Use of Social Media for Health Communication Campaign in the Management of the Ebola Crisis in Beni-Butembo/DRC ()
1. Introduction and Background to the Study
The first outbreak of Ebola virus disease in the DRC began near the Ebola River in Equateur Province in 1976. Its diagnosis was made thanks to the expertise of Dr Muyembe. It is characterized by a haemorrhagic fever. Indeed, the patient dies of haemorrhage. The first outbreak of Ebola virus disease (EVD) in 1976 near the Ebola River in Equateur Province demonstrated the fatal nature of haemorrhagic fever. During this outbreak, examples of haemorrhage were alarmingly apparent. Many patients exhibited symptoms of internal bleeding, resulting in organ dysfunction, while others suffered from external bleeding from the gums, nose, and injection sites (Mjumbe, Omba, Ilunga, & Nuymbi, 2020) . These symptoms not only exacerbated their condition but also illustrated the deadly nature of the virus.
Fast forward to the 2018 Ebola crisis in the Democratic Republic of Congo (DRC), which began in August in the North Kivu province and spread to the neighboring Ituri province. This outbreak offered further examples of the lethal impact of haemorrhage. The fatality rate was significant, with deaths frequently attributed to haemorrhage. Patients often succumbed to a combination of internal bleeding and multi-organ failure. For instance, there were reports of patients bleeding profusely from injection sites and natural orifices, leading to shock and death. The haemorrhagic nature of the disease also posed unique challenges in treatment. Medical teams faced difficulties in administering care, as they had to balance the management of bleeding with other severe symptoms (Aruna et al., 2019) .
The visibility of bleeding symptoms created fear within local communities, hampering containment efforts. This fear was not unfounded, as the disease became the second-largest Ebola outbreak in history, only surpassed by the 2014-2016 epidemic in West Africa (Bourgarel & Liégeois, 2019) . Thus, the examples from both the 1976 and 2018 outbreaks illustrate the grim reality that haemorrhage is a defining and often fatal characteristic of EVD. The challenges presented by this symptom go beyond clinical treatment, affecting community engagement and containment efforts. These instances highlight the necessity for ongoing vigilance, research, and international collaboration to manage and mitigate the devastating effects of this disease.
The Ebola crisis in the Democratic Republic of Congo (DRC) has been an ongoing concern for the country and the international community since 2018 (World Health Organization, 2019) . The outbreak began in August 2018, in the North Kivu province and spread to the neighboring Ituri province. This was the tenth outbreak of Ebola in the DRC since 1976, and it was the second-largest Ebola outbreak in history, surpassed only by the 2014-2016 epidemic in West Africa (Mulangu, Mbala-Kingebeni, & Mbaya, 2022) .
The outbreak in North Kivu and Ituri provinces was complicated by the ongoing armed conflict in the region, as well as local mistrust of health workers, misinformation, and community resistance to control measures (Aruna et al., 2019) . The epidemic was also exacerbated by the movement of people across borders, including between the DRC and Uganda. Despite the challenges, the DRC government, along with international health organizations, made significant efforts to contain the outbreak (Barry et al., 2018) . This involved deploying personnel to affected areas, setting up treatment centers, conducting contact tracing and surveillance, and implementing vaccination campaigns. However, the high number of cases and deaths, combined with the insecurity and resistance, made the response efforts extremely challenging.
In June 2020, the World Health Organization (WHO) announced the end of the Ebola outbreak in the DRC, after a total of 3481 cases and 2299 deaths were reported. The successful containment of the outbreak was largely attributed to the efforts of the DRC government, international partners, and local communities, who worked together to control the spread of the virus. The Ebola crisis in the DRC highlighted the importance of strengthening public health systems in countries that are at risk of outbreaks. It also emphasized the need for a coordinated and rapid response to contain the spread of the virus, as well as the importance of community engagement and trust-building in the control efforts.
The Ebola crisis in the DRC has been met with resistance and distrust from the population, fuelled by social media (Masumbuko, Underschultz, & Hawkes, 2019) . The reasons for this include the population’s long-standing insecurity due to kidnapping and massacres, neglect by the government in affected regions, and suspicion that the government and aid workers may be complicit in the epidemic. Additionally, ignorance and misinformation propagated by social media contribute to the problem. The resistance and distrust not only impede the effective fight against Ebola but also exacerbate the health crisis (Muzembo et al., 2022) . Attacks on aid workers and treatment centres have been reported, including the murder of a WHO doctor.
