1. Introduction
The shoulder is one of the large joints in the body, many disorders may affect the shoulder and cause morbidity and affect a patient’s lifestyle. Therefore, there are many shoulder scores out there in the literature, and to our knowledge, there are more than 40 different shoulder scores to assess pain and functional outcomes [1] [2] . M-CMS is one of the most popular tools all around the world especially in Europe [2] . It is easy to obtain by history and clinical examination and takes 5 - 7 minutes. Besides, it’s sensitive to the smallest change in the functional outcome by 95%. Also, several papers studied its psychometric properties [2] . Murley Score (CMS) was a major criterion to assess the shoulder health of an individual after getting treatment for a shoulder injury [1] . However, several inconsistencies were found in CMS including the lack of objective measurement, imprecise terminology and lack of a standardized methodology; therefore, the Modified Constant Murley Score (M-CMS) was adopted in order to get a more precise assessment of shoulder treatment and to evaluate the effectiveness of shoulder treatment provided to patients [2] . In addition, traditional CMS was based on scores of four different criteria including pain, range of motion, strength, and ability to perform routine tasks. Additionally, previously mentioned factors had scores that were based on information provided by patients [3] . In contrast, under M-CMS, areas of assessment were the same but the information was not only based on the information provided by patients but also from the use of different assessment tools. There are several studies that have been done in the past in order to assess the effectiveness of M-CMS and its validity when translated into other languages [3] . M-CMS has been culturally adopted and translated into Brazilian, Turkish, Danish and Greek [4] [5] [6] [7] but still the Arabic translation is not available. In these studies, multiple independent translators were used followed by an expert committee and the M-CMS was tested in the field and validity was assessed using statistical analysis. There is a need for an Arabic translation to help interpret the scores more accurately. Therefore, this study focuses on the translation and cultural adaptation of M-CMS in the Arabic language.
2. Materials and Methods
2.1. Modified Constant-Murley Score (M-CMS)
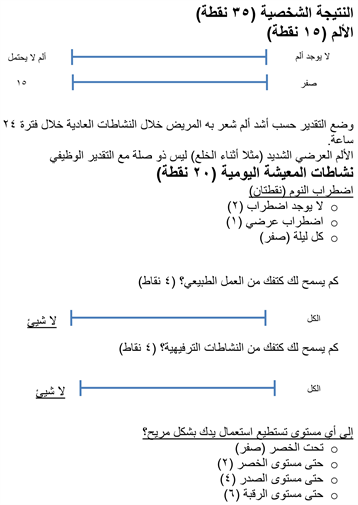
Terminology precision was lacking in the original CMS, therefore, it was criticized. As a result, CMS was modified and the modification was published in 2008 [8] . Under M-CMS, there are 100 points that can be scored by a healthy individual. However, the distribution of these points was that 35 points were given to subjective parts while the remaining was given to objective parts as per the instructions of the physician [9] . Furthermore, the study [9] stated that 4 different parts were selected under M-CMS including daily living activities, pain, strength and movement. Moreover, points were allotted differently for the four different parts; 15 for pain, 20 points for daily living activities, 40 points for movement and 25 points for strength.
Additionally, the bifurcation of points was different among each part because each and every part had sub-parts and the score was based on different activities under a single part of M-CMS. Under the 15 points of pain, points were distributed as the severity of pain that the patient felt over the 24 hours, this pain was measured using pain visual analog. On the other hand, points for daily living activities were distributed as two points were allotted to uninterrupted sleep, one point was allocated for occasional disturbance and zero point was given to disturbance in every night. Moreover, a 1 - 4 points additional scale was provided for reaction-based activities and work. However, the last 1 - 4 points were allocated for the amount of work and recreational activities that the patient can perform [9] .
In addition, 10 points were recorded by asking the patient about movement allowed by his/her shoulder. If the patient was comfortable to move shoulder above his head, 10 points were given. In contrast, if the movement was limited below the wrist, zero point was given. Furthermore, the movement was allocated 40 points, out of 40 points, painless forward elevation was given 10 points. Similarly, lateral elevation and functional internal and external rotation were also provided 10 points each. Finally, the remaining 25 points of the entire mechanism were allocated to strength [9] .
2.2. Translation Process
The process of translation and cultural adaptation followed previously published guidelines to assure validity [10] [11] , which is currently used by the American Association of Orthopedic Surgeons (AAOS) [12] . All translators were chosen based on their qualifications and suitability for the task. This process was done in five stages:
Stage 1: Initial Translation
In the first stage, two native Arabic translators who were fluent in English were given the responsibility to provide literal and conceptual translation of M-CMS. Between the selected two translators, one was an informed orthopaedic consultant who was aware of M-CMS while the other person was a blind English translator with a Bachelor’s degree in translation.
Stage 2: Synthesis of Translation
After the conversion from English to the Arabic language, an individual who was bilingual reviewed the instrument. Also, translators with Bachelor’s degrees in translation took part in this activity to identify any conceptual errors or inconsistencies. At this stage, a common translation of the instrument was developed.
Stage 3: Retranslation
At this stage, two speakers who used English as their first language while also having sound knowledge of Arabic were requested to translate the paper back into English from Arabic. However, the unique thing at this stage was that those English native speakers had no access to previously translated papers and they were unaware of the objectives of this study. Furthermore, the aim of this stage was to validate all items of M-CMS and to assure that the Arabic version was showing the same meaning.
Stage 4: Expert Committee Meeting
After the retranslation of the Arabic version of M-CMS, the third translator was incorporated in the system in order to review retranslated version of M-CMS papers to prepare for the expert committee meeting. Additionally, the committee consisted of a methodologist, a language professional and two orthopaedic surgeons. The aim of this meeting was to allow all members of the committee to compare the original, translated and retranslated versions of M-CMS and provide a pre-final version.
Stage 5: Testing the Pre-Final Version
King Khalid University Hospital was utilized in order to conduct a pilot test in the orthopaedic clinics. Moreover, the aim of this pilot test was to finalize the Arabic version. 41 patients were recruited in a randomized fashion. Those included in the study were adults, who came to the clinic either for pain or stiffness in their shoulder without a history of shoulder injury [11] . The patients were informed of the study design and those that consented were included in the study. Those patients were excluded who were having instability symptoms, recent shoulder (3 months) surgery or who were having a psychiatric illness. Patients were requested to come back after one week for a second assessment. On both occasions, researchers obtained and scored data, measured motion utilizing a standard goniometer and gauged power utilizing an isometric dynamometer. All these data were collected and inputted in SPSS.
3. Results
Apart from the qualitative aspects, quantitative statistical tools were also used in this study to assess the reliability, validity and relations between all four aspects of M-CMS. Therefore, three different statistical tools were used including a reliability test, Correlation analysis and Chi-Square test of association. Moreover, the purpose of the reliability test was to assess the reliability of data, on the other hand, the correlation test was used to analyze the relation between variables and finally, the chi-square test of association was used to assess the validity of data. Furthermore, data was collected twice: first, the data was collected in the Arabic version of M-CMS, and second time from the same patients one week apart by the same data collectors.
Reliability Test
Reliability test was done using Cronbach’s alpha, and results were as per Table 1.
a: List wise deletion based on all variables in the procedure.
It can be seen from Table 1 that there were 41 cases that were enrolled in the test, and all of them were valid, therefore, SPSS did not exclude any case. Moreover, Cronbach’s statistics were as per Table 2.
It was found (Table 2) that the reliability of data was around 0.872. Correlation analysis was used in order to assess the relationship between the four defined variables of the study. However, the data was collected in two different parts as stated above. Therefore, all variables of data were not included in the correlation test. We calculated subjective scores for daily living activities under which all criteria of daily living activities were included. Similarly, subjective scores were calculated for movement while strength was taken for the best attempt and pain was taken directly. Lastly, there were two inter-observer datasets set 1 and set 2.
After the application of correlation analysis, results in Table 3 were obtained.
From the results in Table 3, we can conclude that all variables were related. However, some were showing positive, and the rests were showing a negative association. But the aim of this test was to assess the association between variables of set-1 and set-2 to evaluate whether these variables were related or not. Therefore, similar variables among set-1 and set-2 were compared, for example, the pain in set-1 was compared with pain in set-2.
First, set-1 pain was compared to set-2 pain, and it was found that there was a 98.7% positive relation between them, which leads to the conclusion that the data of set-1 and 2 were highly correlated. Similarly, the next set was an activity of living subjective score set-1 and an activity of living subjective score set-2. When the comparison of these two variables was made, it was found that both of them were showing a 98% relation. The next attempt was made at the third variable, which was subjective movement score set-1 and set-2. When the relation was analyzed, it was found that the relation was very high and positive (98.6%).
The last comparison was made between set-1 strength best attempts and set-2 strength best attempts. The correlation for the mentioned set was analyzed and found it to be 100% correlation (1.00). Moreover, the relation between variables of set-1 and set-2 was analyzed in order to assess the relationship between variables of set-1 and set-2 separately. First, set-1 pain was compared to the activity of living subjective score set-1, and it was found that there was a 42.2% negative relation between them.
Then, set-1 pain was compared to the movement subjective score of set-1, and it was found that there was a 4% negative relation between them, which showed that the movement subjective score of set-1 and pain of set-1 was negatively associated. Moreover, set-1 pain was compared to the strength best attempt of set-1, and it was found that there was a 12.9% negative relation between them, which revealed that movement strength best attempt of set-1 and pain of set-1 was negatively associated.
Similarly, results for set-2 were assessed in order to find out the association between factors and variables of set-2. As a result, different outcomes were obtained, which identified new dimensions from the data. Later on, set-2 pain was compared to the activity of living subjective score set-2, and it was found that there was a 41% negative relation between them, which identified that the activity of living score of set-2 and pain of set-2 was negatively associated.
Afterward, set-2 pain was compared to the movement subjective score of set-2, and it was found that there was a 4% negative relation between them, which showed that the movement subjective score of set-2 and pain of set-2 was negatively associated. Moreover, set-2 pain was compared to the strength best attempt of set-2, and it was found that there was a 16.4% negative relation between them, which revealed that movement strength best attempt of set-2 and the pain of set-2 was negatively associated.
Finally, the statistical significance of all sets was analyzed and it was found that all of them were statistically significant. The stars were showing that the correlation is significant at 0.01 alpha. It means that the p-value of all variables was less than 0.01. In other words, it can be also said that the relationship was statistically significant at 99% alpha. Finally, from the correlation analysis, it was found that variables were related to each other and there were no differences occurred when data was translated. To assess the validity of data and assess the qualitative side of the relation between similar variable sets, the chi-square test of association was utilized and the results were as shown in Table 4.
The purpose of the chi-square test was to evaluate whether the variables of the study and data were valid or not. Since, it was assumed that if the variables are associated as per the chi-square test, the data and variables’ set are valid.
Finally, it can be seen from the results (Tables 4-7) of the chi-square test that the data was valid when the results of variables from set-1 compared with the results of the same variables from set-2. Also, it confirmed the relations between variables that were identified from the correlation test.
4. Discussion
The M-CMS was successfully translated and culturally adapted into Arabic following international recommendations. Also, in this study, we analyzed the relation between the four different variables of M-CMS, and it was found that the variables of M-CMS were correlated to each other and finally, it was revealed that all variables were valid and showed a significant relation.
a: 168 cells (100.0%) have expected count less than 5. The minimum expected count is 0.02.
![]()
Table 5. Activity of living subjective score Set-2 activity of living subjective score.
a: 272 cells (100.0%) have expected count less than 5. The minimum expected count is 0.02.
![]()
Table 6. Movement subjective score Set-2 movement subjective score.
a: 182 cells (100.0%) have expected count less than 5. The minimum expected count is 0.05.
![]()
Table 7. Set 1 strength best attempt Set-2 strength best attempt.
a: 22 cells (88.0%) have expected count less than 5. The minimum expected count is 0.10.
Moreover, the study focused on the reliability and validity of M-CMS when translated into Arabic from English and then retranslated into English. The validity and reliability of the version were tested and were found efficiently acceptable. The reliability test was done using Cronbach’s alpha and there were 41 cases that were enrolled in the test, and all of them were valid. Furthermore, it was found that the reliability of data was around 87%, which means that the data was reliable and can be used for further analysis. In comparison, the Turkish version had 87% reliability, Brazilian version had 85% reliability, and the Danish version had 94% reliability. Accordingly, all these translated versions were reliable.
Correlation analysis was used in order to assess the relationship between the four defined variables of the study. However, the data was collected in two different parts as stated above, therefore, all the variables of data were not included in the correlation test. We calculated subjective scores for daily living activities under which all criteria of daily living activities were included. Similarly, subjective scores were calculated for movement while strength was taken for the best attempt and pain was taken directly. As a result, the aim of this test was to assess the association among variables of set-1 and set-2 to evaluate whether those variables were related or not. Therefore, similar variables among set-1 and set-2 were compared, where pain, activity of living, and strength and it was found that there was approximately 98% positive relation between all of these variables in both sets in comparison to Turkish [5] 87% and Danish [6] 94%, which leads to the conclusion that data of set-1 and 2 is highly correlated. Finally, the statistical significance of all sets was analyzed and it was found that all of them were statistically significant.
The Chi-Square test was used primarily to analyze the validity of the variables’ set because the association was identified by the correlation above. Moreover, it can be seen from the results of the chi-square test that the data was valid because when the results of variables from set-1 were compared with the results of the same variables from set-2, the null hypothesis of the chi-square test (variables of set-1 and set-2 are not correlated) was rejected confirming the relation and validity of data. Also, it confirmed the relations between variables that were identified from the correlation test as in the literature [4] [5] [6] [7] . One of our study’s limitations was the lack of an isometric dynamometer of the shoulder in the institution, so the strength of the shoulder was measured through manual power grades.
5. Conclusion
M-CMS was successfully converted from Standard English to Arabic. No cultural adaptation was needed since M-CMS was easy to understand in our community and there was no difference in the terminology meaning between both cultures. Moreover, when the tool was retranslated, it provided the best results and showed that variables of set-1 and set-2 were valid, reliable and associated with each other. The previous analysis leads to the conclusion that whenever M-CMS is correctly translated into other languages, it gets successfully adopted by the culture and there is no negative impact on results. Also, it can be summarized that if M-CMS is further translated and culturally adopted into different languages, it will provide suitable results without disturbing its originality and significance.
Acknowledgements
Dr. Hind Alotaibi, assistant professor, English language and translation, languages and translation collage, King Saud University, who is participated in back translation of the Arabic version to English as part of the validation process. Dr. Reem Alsalem, assistant professor, English language and translation, languages and translation collage, King Saud University, who is participated in back translation of the Arabic version to English as part of the validation process
Ethical Approval
Permission to utilize M-CMS was electronically obtained from primary author. King Saud University institutional review board approved the research to be conducted at its affiliated hospitals.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Authors Contribution
SA, RB, AA and SA: Substantial contribution to the conception, design of the work; the acquisition, analysis, interpretation of data for the work and drafting the work and revising it critically for important intellectual content approved the final manuscript and agreed for publication. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Appendix