Inflammatory Pseudotumor of the Anterior Mediastinum Appearing as a Thymic Malignancy: Report of a Case ()
1. Introduction
There are few reports on thoracic inflammatory pseudotumor (IPT) mimicking a thymic neoplasm [1] [2] . We herein report a case of IPT of the mediastinum that showed strong enhancement on 18-fluorine fluorodeoxyglucose positron emission tomography (18F-FDG-PET) and was thus suspected to be a thymoma or thymic carcinoma.
2. Case Report
A 69-year-old male patient with stomatitis and anorexia was diagnosed with an anterior mediastinal tumor as revealed by computed tomography (CT) (Figure 1). Following the diagnosis, he underwent FDG-PET. Upon referral to our department, the mass lesion measured 70 mm in diameter on CT and showed high uptake of 18FFDG with a maximum standard uptake value (SUVmax) of 10.24 on PET (Figure 2). He showed no clinical or laboratory evidence of lymphoma. The lesion was diagnosed as a thymoma or thymic carcinoma based on the CT findings, without biopsy, according to previously described criteria [3] . The patient then underwent complete surgical resection of the mass. With the patient in the supine position, video-assisted thoracoscopic thymectomy was attempted through the left pleural space. However, severe adhesion was encountered between the mass and the left brachiocephalic vein (Figure 3). The adhesion could not be distinguished from tumor invasion. Therefore, the procedure was converted to open resection through a trapdoor incision involving a median sternotomy with extension to an anterior left thoracotomy and a supraclavicular incision. The lesion was completely resected with combined segmental resection of the left brachiocephalic vein. Histologic examination revealed the presence of proliferating spindle cells and oval cells with a background of infiltrating lymphocytes and plasma cells; these findings were compatible with the typical histologic features of IPT (Figure 4). No malignant cells were observed in the resected specimen. The brachiocephalic vein was histologically free from invasion of the pseudotumor. The patient made an uneventful recovery and has been well with no evidence of disease recurrence for 15 months since the surgery.

Figure 1. Computed tomography showing a tumor measuring 70 mm in diameter in the anterior mediastinum and an anomalous right aortic arch.

Figure 2. 18-Fluorine fluorodeoxyglucose-positron emission tomography showing abnormally high uptake in the anterior mediastinum.
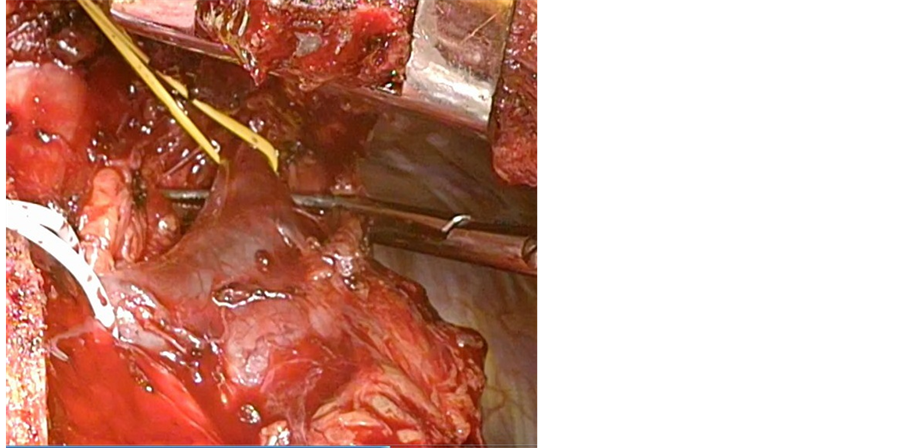
Figure 3. Surgical view showing adhesion between the pseudotumor and the left brachiocephalic vein.

Figure 4. Photomicroscopic findings showing spindle cells with a background of infiltrating plasma cells and lymphocytes.
3. Discussion
IPT is a non-neoplastic inflammatory process characterized by a tumor-like appearance as an indolent tumor in most cases [4] . IPT affects both sexes and all races equally, and patient age at presentation ranges from 1 to 73 years [1] . IPT is known to occur in a variety of organs or tissues, including the lung, liver, spleen, urinary tract, and soft tissue; the lung is the most frequent origin [5] . However, we found only a few reports of IPT originating in the anterior mediastinum in a PubMed search of the English-language literature [1] [2] .
IPT usually shows oncologic characteristics similar to those of benign tumors, such as a very low incidence of invasion or metastasis [6] . IPT was once believed to be a benign mass lesion containing various proportions of fibroblasts, myofibroblasts, plasma cells, and lymphocytes all recruited in an inflammatory process. Therefore, IPT was termed inflammatory myofibroblastic tumor (IMT), histiocytoma, plasma cell granuloma, or xanthoma depending on the predominant cell in the affected patient [7] . More recently, however, Lawrence et al. [8] reported rearrangement of the anaplastic lymphoma kinase gene in some patients with IMT. Considering these findings and a higher likelihood of invasion or metastasis, IMT is currently considered to be a neoplasm and is no longer categorized as IPT [2] . The histologic features commonly seen in IMT were not observed in the present case.
Recent studies reported positive correlations between the malignant grade of thymic epithelial tumors and the SUVmax on FDG-PET [9] [10] . As suggested by these studies, we initially considered the lesion in our case to be thymic carcinoma or thymoma with a high-risk histologic subtype (type B2 or B3) based on the extremely high SUVmax. However, the presence of a high SUVmax also depends on various inflammatory cell-mediated processes other than glucose metabolism in tumor cells [10] . Our case suggests that IPT should be included among the differential diagnoses when an abnormally high SUVmax is observed in a mediastinal mass on FDG-PET.
Surgery is the most reliable modality for both treatment and definitive diagnosis of IPT when appropriate. IPT is usually difficult to diagnose without biopsy, considering its radiologic features. The effectiveness of nonsurgical treatment remains unclear, although the use of antitumor drugs, steroids, and radiotherapy has been reported in patients with unresectable IPT of the anterior mediastinum [2] . Spontaneous regression has been reported in some cases of IPT, but there is currently no method by which to predict spontaneous cure [1] . Whether IPT also has the potential for recurrence or metastasis, as described in reports on IMT, is unclear [2] . Local recurrence of IPT has occasionally been reported [6] ; therefore, careful long-term follow-up is needed even after macroscopically complete resection.
4. Conclusion
Our case suggests that IPT should be considered in the diagnosis of an anterior mediastinal mass with a high SUVmax on FDG-PET.