Frequency and Determinants of Peripheral Neuropathy in Diabetic Children in Sohag, Egypt ()
1. Introduction
Type 1 diabetes is a chronic metabolic disease characterized by absolute insulin deficiency, resulting from a T cell-mediated destruction of pancreas B cell. It is considered one of the most common endocrine diseases in childhood and constitutes 5% - 10% of patients with diabetes [1] . The annual incidence of T1DM varied from 0.61 cases per 100,000 populations in China to 57.6 cases per 100,000 in Finland [2] . Middle East region, Saudi Arabia and Kuwait have the highest incidence rate at 31.4 and 22.3/100,000 per year [3] . In Egypt, the prevalence of type I diabetes in adolescents was 0.6% and there is growing epidemic of diabetes among children and adolescents [4] .
Diabetic neuropathy is known as a set of varied clinical syndromes with sensory, motor, and/or autonomic nerve fiber dysfunction, although the most common type is symmetrical distal sensory polyneuropathy (DPN) [5] . Diabetic peripheral neuropathy (DPN) is a common complication of T1DM, and unlike adults, patient’s polyneuropathy has no clinical manifestations in diabetic children in its early stages [6] . Clinical examination had less sensitivity and specificity than nerve conduction studies, which serves as a gold standard to detect subclinical neuropathy in these patients [7] . DPN is a major cause of morbidity and poor quality of life in patients with diabetes mellitus. It can increase the chances of other complications, namely amputation and foot ulcer [8] .
Abnormalities of nerve conduction are common findings in children with diabetes. The prevalence of DPN in both adults and children ranges between 7% and 57% (8 m), and the highest prevalence for DPN is found in children and adolescents with poor glycemic control and longer duration of diabetes, abnormal lipid profile, which are considered important risk factors for DPN [9] [10] .
Patients with TIDM have subclinical neuropathy long before occurrence of evident neuropathy, Moreover once symptoms appear, there are few effective therapeutic strategies [11] [12] . This indicates importance of early identification of DPN, in its primary stages to prepare appropriate measures to prevent its development. However, few studies have evaluated the subclinical neuropathy in these patients, and also the prevalence of early stages of DPN among children and adolescents is not well-known.
The aim of this research was to evaluate the prevalence of DPN (both clinical and subclinical subtypes) and its possible risk-factors in children with insulin dependent DM.
2. Material & Method
2.1. Study Design
This is a cross sectional study conducted to determine prevalence and determinants of DPN in diabetic children presented to Pediatric department in one year duration extending from October 1st 2016 to September 30th 2017.
2.2. Setting
Pediatric Neurology, Endocrinology Outpatient Clinics and Pediatric Department, Sohag University Hospital.
2.3. Study Population
All patients from 5 to 18 years suffering from diabetes mellitus type 1 for more than one year presented to Neurology and Endocrine Outpatient Clinics during the period of the study were included in this study. Exclusion criteria included: diabetic patients with duration of diabetes less than 1 year, age younger than 5 years old or older than 18 years old, children with other chronic diseases, handicapped children, children with cancer, chronic renal impairment, or other neurological diseases and children who were on medications that can produce peripheral neuropathy, i.e. antineoplastic drugs. Accordingly 50 patients were included in the study.
2.4. Data Collection Procedure
Predesigned questionnaire was filled by the investigator from the child or his parents. The first section of the questionnaire included in addition to socio demographic data of the studied child (age, gender, parental consanguinity and residence), detailed clinical data with special reference to (age of onset, duration and complications of diabetes mellitus, the presenting symptoms focusing on symptoms of peripheral neuropathy as numbness, tingling, loss of sensation, ulceration and Family history of diabetes mellitus and diabetic neuropathy.
The second section included data of patients examination focusing on neurological system as detailed neurological examination. Vibration perception, temperature sensation, pinprick sensation, MMT and ankle reflex were also examined in the participants. A tuning fork (128 Hz), Semmes-Weinstein monofilament test, cold and warm water test, and a reflex hammer were used for the evaluations. Neuropathy was evaluated through electrodiagnostic studies. The reference for evaluation and comparison of the electro-diagnostic parameters of sensorimotor responses were based on the tables from the “Electrodiagnosis in diseases of the nerve and muscle” and “electro-diagnostic medicine”.
