Right Diaphragmatic Rupture with Passage of an Intrathoracic Ileal Segment Apropos of a Case and Review of the Literature at the Kankan Regional Hospital ()
1. Introduction
Traumatic ruptures of the diaphragm are tears due to trauma. They are often associated with a hernia of the abdominal organs (liver, stomach, intestine, spleen, kidneys). Infrequent, ruptures of the diaphragm can occur in polytraumatized people, mainly following a road accident.
A rupture of the diaphragm can be difficult to highlight in the acute phase, because its signs are not very specific and the imagery, which visualizes the ascended organs but more difficultly the rupture itself, can be faulted.
Right diaphragmatic rupture is rare and occurs in about 5% to 20% of all diaphragmatic injuries [1] . The incidence of herniation of intra-abdominal organs into the pleural cavity is low Düzgün AP et al. report 1.2% [2] . According to Hofmann S et al. in 2012, post-traumatic diaphragmatic hernia occurs more frequently on the left, because the diaphragm is more resistant on the right and it is more protected by the large surface of the liver. On average, 74.1% of patients have a lesion on the left (between 64.7% and 90% of patients depending on the study) and 4% of patients have a bilateral lesion [3] .
The objective of this clinical case is to study the physiopathological mechanisms, and to report our experience in the management of this condition.
2. Case Report
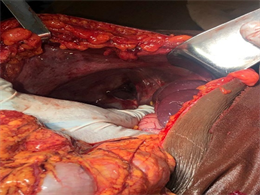
Patient M C., 40 years old, farmer and chronic smoker presenting with abdominal pain, nausea, stopping of matter and gas, abdominal distension, who was the victim of a public road accident (motorcycle). He consults three weeks later in a medical office where he was operated on for hernia of the white line and a right inguinal hernia; without improvement, he consults in our department for support. The examination showed an anxious patient, with good staining of the integuments and mucous membranes, distended abdomen, site of two recent sutured wounds; one supra-umbilical median sutured in 3 points, another oblique in the right inguinal region sutured in 4 points. The abdomen is painful, with tympanism in the epigastrium and the right hypochondrium. Cardiopulmonary physical examination was normal. The patient was eupneic, SpO2 was 99% on room air with a normal hemodynamic state. An indication for laparotomy was made. The patient benefited from a nasogastric sounding and a urethral catheter. It was taken under general anesthesia, a median laparotomy supra umbilical widened in sub umbilical was carried out, which made it possible to highlight a retro-distension of the hail upstream of the obstacle and flattened downstream.
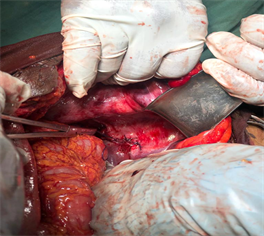
(Picture 1). The extrication of the small handles, three in number, of the right thoracic cavity through a breach of about 5 cm on the long axis of the right dome (Picture 2) showed a bruise at the level of the striction zone and a punctiform perforation at its free edge on the proximal side which leaked stools; the rest of the loop looked normal (Picture 3).
We proceeded to suture the breach of the right diaphragmatic dome and the hail wound (Picture 4). The postoperative course was marked mainly by the resumption of gas transit on the 4th day of the operation. On the 6th day of the surgical act, we noted parietal suppuration of the median wound above the umbilical which resolved in 10 days. The patient seen again a month later in a follow-up consultation returns in good general condition, without any problems, transit, nor respiratory distress to be deplored.

Picture 1. Hail distended upstream and flattened downstream before extrication.
Picture 2. Breach of the right diaphragmatic dome after extrication.

Picture 3. The area of ecchymotic ileal stricture and the loops that were incarcerated through the diaphragmatic breach.
Picture 4. Aspect of the right diaphragmatic dome after suturing.
3. Discussion
Diaphragmatic rupture should always be considered during a high-energy thoracic and/or abdominal trauma. The rupture mechanism consists of a sudden rise in abdominal pressure, up to ten times normal, following compressive forces [4] . Data from the most recent series show that ruptures of the right diaphragm can account for nearly 35% of all diaphragmatic injuries [5] . This is generally explained by the barrier role of the hepatic mass, and especially the fact that right ruptures are often associated with serious vital lesions resulting in death before arrival at the hospital [5] .
The main risks of a right diaphragmatic rupture are represented by insufficient diaphragmatic function, pulmonary compression, displacement of the mediastinum and reduced venous return [6] . Indeed, the ascended organs in the thorax cause a paradoxical elevation of the central venous pressure.
The preoperative diagnosis of diaphragmatic rupture is difficult. Twenty to 40% of ruptures are discovered during a laparotomy performed for another lesion because the clinical signs are inconstant and rarely specific [1] . In our case, the diagnosis could only be made intraoperatively given the circumstances and the postoperative context, which undoubtedly confused us. It is only intraoperatively that we have not only highlighted the diaphragmatic wound but also its consequences. Classical diagnostic means include chest X-ray, ultrasound, computed tomography (CT), magnetic resonance imaging (MRI). Chest X-rays have a relatively low sensitivity, but remain a screening tool with suggestive diagnostic results only in 17% to 40% of patients [7] . Rupture should be suspected in the presence of any marked elevation of the diaphragmatic dome with an intrathoracic hernia of the abdominal viscera [8] . Extended abdominal ultrasound above the diaphragm may be helpful for diagnosis. It makes it possible to observe the absence of movement of the diaphragm, the hernia of the viscera, or the planes of rupture of the membrane [6] . Helical CT is the preferred diagnostic modality due to its ability to acquire volumetric and good quality data from coronal and sagittal reconstructions [9] . CT, in right diaphragmatic ruptures, has a sensitivity of 50% to 90% and a specificity of 90% to 100% [1] [10] . MRI, currently unusable in the emergency context, provides information identical to that of the helical scanner, but with direct frontal and sagittal images and better spatial resolution [11] .
During the treatment of the lesions, the abdominal approach allowed us to treat the occlusion by extrication of the ileal loops, and the repair of the lesions on the hail and the diaphragmatic wound. At first, the abdominal route is the reference route. It allows the exploration and treatment of all intra-abdominal lesions.
According to Abdelkarim K [12] , when we are beyond 7 days and in the absence of intestinal lesions, the right thoracic tract with reintegration of the liver intra-abdominal and only repair by right diaphragmatic separate stitches.
4. Conclusion
Traumatic rupture of the right diaphragm, a rare condition, could only be diagnosed intraoperatively due to a lack of imaging means. The laparotomy made it possible to inventory and repair the lesions.