Thus, the study aimed to achieve three objectives related to the Ebola crisis in Beni-Butembo, DRC. The first objective was to explore the health communication campaign in the management of the Ebola crisis. The second objective was to analyze the use of social networks during the crisis. Lastly, the study aimed to suggest innovative ways to improve the communication campaign in the fight against the Ebola epidemic. The study was literature based. A literature-based study is one that is conducted by analyzing and synthesizing existing published works on a particular topic. This approach allows researchers to draw conclusions and make inferences based on the collective knowledge and findings of others. In such studies, the primary source of data is existing literature, including scholarly articles, books, and other published materials.
The use of social media in health communication campaigns has become increasingly prominent, and there are several compelling reasons for this trend. Social media platforms are accessible to billions of people worldwide. By leveraging these platforms, health communication campaigns can reach a diverse and broad audience, including those in remote or underserved areas. For example, a campaign promoting vaccination can utilize social media to disseminate information to various age groups and demographics, ensuring that the message reaches those who may not have access to traditional media. In addition, social media enables two-way communication, allowing for real-time engagement and interaction with the public. Health organizations can answer questions, address concerns, and provide personalized information. This interactive nature fosters a sense of community and encourages participation, making the health campaign more effective. For instance, during a mental health awareness campaign, individuals can share their stories and support one another through social media channels.
Further, compared to traditional media outlets, social media often provides a more cost-effective way to deliver health communication messages. This is particularly important for nonprofit organizations or campaigns with limited budgets. They can use social media to reach their target audience without incurring the high costs associated with TV or print advertising. Likewise, social media offers tools for monitoring and analyzing audience response in real-time. Health organizations can track engagement, assess the effectiveness of their messages, and adapt their strategies as needed. This ability to make quick adjustments helps ensure that the campaign stays relevant and resonates with its audience. In the era of information overload, misinformation regarding health matters can spread quickly. Social media can be a powerful tool in combating this by providing accurate and evidence-based information. Health organizations can swiftly correct false information and guide the public toward trustworthy sources.
Different cultures may respond differently to health messages. Social media allows for the segmentation and tailoring of messages to suit various cultural norms and values. This can enhance the relevancy and acceptance of health messages among different communities. Thus, the rationale for using social media in health communication campaigns is multifaceted and includes advantages in terms of reach, engagement, cost-effectiveness, real-time adaptation, combating misinformation, and cultural sensitivity. By understanding and leveraging these benefits, health organizations can create impactful campaigns that resonate with diverse audiences and contribute to the improvement of public health outcomes.
2. Problem Statement
The media (traditional or new), through journalistic practices (of professionals or amateurs), have always played the role of essential intermediary between people (Bulatova, Kungurova, & Shtukina, 2019; Koreman, Verboord, & Janssen, 2023; Sirois, 2021) . They provide, at the strongest need of interaction, the links between individuals (Burger, Thornborrow, & Fitzgerald, 2017) , up to creating a media culture (Requate, Goulet, & Pinson, 2019) by making information available in real time. However, the management of new media during the Ebola virus epidemic has given rise to infodemia (a contraction of the words information and epidemic), a phenomenon of misinformation (Gardère, 2021) that disrupts the informational ecosystem through the number, diversity, scale and impacts of the fake news conveyed. If we look at the information circulating through social networks and especially on digital media, we realise that it falls into two categories: potentially true information and potentially false information, referring to fake news.
The dialectic of truth and falsity in the era of the Ebola Virus epidemic is thus put into action here. In a health crisis such as Ebola, the informational stakes are high. In addition to the unproven official information transmitted by the traditional media, and in this case by the communication unit for the management of the Ebola virus epidemic, other sources are constituted as spatial relays of fake news on the same epidemic. Bourrier (2019) , speaking about the publication of the positive cases and the consequences that followed, argues that the management of communication in the campaign against Ebola was done differently between the traditional media, the communication units for the management of the epidemic and the social media. Social media has caused many people to doubt the existence of Ebola, the way it is being managed, while traditional media has generally preached the existence of the epidemic and praised the way it is being managed. How should this upheaval be managed, as it has caused the traditional media and the journalistic practices of the communication units for the management of the epidemic to lose their watchdog role, depraved by infodemia or disinformation (Gardère, 2021) ? How can official information be given credibility in front of a population in the grip of the infodemia?