The evaluation was done in a calm room with optimal lighting and temperature temperature was approximately 34 degrees Celsius, at the time of evaluation. The sensory nerves evaluated were the median, radial and ulnar nerves in the upper limbs, Sural and superficial peroneal nerves in the lower limbs. The methods used for the stimulation, recording, and analysis of the data were based on the standards of the books aforementioned. Nerve Conduction Velocity (NCV) and distal latency tests were performed in the following nerves: Common peroneal nerve, tibial nerve (motor), superficial peroneal nerve, and sural nerve (sensory) nerve in the lower extremities, as well as median (motor and sensory) nerves in the upper extremities, were observed in the tests. This section of the questionnaire included results of Hemoglobin A1C.
2.5. Ethical Consideration
Approval of Sohag Faculty of Medicine Research Ethics Committee was obtained. Written consent was obtained from the parents.
2.6. Statistical Analysis
The statistical analysis was carried out using SPSS software for Windows (version 22.0, Chicago, IL, USA). Sample characteristics were summarized numbers and percentage for categorical variables. Chi-Square test was used for comparison between qualitative variables. The associations between DPN and both duration of diabetes and HbA1c level was done using Mann-Whitney test.
3. Results
The mean age of the studied children was 10.5 ± 0.3 years ranging from 5 to 18 years. Among the studied 50 children having TIDM 22 cases (44%) were younger than 10 years, 27 children (54%) were females and 25 children (50%) were from urban areas. Family history of diabetes was found in 27 cases (54%), while positive consanguinity was detected in 20 cases (40%).
Among the studied children with type I diabetes 12% were diagnosed as having diabetic neuropathy as displayed in Figure 1. As regard the type of neuropathy, one case (2%) subclinical neuropathy, two cases (4%) had mild sensory axonal neuropathy, 2 cases (4%) had mild sensory motor axonal neuropathy, and one case (2%) had moderate sensory motor axonal neuropathy (Figure 2).
![]()
Figure 1. The percentage of neuropathy among the studied diabetic children.
![]()
Figure 2. Distribution of the studied diabetic children according to type of neuropathy.
As displayed in Table 1 no significant relation was found for age, gender, residence, consanguinity and family history and duration of diabetes and DPN. While highly significant association was found between DPN and Hemoglobin A1C.
Image 1: NCS show Rt. minimal sensory carpal tunnel syndrome (CTS) of a male diabetic patient 11 years old diagnosed 7 yeares ago was complaining of numbness and tingling in Rt. and Lt. hand, his serum creatinine was 0.8, and Hb
![]()
Table 1. Comparison between diabetic children with and without peripheral neuropathy as regard socio demographic characteristic, family history of diabetes, duration of diabetes and HbA1c level.

Image 1. Case no. (1).
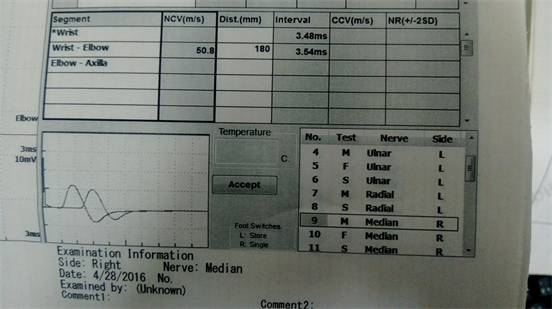
Image 2. Case no. (2).
A1c was 13 with normal fundus examination, diagnosed by NCS to have Rt. minimal sensory carpal tunnel syndrome (CTS) with impaired 2 sensory comparative studies on Rt. side.
Image 2: NCS show bilateral mild CTS more on Rt. Side of a male diabetic patient 16 years old diagnosed to have diabetes 3 years ago, was complaining of upper limb numbness and tingling and lower limb weakness, his serum creatinine was o.7, HbA1c was 12 with refractive errors and normal fund us examination, diagnosed by NCS to have bilateral mild CTS more on Rt. Side with comparative study done between median and ulnar nerve found that median nerve more affected than ulnar nerve (>0.6).
4. Discussion
DPN is a chronic complication of the diabetes that is rarely reported in children, since it has a relatively longer latency period [13] [14] . Our main objective in this study was to determine the prevalence of DPN among diabetic children and to assess the percent of subclinical neuropathy in addition to identification of possible risk factors of DPN among these children.
