Telemonitoring of Patients with Implantable Cardiac Devices to Manage Heart Failure: An Evaluation of Tablet-PC-Based Nursing Intervention Program ()
1. Introduction
Similar to that in Western countries, the number of heart failure patients has increased in Japan. Moreover, it is anticipated that this number will increase in the future [1] . If chronic heart failure is allowed to progress far enough, it becomes irreversible, resulting in repeated hospitalizations due to heart failure exacerbations. Repeat hospitalizations confer a major burden on patients, their families, and society, and limit patient roles and life expectancy, leading to distress [2] .
Meanwhile, heart failure treatments continue to evolve. The use of implantable cardiac devices, such as implantable cardioverter defibrillators (ICDs) and cardiac resynchronization therapy defibrillators (CRT-D), has become standard. Although implantable cardiac devices are beneficial for improving patient prognosis, many patients with such devices still require urgent clinic visits or rehospitalization due to aggravated heart failure, arrhythmia, and unexpected device problems. To solve these issues, remote patient management using implantable cardiac devices has been performed [3] . In telemonitoring, implantable cardiac devices continually record device and patient heart status and regularly transmit the information to medical facilities via the Internet. The aims of telemonitoring are to maximize outpatient visit efficiency, promptly detect situations requiring treatment, and ensure early treatment. Studies have shown that telemonitoring decreases the frequency of urgent clinic visits and reduces cost [4] -[7] .
Telemonitoring delivers data, such as heart rate, arrhythmia episodes, activity patterns, intracardiac pressure, and thoracic impedance, to medical staff without needing to interact with the patient. The lack of direct interaction may be a disservice to patients who struggle with self-care [8] . The telenursing aspect of telemedicine has evolved because it allows for the provision of both medical treatment and nursing care to a wide variety of people at reduced cost [9] . Telenursing has been associated with successful treatment of patients with chronic diseases, such as heart failure and chronic obstructive pulmonary disease [10] [11] .
Innovations in the field of information technology (IT) have advanced rapidly as well. Although telenursing was provided mainly via telephone and desktop personal computer (PC) in the past, novel information terminals are expected to become the predominant mode of interaction. In particular, the tablet PC is thought to be user-friendly because of its large screen and portability, especially for individuals who are not adept at using IT devices, such as women or the elderly. In this study, using tablet PCs as novel information terminals, we provided telenursing to support patients in their native environments by centering on interactive communication.
The purpose of this project was twofold. Our first aim was to develop a tablet PC-based nursing intervention program for patients requiring telemonitoring of implantable cardiac devices. The second purpose was to evaluate the efficacy of the program using a mixed-methods research approach.
2. Research Design
This study used a mixed-methods research approach that multifactorially clarifies phenomena by combining quantitative and qualitative data [12] . The two phases of the study are displayed in Figure 1. In phase 1, a tablet PC-based telenursing support program was developed according to the needs of patients with heart failure undergoing telemonitoring with implantable cardiac devices and based on findings of a literature search. In phase 2, an exploratory evaluation was conducted of the telenursing support program using an experimental implantation model [13] . In this experimental model, qualitative data are implanted into an experimental design. We conducted a randomized controlled trial, which served as a preliminary investigation, and interviewed the participants. These qualitative and quantitative data were combined to evaluate the program.
3. Phase 1: Modeling
3.1. Methods
In phase 1, a semi-structured interview was first performed among the patients with heart failure, who were un-
dergoing telemonitoring with implantable cardiac devices, to determine their needs. Simultaneously, a literature search was performed to determine which components of heart failure disease management were effective. Finally, the components derived from the literature were combined with the subject needs to develop the telenursing support program
3.1.1. Identifying Patient Needs
1) Data sample and collection The subjects were adult outpatients who had been discharged from the hospital at least 3 months prior to the study. The subjects were selected from all patients who had been identified as being high risk for rehospitalization by a physician and who underwent continuous telemonitoring with ICD, cardiac resynchronization therapy pacemaker (CRT-P), or CRT-D through the university hospitals within the metropolitan area of Japan. The study period was May 2010 to September 2010.
