IGF2 ApaI A/G Polymorphism Evaluated in ESRD Individuals as a Biomarker to Identify Patients with New Onset Diabetes Mellitus after Renal Transplant in Asian Indians ()
1. Introduction
Insulin-like growth factors (IGFs) are regulators of processes like growth and metabolism. IGF1 and IGF2 contribute to pancreatic β-cell growth and development by regulating β-cell replication, renewal, and apoptosis [1]. Deregulation of balance between β-cell renewal and apoptosis due to alterations in IGF levels is potentially of great importance in the development of glucose intolerance, a major characteristic of diabetes. In addition, insulin-dependent glucose homeostasis may be affected by IGFs as they act via the insulin signaling pathway [2]. Defects in the IGF/insulin-signaling pathway affects birth weight and fat metabolism in both domestic animals and humans, which are known risk factor for development of Type 2 diabetes (T2D) [3]. IGF2 polymorphisms have been associated with weight gain, Body mass, obesity and adiposity [4].
Hence in the present study Apa1 polymorphism (rs# 680) has been evaluated in ESRD individuals who have undergone renal transplant to help identify individuals at a risk of developing new onset/Post transplant diabetes mellitus (PTDM).
PTDM or new onset diabetes mellitus (NODM) is a serious metabolic complication that may follow organ transplantation in patients on immunosuppressive therapy [5]. According to American Diabetes Association (ADA) criteria, 13% of patients develop NODM by 3 months after transplant and 39% in the long term have abnormal glucose metabolism [6]. Although there are currently no clearly established risk factors for identifying individuals who develop NODM, a number of characteristics have been identified that appear to predispose patients to the development of NODM. These are above 40 years of age, African-American and Hispanic populations, patient with a positive family history for T2D, increased BMI, hepatitis C virus infection and the immunosuppressive regimen [7]. The pathophysiology of NODM closely mimics that of T2D, both pathologies are characterized by a combination of insulin hyposecretion and insulin resistance [8,9]. TCF7L2, SLC30A8 and KCNQ1 polymorphisms have been studied in NODM which were earlier reported to be associated with T2D [10]. Increased activity of the IGF signaling pathway has been implicated as a major contributor to diabetic nephropathy, conferring the typical morphological appearance to diabetic glomeruli by virtue of its ability to induce characteristic changes and affect glomerular hemodynamics. Increased glucose levels in diabetics elevate IGF levels in the kidney. However, the association of IGF2 ApaI polymorphism with NODM has not been studied in any population.
Hence the aim of the present study was to evaluate the association of IGF2 ApaI polymorphism with ESRD and development of NODM after renal transplant.
2. Materials and Methods
2.1. Subjects
The present study was carried out in 364 Asian Indian individuals from a cosmopolitan city Hyderabad, located in South India. 140 of which were unrelated non-diabetic end stage renal disease (ESRD) patients who had undergone renal transplant and were on immunosuppressive therapy for more than three months, these individuals were on routine follow up and monitored periodically for renal function 42 of these developed NODM based on the ADA [11] criteria.
The control group consisted of 224 healthy volunteers, above the age of 40 years without T2DM or related health problems and who had a normal FBS. The study was approved by the Institutional Ethics Committees.
2.2. Sample
2 ml of peripheral blood was obtained from all the individuals included in the study along with a detailed clinical and family history recorded in a well designed proforma.
2.3. Isolation of Genomic DNA
Genomic DNA was extracted from leukocytes by a salting out technique which is routinely used in our lab [12]. The extracted DNA samples were dissolved in 0.1X TE buffer (pH 8.0) and stored at −20˚C till further use. DNA concentration was adjusted to 100 ng/µl before carrying out polymerase chain reaction (PCR).
2.4. Genotype Analysis by PCR-RFLP
A three step PCR-RFLP method was followed for IGF2 exon 9 ApaI genotyping, which has been published by our group [13]. Specific primers: forward primer: 5’- CTTGGACTTTGAGTCAAATTGG-3’; reverse primer: 5’-GGTCGTGCCAATTACATTTCA-3’ were synthesized by Bioserve biotechnology, (Hyderabad, India) for PCR analysis. DNA was denatured at 95˚C for 5 min, amplified by 35 cycles of 94˚C for 30 sec, 55˚C for 30 sec, 72˚C for 45 sec and the final extension with 72˚C for 5 minutes, 2.5 units of Taq polymerase (cat#MME27, Banglore Genei, Banglore, India) were used per reaction. PCR products were digested for 2 hours with ApaI at 30˚C (10 units of ApaI enzyme, 8 μl PCR product and 1.5 μl buffer in a final volume of 15 μl); and electrophoresed on 2% agarose gel with ethidium bromide.