3. Objectives
This article has three objectives:
1) Exploring the health communication campaign in the management of the Ebola crisis in Beni-Butembo/DRC;
2) Analysis of the use of social networks during the Ebola crisis;
3) Suggest innovative ways to improve the communication campaign in the fight against the Ebola epidemic.
4. Methodology
The literature-based study, which primarily relies on existing published literature rather than collecting primary data, was adopted in the research. This method allowed the researcher to collect and synthesize information from previous studies, books, articles, and other published literature, specifically focusing on secondary data related to social media posts during the management of the Ebola outbreak. While a literature-based approach offers a practical and cost-effective way to conduct research when primary data collection is not feasible, the lack of introduction to this specific method might raise questions about its appropriateness for the study in question. Without an explicit rationale or detailed explanation for choosing this approach, readers might be left without a full understanding of why this method was deemed suitable for the research objectives. Therefore, a clear introduction to the adoption of this method, outlining its strengths, limitations, and relevance to the research question, would enhance the credibility and comprehension of the study.
5. Findings
Based on our three objectives, we have formulated our findings under three themes, of which we present a summary:
• The health communication campaign in the management of the Ebola crisis in Beni-Butembo/DRC;
• The analysis of the use of social networks during the Ebola health crisis;
• Indications for improving the communication campaign in the fight against the Ebola virus epidemic.
5.1. The Health Communication Campaign in the Management of the Ebola Crisis in Beni-Butembo/DRC
Good communication is an open door to good understanding, and poor communication or lack of communication is a source of misunderstanding (Adler, Towne, & Shewchuck, 1991; Kurtz, Silverman, & Draper, 1998) . This leads us to analyse, understand and, above all, criticise the way in which the management of information by the response teams had created many misunderstandings among the population, and led to errors of judgment on their part from the start of the process. When they arrived in Beni territory, the response officers did not have time to contact the population and explain why they were there and what their mission was. They started to circulate and work straight away, without taking into account the lack of knowledge of the disease by the populations concerned. Some facts required them to talk to the population beforehand, and the fact that they did not do so did not fail to arouse doubts towards these new people, which had negative repercussions in the good management of the epidemiological crisis. The health communication unit in the response campaign such as the Ebola epidemic in Beni and Butembo had its shortcomings. It was sometimes characterised by gaps in information and disinformation that did not take into account the local context.
5.1.1. Communication on the Presence of Foreign Teams as First Lines of Response
At the beginning of the epidemic in Beni territory, it was necessary to bring in doctors who had already had to deal with the disease in other regions or other countries, so that they could pass on their experience to local doctors who had never had to treat Ebola. But as this had not been well explained to the population, they quickly misunderstood: “they had doctors from such and such a country, we wondered if we didn’t have doctors at home; these foreigners didn’t want the locals to take over the answer, given the salaries they were receiving”. Rather than explaining to the population why the presence of non-local doctors was necessary, the response communication unit focused on sensitising the population to accept that the disease existed and that it was necessary to work with the response team. As a result, the poor communication created a resistant attitude on the part of the local population and local doctors.
5.1.2. Communication on the Availability of Vaccines at the Beginning and Mid-Point of the Response
At the beginning of the response, vaccines were in very short supply, and only those at risk of contracting the virus were vaccinated, i.e. those who had been in contact with an infected person. However, once the vaccines were available in larger quantities, they could be administered to a larger population. This change in the situation, which had not been explained beforehand, a failure to communicate, created judgements among those who were supposed to receive it, and suddenly there was a clear resistance to it: “Before, we used to ask for the vaccine by ourselves, but we were refused it because it was expensive, now what has changed so that suddenly there is enough of it and it is imposed on everyone? So we are afraid, we are afraid that this vaccine will kill us (WHO Ebola 2020 report)”.
5.1.3. Communication about the Different Signs of the Disease
At the beginning of the awareness campaigns, the sensitisers, not speaking the local language, distributed leaflets and hardly spoke at all. On these leaflets, the sign of a person with Ebola was bleeding. That’s what people remembered. For them, there could only be Ebola if there was bleeding. With this kind of health communication, when a family had a sick person, who was diagnosed with Ebola without any bleeding, they concluded that doctors were desperate to inflate the number of people with Ebola to get funding, and declared those who were not sick: “When somebody dies in a centre, without bleeding, they say he died of Ebola, and they have to burn the body, the house and everything else, how do you explain that? It is enough to have a fever to diagnose an Ebola patient; yet when you have sick children at home, water on the head is enough to bring down the temperature in case of fever; but only you call the response, directly he will be declared affected, and then it is his death if he goes to the Ebola Treatment Centre.” (WHO Ebola 2020 Report). The population had not been made aware of all the warning signs of the disease, was defensive about any report of a case that did not show the symptoms as they understood them, and was quick to question the results of the screening centres.