2) Ethical Considerations This study (phase 1) was approved by the study ethical committee of the Saitama Medical Center Jichi University. Study candidates who provided consent after being informed of the study purposes were considered participants. We obtained a signed consent form from each participant who received the written instructions and a verbal explanation, including reassurances that participation was based on their free will and their anonymity would be secured. We thoroughly explained that refusal of further study participation or withdrawal of study participation would not influence the medical or nursing care they were provided.
3) Procedure For participants who provided consent, a semi-structured interview was performed using an interview guide after outpatient visits. The contents of the interview consisted of thoughts about, understanding, acceptance, and expectations of telemonitoring. We used open ended questions: What do you think or feel about the telemonitoring? What are you expecting of the telemonitoring? Participants were allowed to talk freely. The contents of the interviews were recorded after we obtained each participant’s consent 4) Data analysis A thematic analysis was performed to determine patient needs for telemonitoring with implantable cardiac devices [14] . First, a verbatim record was made based on the recorded interview. After reading it repeatedly to understand the context, the minimum representation of “the needs of telemonitoring” was extracted from participant comments into a record unit. Second, the implications of each record unit were read and expressed in a single concise sentence as a code. The extracted codes were integrated for each participant, and then similar codes were integrated to extract a theme.
3.1.2. Identifying Effective Components of Heart Failure Disease Management
We conducted a literature search for the purpose of determining the effective components of a heart failure disease management program. Meta-analyses of heart failure published between 2005 and 2011 were searched using PubMed. The studies in which only drugs and exercise effects were evaluated were excluded. From the searched studies and guidelines, the effective components of a heart failure disease management program were extracted.
3.1.3. Modeled Process
The Health Belief Model [15] was used as a theoretical framework for development of the program. According to the Health Belief Model, the following six concepts influence activities for disease prevention and affect disease management decisions: perceived susceptibility, severity, benefits and barriers, cues to action, and self- efficacy. Patient needs (as determined from the qualitative survey) and the effective components of a heart failure disease management program (as determined from the literature search) were classified based on the six concepts of the Health Belief Model. Similar findings were integrated, from which the specific program contents were derived.
3.2. Results
3.2.1. Participants
The mean participant age was 63 years. There were more male participants (14 men; 78%). Five participants had an ICD, and 13 participants had a CRT-D (Table 1). The average interview duration was 30 minutes.
3.2.2. Telemonitoring Needs of the Patients with Heart Failure Using the Cardiac Device
The following four needs of patients with heart failure undergoing telemonitoring were extracted: “check the data by myself” (patients wanted to check their own data); “reminder” (patients wanted to have something that corrected their attitude that management behavior for heart failure tends to be neglected at home); “alert” (patients said they could live a life in peace at home if when an abnormality occurred, it was reported to their physician); “advice” (patients wanted to obtain advice from medical staff rather than just send in their data). As stated earlier, to live at home safely, the patients wanted information that would help them receive medical care at home.
3.2.3. Identifying Effective Components of Heart Failure Disease Management
We identified three publications and three guidelines. The contents of an effective heart failure disease management program consisted of frequent contact with medical staff [16] , self-monitoring [17] , daily assessment, patient involvement in symptoms, mental support [18] , and patient education [18] -[21] .
3.2.4. Modeled Program
The six concepts of the Health Belief Model are shown in the lower portion of Table 2. The following four elements are related to individual cognition: Perceived severity, Perceived susceptibility, Perceived benefit, and Perceived barriers. The other two elements, Cues to action and Self-efficacy, are related to action. We created

Table 1. Characteristics of participants.
the program to enable action by encouraging the desired cognition.
The needs of patients undergoing telemonitoring with implantable cardiac devices and the results of the literature search were classified accordingly. The contents of the program that satisfied these results are shown in the upper portion of Table 2.
To produce the desired cognition, people need to recognize the present condition and acquire the proper knowledge in the health belief model. If patients take interest in their data, they will better understand themselves and their condition. It is recommended that a health professional follow a patient to ensure the patient’s actions are in compliance with the literature and guideline. Therefore, one of the components of the program is monitoring. In addition, we included patient education in the program so that patients might acquire knowledge appropriate to their condition.
When patients perform a health-related action, that action must be preceded by a cause in order to raise selfefficacy in the health belief model. The following keywords indicate patients want a cue to action: Reminder, Alert, and Advice. Good feedback is more than just a reply; it gives the suitable cue to action for a patient’s present condition or raises self-efficacy. Mental support by a health professional bolsters the patient’s efforts.
The program had three components. The first component was monitoring, which was performed using a tablet PC, implantable cardiac device, and telephone. The participants used a tablet PC to send their body weight, blood pressure, and symptoms to the medical team from home. When the participants sent their data to the medical staff, they performed self-monitoring at the same time. A nurse confirmed the implantable cardiac device data (e.g., mean heart rate, impedance, and arrhythmia) via telemonitoring and called each patient once monthly to assess medication adherence, sleep, and mental status. The second component was patient education. Participants were asked to participate in e-learning to learn the basics of heart failure and implantable cardiac devices, and to learn about preventing heart failure. The educational contents were prepared using the Heart Failure Society of America education module [22] and the chronic heart failure treatment guideline [19] . To increase the attendance rate, the content was limited to 3 minutes per module. The third component was feedback of data to the participants. Nurses informed participants of their data as clearly and positively as possible twice a week. Participants were educated mainly on diet or fluid restriction as needed. The nurses used a tablet PC and telephone to communicate with the participants.
3.2.5. Study Program
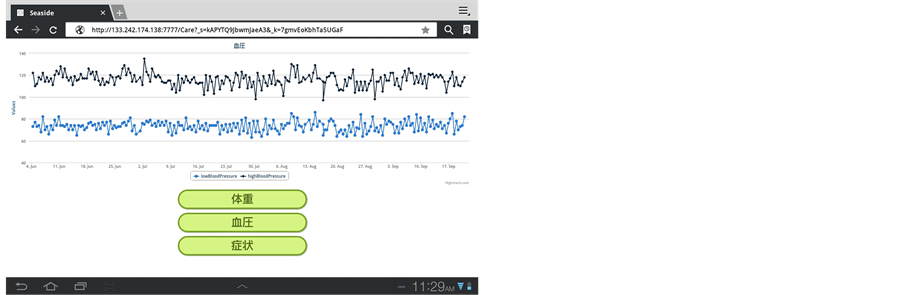
Cooperation between the patient, hospital, and university, as well as relationships between the telemonitoring system and the tablet PC-based telenursing support are shown on the left side of Figure 2. The online self-care website used in the study is shown on the right side of Figure 2. The website design was instinctive and inspired by an automated teller machine (ATM).
4. Phase 2: Preliminary Investigation
4.1. Methods
A mixed-methods study was performed to evaluate the effects of the program developed in phase 1. Participants were interviewed about their experience in order to acquire qualitative data.
4.1.1. Data Sample and Collection
A general hospital located in the medical service area in Japan was selected as the study site because it was in a medically underserved area, where the population would especially benefit from telenursing. The participants met all of the following criteria: adult outpatients undergoing continuous telemonitoring with ICD, CRT-P, or CRT-D; hospitalization due to worsening heart failure in the past year or a left ventricular ejection fraction ≤ 40%; and able to input data using a tablet PC (or the presence of a family member, who could perform the data entry). Participants in phase 2 were not included in phase 1. The 6-month study period (March 2012 to October 2013) included a 3-month intervention period and a 3-month follow-up period. Participants in the usual care (control) group were followed up on an outpatient basis by a cardiovascular specialist every 1 - 3 months.
4.1.2. Ethical Considerations
Phase 2 of this study was approved by the study ethical committee of the Kameda Medical Center. The procedure for obtaining informed consent was the same as in phase 1.
4.1.3. Randomization
We conducted a randomized trial. The participants were randomly assigned to the intervention and usual care groups and each provided informed consent [23] [24] . This method was adopted because it simplifies the process for obtaining consent for new treatments [25] , and the bias that might result from patient preference could be excluded [26] . Informed consent was obtained from the participants in both groups after randomization [24] . A minimization method was used for the assignment [27] . The assignment factors of the qualified participants were age at inclusion in this study (≤64 years old or ≥65 years old), sex, and device type (ICD or CRT-D).
4.1.4. Measurements and Variables
The outcome measures were as follows: rehospitalization rate, urgent clinic visits rate, quality of life (QOL), self-efficacy, and self-care behavior for heart failure. For QOL, the SF-8 Health Survey (standard Japanese version) [28] was used. A higher score indicated better QOL. For self-efficacy, health behavior-related self-efficacy for the chronic disease patient [29] was used. A lower score indicated better self-care. For self-care behavior for heart failure, the Japanese version of the European Heart Failure Self-Care Behavior Scale [30] [31] was used. A higher score indicated better self-care.
4.1.5. Statistical Analysis
An intention-to-treat analysis was performed. Fisher’s exact test was used to compare the attributes between groups at program initiation. For ordinal scales, once the distribution of data was assessed using the Shapiro-Wilk test, either a two-sample t test or a Mann-Whitney test was applied according to the presence or absence of normality. To determine readmission and urgent clinic visit rates, the time period between study initiation and event occurrence was used as the target variable, while a survival analysis was performed using Kaplan-Meier
 (1)
(1)  (2)
(2)  (3)
(3)  (4)
(4)  (5)
(5)  (6)
(6)
Figure 2. Overview of the nursing intervention system and online self-care website. (1) Diagrammatic representation of the telemonitoring system used in the trial, (2) Tablet-PC set and E-learning, (3) Main page of online self-care website where participants send information about blood pressure, weight, and symptoms (e.g., breath shortness, palpitation, edema, and fatigue), (4) Review test, and (5) Blood pressure chart.
survival analysis according to the two groups. To analyze changes in each scale score, the Wilcoxon signed-rank test was used for intragroup comparisons, and the Wilcoxon rank sum test was used for intergroup comparisons. The SAS 9.2 statistical software (SAS Institute Inc., NC, USA) was used, and the significance level was set at 0.05.
4.1.6. Qualitative Data Regarding Patient Experiences
To study patient experiences during the program, data were collected by semi-structured interview following the intervention, and a thematic analysis [14] was performed. First, a verbatim record was made based on the recorded interview. Second, after repeated readings for familiarization with data, the representations associated with patient experiences of the telenursing support program were extracted. Third, we generated initial codes to describe the data extracted. Fourth, the codes were integrated for each participant, and then similar codes were integrated to search for a theme. Fifth, themes were reviewed, defined, and named. To ensure reliability, we made repeated checks, examinations, and corrections to ensure that each code and theme was suitably named by researchers.
4.2. Results
4.2.1. Participants
Forty patients met the study inclusion criteria: 23 and 17 were assigned to the intervention and control groups, respectively. Of the 23 patients who were assigned to the intervention group, 17 provided consent and six refused to participate in the study. The reasons for refusal were: “the current treatment is sufficient for me”; “I am too old to operate a personal computer”; “it seems to be troublesome”; and two patients stated “I am busy because of my work.” Three patients in the intervention group dropped out of the study for the following reasons: “I am busy,” and “I suffered a great psychological shock due to the sudden death of a relative.” Of the 17 patients assigned to the control group, 16 provided consent, 1 refused to participate in the study for lack of interest, and another participant did not complete the questionnaire and was therefore excluded (Figure 3).
4.2.2. Baseline Characteristics
Forty patients met the study inclusion criteria: 23 and 17 were assigned to the intervention and control groups, respectively. Of the 23 patients who were assigned to the intervention group, 17 provided consent and six refused to participate in the study. The reasons for refusal were: “the current treatment is sufficient for me”; “I am too old to operate a personal computer”; “it seems to be troublesome”; and two patients stated “I am busy because of my work.” Three patients in the intervention group dropped out of the study for the following reasons: “I am busy,” and “I suffered a great psychological shock due to the sudden death of a relative.” Of the 17 patients assigned to the control group, 16 provided consent, 1 refused to participate in the study for lack of interest, and another participant did not complete the questionnaire and was therefore excluded (Table 3).

Figure 3. Flow of participants throughout this study.
4.2.3. Unplanned Hospitalizations and Emergency Room Visits
The rates of urgent hospital admissions associated with the heart within 6 months after study initiation were 11% and 18% in the intervention and control groups, respectively. The rate difference was not statistically significant based on two different tests: the log rank test (p = 0.3017) and the Cox regression analysis using the intervention group as a reference (hazard ratio [HR] 0.82; 95% confidence interval [CI] 0.42 - 12.42; p = 0.3441). Within 6 months after study initiation, the unplanned consultation rates associated with the heart were 11% and 18% in the intervention and control groups, respectively. This rate difference also was not statistically significant based on the two tests: log rank test (p = 0.3179) and Cox regression analysis using the intervention group as a reference (HR 0.45; 95% CI, 0.26 - 9.52; p = 0.6172) (Figure 4).
4.2.4. QOL, Heart Failure Self-Care, and Self-Efficacy
The amount of change in each score based on the intervention time point was calculated and an intragroup comparison was performed. As shown in Table 4, the degrees of change were compared between the groups, but no significant differences were found.
4.2.5. Qualitative Data Regarding Patient Experiences
Fourteen participants in the intervention group, who completed the study, were interviewed just after the end of the program. The interview was performed for an average of 40 minutes. Table 5 shows that three categories were ultimately derived.
 (a)
(a) (b)
(b)
Figure 4. Kaplan-Meier curve depicting the probability of survival ((a) Hospitalization for heart failure, (b) Unexpected visit to clinic) between the 2 groups (experimental is a solid line and the control is a dotted line), censored at 180 days.
1) Getting a sense of safety Most participants reported developing a sense of safety through participation in the program. The participants who experienced multiple hospitalizations led a life of anxiety that may worsen. However, they felt safe, like being followed by an escort runner during program participation. The sense of security was strengthened by knowing that no abnormality would go undetected.
“In this program, I felt relieved when I received a message such as no arrhythmia was detected. I felt assured for 3 months of the study period. Even if the message indicated that a slight arrhythmia was found, I felt that my condition was understood. If something occurs or if I contact you, I can receive some reply or advice. In such aspects, I was very relieved.”
Table 4. Within-group comparison and between-group comparison.
Abbreviations: SF8, SF-8™ Health Survey; HADS, Hospital Anxiety and Depression Scale; EHF ScB scale, European Heart Failure Self-Care Behavior Scale; aHigher score means better QOL; bLower score means better self-care; cHigher score means better self-efficacy.
Table 5. Patient’s experience with the nursing intervention program via tablet-PC for remotely monitored patients with a cardiac device to manage heart failure.
2) Triggering a health behavior change Most of the participants were encouraged to change their health behaviors by participating in this program. Even if they felt some abnormalities, they lived in a place that was too far from a medical institution and tended to hesitate before contacting a hospital. However, they became sensitive to changes in their symptoms because their level of awareness was increased during their participation in the program. Their consultation behaviors were also promoted since they communicated regularly with the nurses.
“I was not motivated to call you only when I felt considerably abnormal, but since I called you every day, I think that I am now more likely to call you if I feel an unusual condition.”
When an abnormality in participant data was found, the attending nurse called the participant, who considered this call a warning and improved their behavior.
“My body weight increased to around 108 kg and I received a call. After that point, I watched my weight more carefully, and it returned to 104 kg.”
3) Feeling like a burden Some participants felt that participating in the program was a burden. Although the tablet PC was easy to use, they felt that sending messages daily was cumbersome. They also felt burdened by occasional problems that occurred with the tablet PC.
“I don’t have many things to do at home, but it is slightly troublesome that I have to send a message every day. As such, I decided to send a message once every 3 days.”
5. Discussion
In this study, a tablet PC program was developed, and its efficacy was examined through interviews and a review of the literature regarding the needs of patients undergoing telemonitoring with implantable cardiac devices. We hypothesized that program implementation might result in: early detection of abnormalities and mental support; reduced rates of readmissions and urgent clinic visits; and improved QOL or heart failure behaviors. However, our statistical data did not support these hypotheses. There seemed to be several causes for this. First, the program period might have been too short. The quantitative survey showed no positive results, while the qualitative survey indicated signs of behavioral changes in participants. For instance, participants who thought that measuring blood pressure and body weight was necessary, but did not measure them, developed healthy behaviors. Since behavioral change usually takes 3 months, we set the program period to 3 months. However, the lack of impact might be reflected by the end point because the program ended when behavioral changes started to happen.
Second, the results might have been influenced by the small sample size. QOL in particular did not improve, which seemed to be due to one of the following reasons: 1) patients in the intervention group had low QOL scores at study initiation; 2) events not associated with the heart occurred in several participants (e.g., cancer occurred or a family member’s health condition worsened). These possible causes might have influenced the overall results.
Most participants in this study were unfamiliar with IT; however, the continuance rate of the program exceeded 80%. Although participants used an unfamiliar information terminal, the continuance rate was high. A previous, representative, large-scale study investigated the efficacy of telemonitoring using a push-button telephone and automated voice for patients with heart failure [32] . Only 55% of the participants finished that study.
The difference in the continuance rate between that study and the present study seems to be attributable to differences in feedback. The provision of specific feedback in contrast to an automated response seemed to increase participants’ interest, which might have increased their motivation to continue the program.
In this study, we primarily communicated with the participants using a tablet PC. However, limited information was obtained, so face-to-face interactions might also be necessary. Many of these participants had no easy access to a hospital owing to distance or traffic conditions. Therefore, use of not only the current intervention but also video technology such as Skype to view the participant’s face may be effective.
Next, we examined the outcome measures, including unplanned consultations. However, one case in which unplanned consultation was used as the end point seemed to include trouble. In this case, in which a participant hesitated about whether a consultation was required for the present symptom, the intervention prompted the patient to act, thereby receiving an appropriate and timely consultation. It is preferable to avoid unplanned consultations whenever possible. If early consultation can prevent aggravation of symptoms, participants will benefit. In some earlier studies [33] -[35] , unplanned consultation was defined as one of the intervention outcome measures. Here, it seemed necessary to evaluate the intervention from different angles using multiple end points.
Although a positive result was not obtained, we cannot deny the validity of the entire program. The tablet PC, which has become widespread, is easy to operate and can be used by the elderly as well. Considering that this program showed a higher continuance rate, the aforementioned issues were improved and reexamined, which should contribute to future use in clinical practice. While society continues to age rapidly, the number of people who are cared for at home has increased. Therefore, in an institution with a wide medical service area such as that in this study, it will be necessary to examine the effects of the program with cooperation of home-visit nursing stations in the future.
6. Limitations
This study has some limitations. First, it had a small sample size, and a single institution, which was made clear in the results. Since patients with implantable cardiac devices did not increase in number as anticipated, the sample size estimated at the planning stage was not reached. Therefore, the statistical analysis has limitations. Second, elderly healthcare dependents were not discussed. There are many elderly people among heart failure patients so the implementation of a program through a caregiver or a visiting nurse must be considered. Third, the cost of the intervention program was not discussed. Cost is an important factor that deserves mention because medical costs are subject to restrictions. Cost should be examined further in future research.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgements
We thank the patients who took the time to participate in this research, as well as the clinical staff of the participating institutions. We are also indebted to Dr. Suzuki and Ms. Iizuka for their support in solving any administrative problems.
The Pfizer Health Research Foundation and Okawa Foundation provided financial support for this study.