2.5. Statistics
Genotype and allele frequencies were calculated for the described SNP (Table 1). The groups were compared using the χ2 test to analyze the statistical significance of the difference in allelic distribution of various polymorphisms in patients and controls. Values of p < 0.05 were considered statistically significant. Odds ratio was performed using MedCalc for Windows, version 7.4.1.0 (MedCalc Software, Mariakerke, Belgium).
3. Results
The IGF2 ApaI genotype and allele frequencies were identified based on the bands obtained after restriction enzyme digestion of the 292 bp PCR product. The A (not digested by ApaI) and G alleles (digested by ApaI) are 292 bp and 229 bp, respectively, heterozygotes were A/G (292/229 bp) at the ApaI polymorphism (Figure 1).
When the renal transplant patients were categorized as those who developed NODM and others who did not based on ADA criteria it was observed that 30% of the renal transplant recipients developed NODM. The IGF2 genotype in individuals with NODM was 26.1% AA and 73.8% AG, while non-PTDM group consisted of 56.1% AA and 43.8% AG. NODM cases showed a significant difference for the G allele and AG genotype
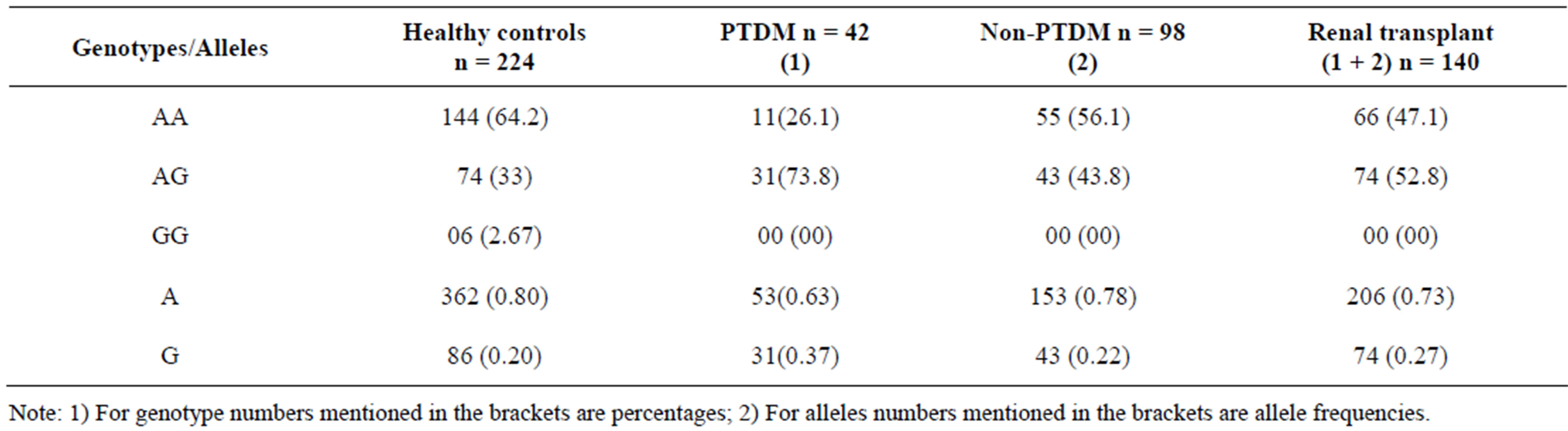
Table 1. Genotypes and alleles distributions of the IGF2 ApaI polymorphism in each of the cases studied along with matching controls.
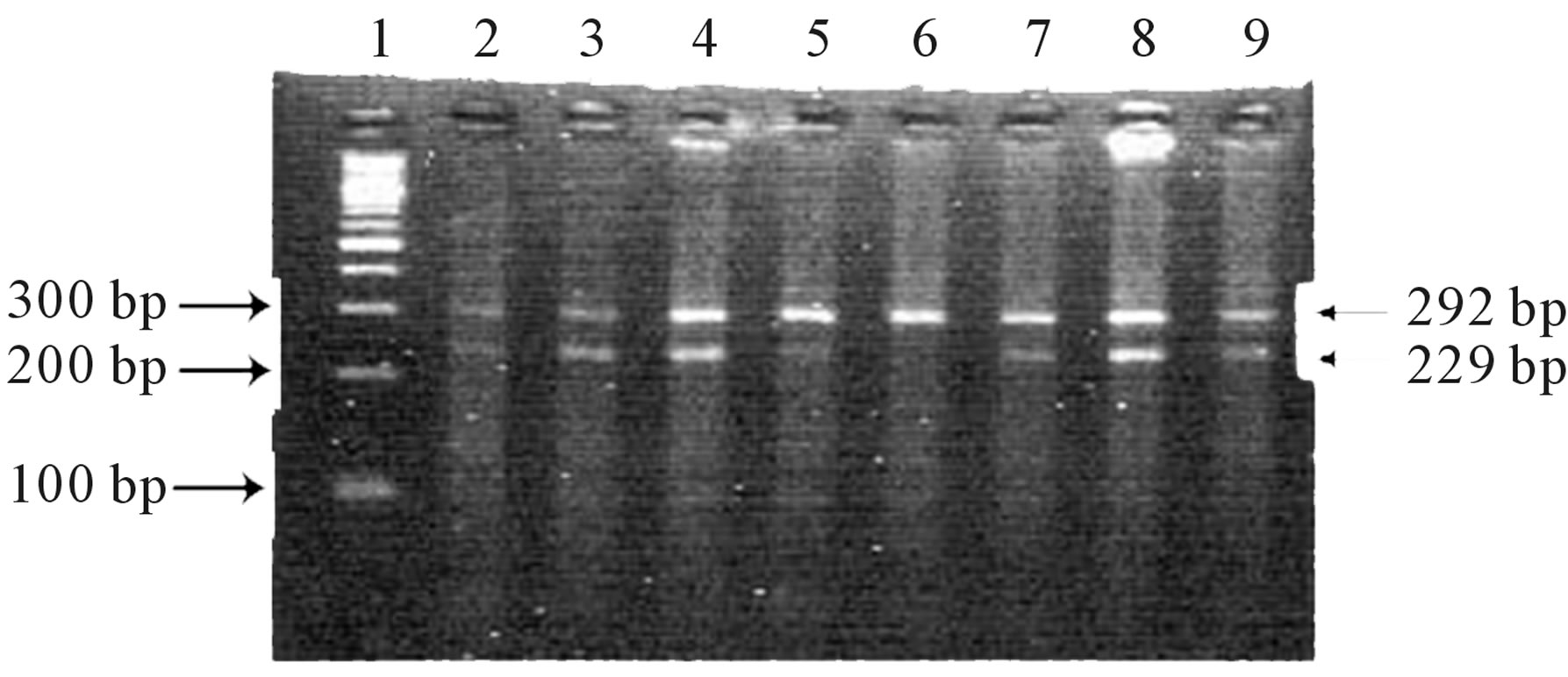
Figure 1. IGF2 PCR products were resolved by gel electrophoresis on 2% agarose gel stained with ethidium bromide after digestion with Apa I restriction enzyme. Lane 1: 100 bp DNA ladder, Lanes 2 - 5 & 7 - 9 showing 292/229 bp bands indicating heterozygous AG genotype, Lane 6: showing 292 bp band indicate homozygous AA genotype.
when compared to the ESRD patients (p = 0.01, p = 0.002) There was an association of NODM with G allele (OR 2.082, 95% CI = 1.191 and 3.634 AG genotype; OR 3.188, 95% CI = 1.498 - 6.785) (Table 2), which was significant. However, it was noteworthy that neither NODM nor the Non-NODM patients had the GG genotype, hence we compared ESRD patients who had undergone renal transplant with normal healthy controls. The G allele and AG genotype (p = 0.02, p = 0.0002) showed a significant association with ESRD (OR 1.512; 95% CI 1.060 - 2.155) and (OR 2.235, 95% CI = 1.453 - 3.438) respectively (Table 2).
4. Discussion
Several lines of evidence support that the susceptibility to NODM has a genetic component similar to Type 2 diabetes. Although no systematic studies have evaluated this, family studies suggest that NODM aggregates within families with a history of T2D [14]. Previously, it was shown that polymorphisms in the IGF1 and IGF2 genes are associated with features of the metabolic syndrome [15-18]. Gene variants in the IGF2 gene were found to be associated with IGF2 levels and BMI [16, 17]. Gomes et al. [19] (2006) studied the association between IGF2 ApaI polymorphism and the BMI, however, did not find any significant association.
In the present study ApaI IGF2 polymorphism was assessed out and it was identified that NODM showed an association with AG genotype and G allele (Table 2) when compared with controls i.e. normal healthy individuals and non-PTDM. GG genotype was completely absent even in the ESRD patients (includes both PTDM and non-PTDM) this was surprising as none of the ESRD cases included in the study were diabetic or had diabetic nephropathy, which has association with IGF2 in an earlier paper published by us Movva et al. [20] (2009). These ESRD patients showed a significant association with both AG genotype and G allele, indicating that both diabetic and non-diabetic renal disease were associated with IGF2 ApaI polymorphism. Similar studies in other populations are required to understand if this polymerphism has a role in ESRD in all ethnic groups or this is specific to the Asian Indian population.