5.1.4. Communication and Burial Procedures for Ebola Deaths
To avoid any risk of contamination, the burial of Ebola deaths was very specific and required the utmost rigour. It was called a dignified and secure burial. This practice did not correspond to the culture of the population. There should have been a lot of sensitisation to enable them to understand the reasons why this type of burial was unavoidable; but due to a lack of good communication, there was a lack of understanding: “People were dying as if they were in parks, we were not informed. At the funeral, instead of cooperating with the families, they imposed their way of doing things on us, which was not in line with our culture; we did not even involve a family member; people rebelled. Some of us even went to check after the burial if the body was really still there, because there were rumours that something had been removed from the body before burial, so they didn’t want any of us to be there.” (WHO Ebola 2020 report).
5.1.5. Communication of Results
On several occasions, people complained about the slow communication of Ebola test results; they complained that even to announce negative results, it took a long time and that nothing was communicated to calm their impatience. They could spend up to 3 days in complete uncertainty, leading them to conclude that the reason results were taking so long was that doctors intended to change the results and have a large number of positive tests to justify the funds they were using. These examples illustrate how the lack of or poor communication from the teams led to a kind of apprehension of the response by the populations, which led to mostly negative perceptions of them.
5.2. The Analysis of the Use of Social Networks during the Ebola Health Crisis
The elements in our possession were collected during the Ebola Virus Disease crisis in Beni and Butembo. Before analyzing them, we first present the context of the Ebola crisis.
5.2.1. Use of Social Media to Disseminate Health Information
Social media are used by the general population as a means of communication to maintain links with family and friends, discuss, disseminate information and learn. They are also considered a source of information on current events. Users send each other links to news sites, for example, or share information from these sites. From a public health perspective, a systematic review has documented the role that social media play in health information for the general public, patients and health professionals. The power of social media lies in their ability to empower users and provide them with a voice, as anyone with access to the Internet can publish or disseminate information (Househ, 2013) . The U.S. Centers for Disease Control and Prevention (CDC) talks about the “three Ps” of social media (personalization, presentation, participation) and highlights the characteristics that make them effective health promotion tools.
Because social media can be used to create personalized and tailored messages for target audiences, these messages can be delivered in multiple formats to a variety of users. Furthermore, social media enable and encourage the participation of users themselves in the communication process, which promotes two-way information exchange in an environment that has traditionally relied on the dissemination of information from the provider to the consumer. Social media can be used to disseminate information on many health-related topics, including contact information and hours of operation for flu vaccination clinics, beach closures and weather warnings. This real-time communication allows public health officials to use social media to convey seasonal messages such as warnings of extreme heat or high humidity, to promote activities such as open houses or free clinics, or to communicate with the general public in times of crisis.
The range of social media platforms allows information to be delivered in different formats (e.g., video or text) and to reach people with special needs. Facebook, for example, is used to share information and experiences related to health. Videos on YouTube enrich written information and add a visual aspect to it. Blog sites, on the other hand, allow individuals, including health professionals, to share stories, information and resources.
In sum, the benefits to health professionals’ use of social media include increased interactivity, the ability to share and personalize information, a greater number of sources of health information, a space where health issues can be discussed and shared with various audiences, and a modality for providing social, emotional or peer support to the public. Social media can also be used to link and “follow” similar organizations. “Following” other public health organizations allows an organization to receive their messages, which can then be forwarded to that organization’s subscribers (in Twitter vocabulary, this is called “relaying a twitter”). This creates a ripple effect and increases the reach of the message. There are benefits to “following” an organization in this way, such as receiving news and information about their activities that is constantly updated and can be disseminated to a wider audience. Other social media applications, such as Facebook and blog sites, offer similar benefits.
5.2.2. Analyses of the Uses of Social Networks during the Ebola Crisis
Social networks were used to disseminate information related to the health of the victims but also information on health structures, particularly the Ebola Treatment Centre (CTE), on the progress of treatment of patients and the administration of vaccines. The instantaneous nature of social networks allows messages to be transmitted to the population in real time.
1) Social Networks and Psychosis
During the Ebola crisis in Butembo and Beni (DRC), rumours about social networks have reinforced psychosis and made it difficult to raise awareness to resolve the crisis. It should be remembered that for some, Ebola does not exist or is a manipulation to decimate the population. For others, a “hidden hand” may be behind the epidemic. The response workers themselves are regularly accused of not really wanting to eradicate the epidemic in order to make money.
We’ve collected some posts on Facebook and WhatsApp that express this accusation, which is strengthening the resistance in the population.
Message 1.
From a WhatsApp group on 04/04/ 2019 this message talks about the non-existence of the disease.
Translation:
I don’t believe Ebola is a disease of animal origin as we are led to believe. Certainly there is a hand behind it.
This message shared by many would be based on the following:
A complete lack of trust in the administrative and state authorities.
The cancellation of the presidential elections in Beni and Butembo, officially because of Ebola,
Aiding and abetting authorities, the tendency is to believe in conspiracy theories.
Message 2
From Facebook this message talks about how the Ebola virus is spreading.
Translation:
At this point during the night, helicopters are flying over the Lubero territory at low altitude to inject the virus into the population.
The population does not trust MONUSCO. MONUSCO is also complicit because, according to the population, it maintains insecurity in the area.
Message 3
On April 17, 2019 at 22:13 The organization Congo chek in charge of good communication during the Ebola crisis, reacts from its site to this message by stating that the spread of Ebola is due to human-to-human transmission. This is through direct contact with infected body fluids and not by spraying the virus in toilets or helicopters.
Translation:
The Ebola virus doesn’t spray in the toilets in Butembo. The spread of the disease is mainly due to direct contact with infected body fluids.
Message 4.
Written on April 26, 2019 at 17:08 This message is another reaction from Congo Chek regarding the healing of Ebola patients, against messages that claim that Ebola Treatment Centres are “mouroirs”. We go there to die.
Translation:
A total of 394 people have already been cured since this epidemic broke out in our region before they left the Ebola treatment centers...
Message 5
It is a message that shows the complicity of white people and the Congolese government in the mutilation of genital organs as was the case during the kidnappings.
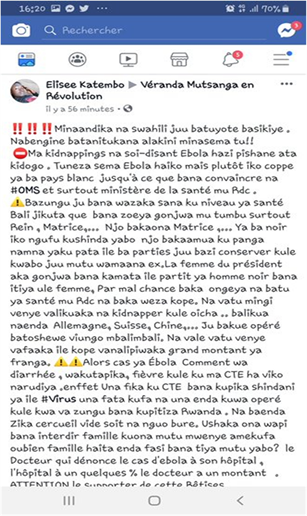
Summary of the translation:
I write in Kiswahili so that everyone understands my message. Even if others will rise up against me, at least I would have said so! There is no difference between kidnapping and so-called Ebola. We can affirm that Ebola does not exist, it is a “cooperation” initiated by the whites who manage to convince the OMS and the Congolese government, especially the Minister of Health, to play their game.
As white people think a lot about their health, they have noticed that they often have kidney problems and gynaecological problems for women. For this reason they need spare organs. This explains the kidnappings and the so-called Ebola.
Message 6
This message of May 5, 2019 incites to the fire of the Ebola Treatment Centres and the taking over by the population.
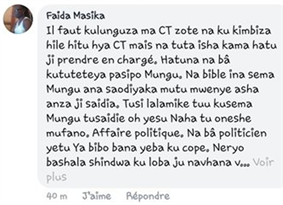
Translation:
We need to burn down every Ebola treatment center and kick out every agent in the response. If not, we’re the ones who die if we don’t take charge. We don’t have anyone advocating for us except God. Besides, the Bible says that God helps the self-helper. Let’s not beg for God’s help without showing ourselves willing to get out of this. This is a political matter. Our politicians are profiting at the expense of the people...
There are also so many posts on WhatsApp and Facebook that sow psychosis and fear of the disease among the population. It seems that in this case social networks are a real psychological weapon. However, they have been used to fight the spread of the Ebola virus disease crisis.
2) Patent interpretation
In the light of all the above, all the rumours that are sinking into psychosis concerning the Ebola virus disease have been amplified by the use of the social media. The resistance of the population is also to be subscribed in the same perspective. Fear and panic is the pitiful spectacle projected by social networks in times of Ebola epidemic. On the one hand, full of fake news and proposals to protect themselves against Ebola, and on the other hand, propelling rumours to staggering distances, community platforms shine by their ability to create disorder in the management of the crisis.