Our findings showed that 12% of the studied diabetic children had DPN. These findings are in agreement with [15] and [16] who reported a prevalence rate of 11% and 13.75%. However Effat et al., reported much higher prevalence (23%) among the studied children having TIDM [17] . Moreover Hollner et al. reported that the incidence of DN was 15% in symptomatic DN cases and 38% in DN cases diagnosed by NCS [18] . Their conclusion was that in type 1DM that is seen in children and adolescents, DPN had a higher prevalence rate; however, the majority of cases remain subclinical. But in our study the majority of diagnosed cases had symptoms of DPN in addition to their diagnosis by Nerve Conduction Analysis.
DPN can be classified into two broad subclinical and clinical stages. Based on results of previous studies, the prevalence of diabetic neuropathy in developing countries ranged between 10% and 68% [19] [20] and in Western countries, up to 60% of all patients with diabetes are affected by DPN [21] . However, the estimated rates of children are inaccurate, considering the prevalence of subclinical diabetic neuropathy observation in this age group.
Based on results of NCV and compared with clinical examination of the studied diabetic children, we found that 2% of diabetic children had subclinical neuropathy, they showed no symptoms or signs of neuropathy on clinical examination. On the other hands these cases of subclinical neuropathy constituted 16% of the total diagnosed cases of DPN. In agreement with our findings but with much more percentages of subclinical neuropathy were the findings of Toopchizadeh et al., who reported that among the diagnosed cases of DPN (57.5%) showed no symptoms of neuropathy [20] . Moreover, Nelson et al. [5] found subclinical neuropathy based on nerve conduction findings in 57% of Canadian children and adolescents with at least 5 years duration of T1DM. Baba and Ozaki found polyneuropathy using neurologic examinations in 43% of the studied diabetic children and using electro diagnostic studies in 63% of children and adolescents without clinical neuropathy [22] . These results indicate that, routine nerve conduction velocity (NCV) assessment for DN is beneficial in those patient groups [18] .
The lack of standardization of screening methods seems to be a general problem in diagnostic research on DPN There is considerable uncertainty about the prevalence of diabetic neuropathy (DN) due to a lack of large epidemiological studies and consensus on diagnostic criteria.
As regard factors associated with occurrence of DPN among the studied diabetic children, in agreement with [20] , no significant relation was found for age gender, residence, consanguinity and family history.
Association between DPN and duration of diabetes had been assessed and reported by many previous studies especially in adolescents and adults, however in children this association remains a matter of controversy. On contrary to [5] [23] , we found no significant association between duration of diabetes and development of DPN. Although these findings agree with [20] [24] [25] .
The level of glycaemic control in the studied diabetic children was unsatisfactory (a mean of 8.9 among the normal group and 16.2 among the group having DN). As recommended by the International Society for Pediatric and Adolescent Diabetes (ISPAD) a level of <7.5% (HbA1c) is crucial for a good metabolic control for all age-groups. As long-term good metabolic control reduces the total risk of complications in type 1 DM [26] . In agreement with our finding several previous researches [23] [25] [27] demonstrated that poor glycaemic control contribute significantly in development of DN among diabetic children.
5. Conclusion
Based on the results of the current study, subclinical peripheral neuropathy is frequent complication in diabetic children that related to poor glycaemic control rather than duration of the disease. This indicates the need for annual screening of neuropathy in children with TIDM using Nerve Conduction Study due to poor cooperation of these children as regard neurologic examination. Moreover, strict glycaemic control is needed to prevent rapid development of peripheral neuropathy and other complication among these children.
Limitation of the Study
The major limitation of the study was the reduced no of children with TI DM. This can be explained by the fact that NCA is a painful investigation that needs cooperation of the child. And many children refused to complete the test.
Questionnaire
Part I
1) Age: 2) Gender: a) boy b) girl
3) Parental consanguinity: a) Yes b) No
4) Residence: a) urban b) rural
5) Age of onset of Diabetes:_______
6) duration:
7) Symptoms of peripheral neuropathy: numbness, tingling, loss of sensation, ulceration
8) Family history of diabetes mellitus: a) Yes b) No
9) Family history of diabetic neuropathy: a) Yes b) No
Part II
Examination of neurological system:
10) Vibration perception:
11) temperature sensation:
12) pinprick sensation:
13) MMT and ankle reflex:
14) A tuning fork (128 Hz) examination:
15) Semmes-Weinstein monofilament test:
16) cold and warm water test:
Part III
NCV results of
17) Median nerve:
18) radial nerve:
19) ulnar nerves:
20) Sural nerve:
21) superficial peroneal:
21) results of Hemoglobin A1C: