestive of mediastinal teratoma [4] . It also examines the relations of the mass with adjacent organs, indicating the presence or absence of tumor border and regularity of tumor interface with the lung and adjacent mediastina structures, and the possibility of surgery. The discovery on chest CT of a heterogeneous process with cystic fluid density and fat allowed us to suggest the diagnosis of teratoma in our patient. Treatment is surgical. It confirms the diagnosis by eliminating the presence of an immature component and prevents the occurrence of complications [5] . Posterior lateral thoracotomy remains the most ideal way for surgery. Video-assisted surgery is often limited by the large size of teratomas and the frequency of adhesions with noble mediastina structures, as we report in this case [6] . From a histological point of view, mature benign teratoma occur readily as cystic tumors composed in varying proportions of different tissues having attained a high degree of differentiation. They can however be composed of skin, cartilage, calcifications, smooth muscle, bronchial epithelium or rarely thymus tissue, pancreas, or thyroid [7] . This pluritissulaire constitution with a respiratory epithelium and the presence of smooth muscle is also found in our study.
4. Conclusion
The posterior mediastinum is a rare seat of MMT. CT is the modality of choice in the diagnosis of these tumors, regardless of their location. Surgery remains the ideal treatment to confirm the diagnosis, prevent complications and eliminating the existence of immature component, whose presence would indicate the adjuvant therapy.
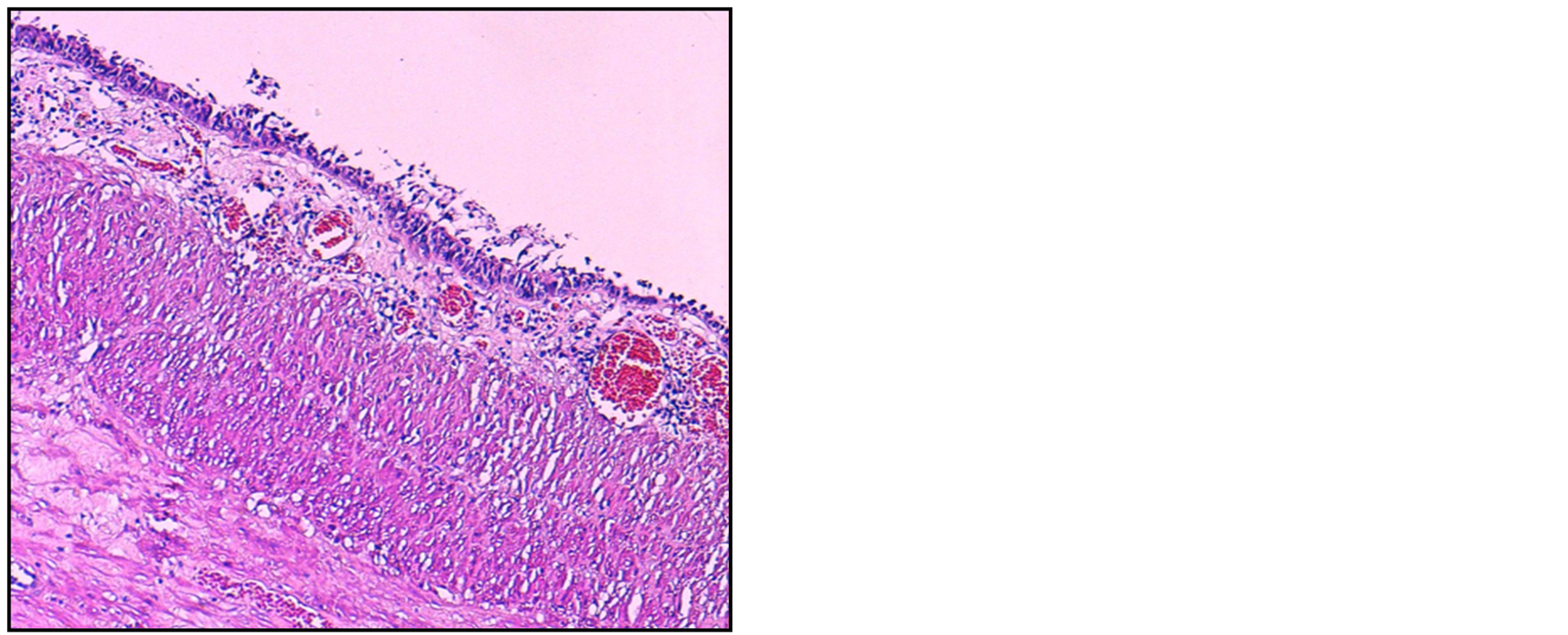
Figure 2. (HES 100×) Histology of the teratoma, with mature differentiated tissue of various origin.
Consent
Written informed consent was obtained from the patient for the study and publication of this case report and accompanying images. A copy of written consent is available for review from the Editor-in-Chief.
Authors’ Contributions
SR collected information and prepared the original draft. ML and JG researched the relevant literature and revised the draft. YO helped with the literature research and preparing the manuscript. MS helped prepare the manuscript. All authors read and approved the final manuscript.
Competing Interests
The authors declare that they have no competing interests.
Abbreviations
MMT: Mature mediastinal teratoma
NOTES
*Corresponding author.