The UN representative in the Democratic Republic of Congo described the rumours circulating around the Ebola epidemic, which has killed more than 1100 people in the east of the country, as “total delirium” (Nkangu, Olatunde, & Yaya, 2017) . Indeed, the head of the UN Mission in Congo (Monusco) LeïlaZerrougui denounced “this story of total delirium” which consists in saying “that there is no disease, that they want to poison us by what they are making money on us”.
Social media have been the means of expression to support resistance but later on to foster collaboration with response teams to eradicate the epidemic. Through the same social networks, response organizations have persuaded victims with the collaboration of psychologists, religious leaders, etc., to join in.
As social networking platforms such as WhatsApp and Facebook are widely used by many people who own or have access to a smartphone and 3G service is available through the city’s major mobile phone operators: AirTel, Orange, Tigo, and Vodacom, members of the response community have also spread their messages to achieve their goal (World Health Organization, “eHealth at WHO”, World Health Organization, 2019 ). Social networks are a popular source of information. They are also a means of communication: a means of documenting what is happening in confined cities and keeping them connected to the outside world.
5.3. Indications for Improving the Communication Campaign in the Fight against the Ebola Virus Epidemic
Behaviour change cannot happen overnight due to interpersonal or environmental factors surrounding the individual. Behaviour change is a process that must enable the individual to change their behaviour. Physical stimuli, rational stimuli, emotional stimuli, skills, family and personal networks and social structures are some of the factors that can lead people to change their behaviour. Communication is an integral part of any public health action. It must be taken with care. In a 2013 report, WHO, in the context of controlling epidemics through behavioural impact communication, states that it underpins, and precedes, the actions taken by those affected or exposed and the interventions deployed in the response.
However, communication strategies are often designed after outbreak investigations and independently of operational decisions. As a result, communication has generally focused on message design and information dissemination. Behavioural impact communication is a planning framework and implementation method that integrates behavioural and social communication interventions into public health programmes. As such, it represents a profoundly new way of thinking about and implementing epidemic communication.
The risk of epidemics increases due to complex factors, including human behaviour. Effective communication, applied strategically, is therefore essential to influence the behavioural and social aspects of disease prevention and control activities. Behavioural and social interventions include a variety of multidisciplinary approaches, including the strategic application of communication for behavioural and social action. Huge sums of money have been spent on communication campaigns to prevent and control diseases such as highly pathogenic avian influenza, and currently Ebola and Corona. But for many of these communication programmes, the effects have not been clearly established, usually because of the gap between those who design epidemic control interventions (e.g. epidemiologists, veterinarians and public health specialists) and those who “communicate” and work to “mobilize” communities. Technical interventions need to be understood and applied in their behavioural, cultural, economic, political and social context, which is essential for successful control and prevention measures.
We share the view that health communication strategies have been used to educate individuals or groups to make the right decisions about the diseases that affect them by changing their behaviour. Behavioural models are used to help researchers understand behaviour and explain why people behave as they do. There are different psychosocial models that seek to explain human behaviour. The following are some of the models used in health communication. The health belief model (HBM) is the most widely used theory in health education and promotion. The health belief model suggests that people’s beliefs about health problems, perceived benefits and barriers to action, and self-efficacy explain engagement, or lack of engagement, in promoting health behaviours.
The Integrated Behavioural Model (IBM) is a combination of two theories: Theory of Reasoned Action (TRA) and Theory of Planned Behaviour (TPB). According to TRA, behavioural intention is created or caused by two factors: attitudes and subjective norms. Attitude and subjective norms determine a person’s intention to behave, with intention being the most important factor in determining behaviour. The Needs, Opportunities and Capabilities model focuses on environmental factors, which is relatively rare in psychosocial models. Similarly, the theory of planned behaviour examines environmental factors in the context of “perceived behavioural control”. This theory focuses on the role of perceived behavioural control as an influence on behavioural intentions and actual behaviour.
The theory of interpersonal behaviour builds on intention-based models by including external factors, such as habit, as part of the “enabling conditions”. This theory explains people’s behaviour in terms of what they have always done, what they think they should do and the consequences they associate with a behaviour.