NODM is a metabolic disorder that develops in response to a relative insulin deficiency in patients after organ transplantation treated with immunosuppressive drugs. From our study on 140 RT patients 30% were identified as PTDM. The onset of PTDM is most pronounced in the first few months after transplant and continue to present with PTDM at a steady rate after the first year post transplant. Our results suggest that IGF2 Apa I genotyping of patients is a possible method of predicting a patient’s risk for developing PTDM and would be a valuable asset in selecting appropriate immunosuppressive regimens for these individuals.
In conclusion our study for the first time shows that IGF2 ApaI G allele increases the risk of developing renal disease in Asian Indians and it can be used as a biomarke for identifying individuals at a high risk of developing NODM especially in case of RT recipients for appropriate management with immunosuppression to prevent the development of PTDM.
5. Acknowledgement
We acknowledge to the Dept of Nephrology of Kamineni
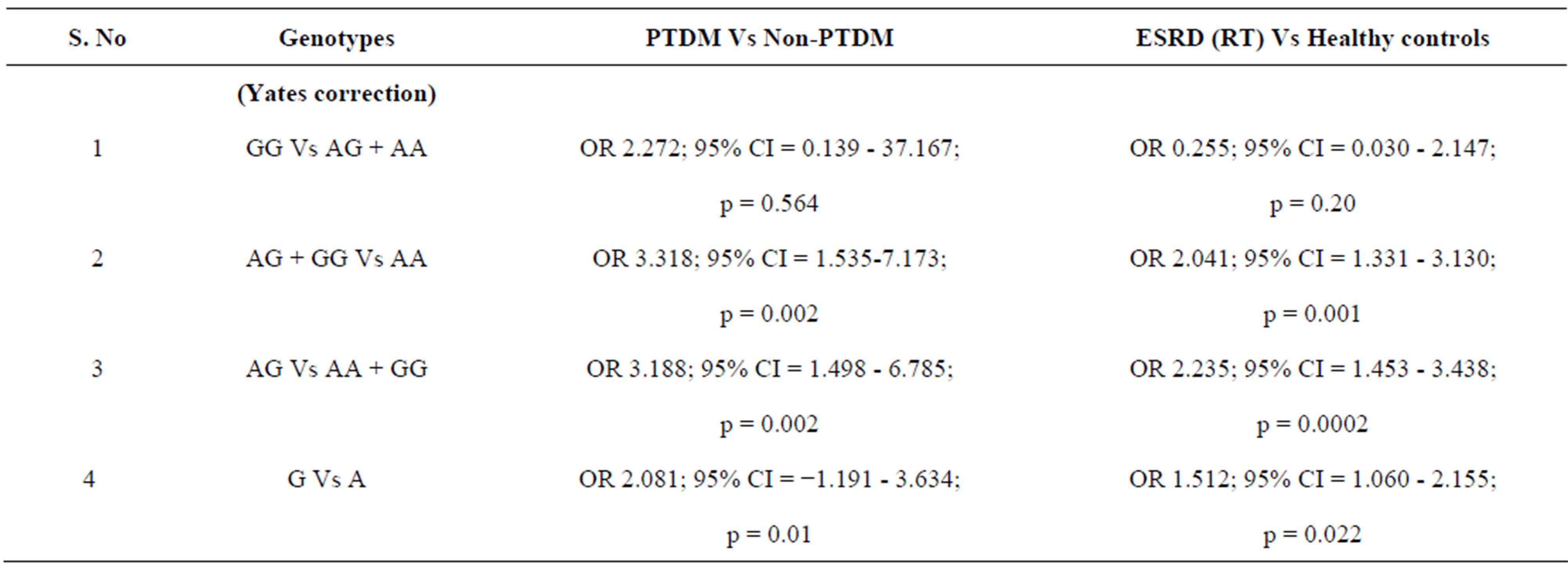
Table 2. Odds ratio and chi square test in IGF2 ApaI allele and genotype distribution in PTDM Vs non-PTDM and ESRD (RT) Vs Healthy controls.
Hospitals for providing samples, we would like to thank Indian Council for Medical Research for funding the project (Sanction No. 5-3-8-39-2007; RHN), we would like to thank who all participated in the study.
NOTES