While behavioural models are important, they also have their limitations. Models are deliberately simplified for ease of understanding and “do not take into account all the complexities of behaviour”. Most models do not segment the target population, but different factors are likely to carry different weight for different people. Mass media messages are disseminated through a variety of channels to promote or raise awareness of the need for behavioural change on health issues that concern the public. However, it is important to ensure that the correct information reaches a specific population and that the model has the potential to bring about positive change. Through education, people are informed about health issues and ways to improve and protect their own health, including more effective use of the health care system.
Health communication is a powerful and fundamental human interaction that can positively influence behaviour change in response to health issues affecting society. Interaction at the intrapersonal level, through the media, information and community engagement communication can increase knowledge, change attitudes and cultural norms and practices, and produce changes in health issues. Frequent health promotion is likely to cultivate the desired behavioural change resulting from the prevention of disease due to health-related behaviours. Behaviour change models have been used in the development of strategies to promote protection, reduce risk behaviours and encourage the adoption and maintenance of positive behaviours.
In addition, behaviour change models are used in the implementation and evaluation of interventions to change health-related behaviours, but they have limitations. Individual factors as well as societal factors contributing to behaviour may require a different approach to achieve a positive impact. Similarly, different behaviour change interventions can be applied to achieve a positive outcome. Efforts to change behaviour in society need to involve all stakeholders, including government, the community, health service providers, the media and non-governmental organisations (NGOs). People sometimes need frequent reminders and reinforcements that can be provided strategically if all parties involved are well coordinated and willing to work towards a common goal of positive behaviour change to prevent health problems.
For our part, specific channels for health communication need to be created in universities organising information and communication sciences, especially in DRC. Indeed, human health is more than a priority that requires no procrastination when it comes to safeguarding it. We believe that the communication limitations of the Ebola response are also due to the poor management of the relationship between the response agents and the communicologists who think that it is enough to broadcast the number of affected cases without measuring the psychological consequences on the rest of the population. This health communication should be based essentially on an ethic also based on the dignity of the human being.
6. Conclusion
Social networks have had a direct impact on the management of the Ebola epidemic. They are also being used as an effective means of communication because they can reach large numbers of people in real time. In other words, social networks are showing a newfound good faith in tidying up their sites—perhaps offering a glimpse of what the hybrid regulation that some, like Facebook, aspire to might look like—and more conspicuously referring their users to reliable official information. In this conclusion, we are left with the question: how can we ensure that in the event of an epidemic such as Ebola, stakeholders become truly active and responsible for their lives? In the first instance, it is through health communication that aims to change the behaviour of stakeholders. When you defend values and a model of society, you aim for change and you use different communication tools. Whether implicit or not, we also use tools of persuasion. For these to be effective, it is not enough to have good arguments, they must be linked to the values and attitudes of the target audiences and put forward low-cost commitments that reinforce their positive identities.
Above all, it is important to remember the value of non-frontal communication: seeing the target as sharing the same goals as ourselves, not as enemies. If we are less about convincing and more about getting people to make a concrete commitment to a cause, this is a completely different approach to communication: communication for health aimed at changing people’s behaviour. Oxfam-World Shops experienced this to some extent in 2016/2017 by campaigning to promote food alternatives without overemphasising the denounced crises and over-consumption behaviours, but rather by valuing the conviviality, the interest of all the alternatives that are currently emerging and their exciting character. That said, this brief analysis should not make us forget that it is global changes that we are aiming for through communication and that individual gestures and behavioural changes, even if they contribute to change, are not enough. Collective movements, politics and institutions must remain privileged targets if we want to defend a more just and sustainable society.
7. Recommendations
Based on the results presented in the essay, there are several recommendations that can be made to improve health communication during an epidemic such as Ebola. Firstly, it is essential to involve the local population in the response process from the beginning, explaining the reasons for the presence of foreign doctors and the importance of their expertise in combating the disease. Secondly, health communication campaigns should focus on providing accurate and comprehensive information on the disease, its symptoms, and the measures required to prevent its spread. This information should be disseminated using various channels, including social media, to ensure that it reaches a wider audience. Thirdly, health communication campaigns should be culturally sensitive, taking into account the local beliefs, values, and practices, to promote acceptance and avoid resistance. Finally, health communication campaigns should be continuous and involve regular updates on the progress of the response efforts, including the availability of vaccines, test results, and the impact of the response on the affected communities. By adopting these recommendations, health communication during an epidemic such as Ebola can be more effective in promoting behaviour change and preventing the spread of the disease.