Aggression questionnaire scores in extremely violent male prisoners, male bodybuilders, and healthy non-violent men ()
1. INTRODUCTION
The long history of human violence is difficult—if not impossible—to explain with contemporary psychological theories. Even before television, toy guns, steroids, narcotics, alcohol and violent computer games influenced our daily lives, men killed each other. In the most ancient tribes, up to 25% of the male population were killed either by local or neighbouring tribe members [1]. Today, men commit most of the world’s violent acts reported to the police, and men are consequently overrepresented (85% - 90%) in prisons [2].
One of the key motives for extreme male—male aggression in the evolution of aggression appears to be the defence of status and honour. In addition, humans have an evolutionary history of sex differences as a contributory explanatory factor in human aggression [2]. A man’s sexual jealousy directed towards another man’s covetousness may also trigger extreme aggression and homicide [3,4]. A significant association between direct, mainly Physical Aggression and greater height, weight and strength, has also been described [5].
As long as 25 years ago, side effects from athletes’ use of anabolic-androgenic steroids (AAS) were recognised as a problem and were found to be increasing, also among non-athletes [6]. Since then, a large number of papers have been published on the adverse effects using AAS [7]. Aggression has been linked to bodybuilding [7], and some authors describe the perception of increased aggression by sports competitors as a desired effect [7,8]. Some studies of health club athletes have shown that 90% of the users of AAS report episodes of over-aggression and violent behaviour [9], whereas other studies do not support such associations [10,11]. After a 25-week study where 600 mg testosterone cypionate per week were given to the study subjects, no participants reported actual violence, but several described instances of uncharacteristic aggressiveness [12].
A more recent paper concluded that high doses of AAS may elicit neuropsychiatric symptoms among a minority of users [13]. However, subgroups of steroid abusers may have known psychiatric pre-morbidities that are likely to introduce bias into the suggested causal relationship between anabolic steroid abuse and neuropsychiatric effects. Studies have also shown a correlation between mental side effects and the severity of steroid abuse [14]. The neural systems underlying the aggression induced by AAS appear to overlap with the brain circuits responsible for the regulation of aggression by endogenous androgens such as vasopressin [15].
Several studies have pointed out that stable personality traits influence aggressive and delinquent behaviour [16]. A meta-analysis [17] found that trait aggressiveness and trait irritability influenced aggressive behaviour under both neutral and provocation conditions. Anger and Type A personality influenced aggressive behaviour only under provocation [18]. People with Antisocial Personality Disorder (ASPD) show greater increases in aggressive behaviour after consuming alcohol than people without ASPD [19], and there is a relationship between borderline personality (BP) traits and aggression, especially the reactive form [20].
The self-rating Buss-Perry Aggression Questionnaire (AQ) [21] is considered by many to be the gold standard for measuring aggression. It has been criticized, for example, for contamination of item and sum scores with social desirability responding (SDR) [22,23]. Despite the fact that the confounding effect of SDR has been found to be quite substantial across all items, it had only a minimal distorting effect when evaluating the extent of bias [22].
Factor analysis showed that the Buss and Durkee Hostility Inventory (BDHI) [24] covers four components of aggression: Verbal and Physical Aggression, Anger, and Hostility. There is a considerable overlap between the BDHI [24] and the AQ [21] which was developed later. Whereas the BDHI has been used, for example, to distinguish between violent and non-violent men and between delinquent and non-delinquent adolescents, the AQ [21] has been widely used to assess the subtraits of aggression and the patterns of their relationships with other variables.
A translated and validated Revised Swedish Version (RSV), based on the validation standard of the AQ [21] now exists (AQ-RSV) [25] for clinical use and research in the general population.
Bryant and Smith [26] introduced a 12-question refined measurement model (BS-AQ) of the original AQ [21] since the latter has low common variance and because of a confusing overlap between what the subscales actually measure. Bryant and Smith discourage basing the analysis of questionnaire responses entirely on the 29-item total scores because important distinctions may be masked.
This led us to investigate whether the AQ-RSV [25] and the BS-AQ [26] can distinguish between different levels of aggression in three selected groups of men: extremely violent prisoners, bodybuilders, and healthy men.
2. MATERIALS AND METHODS
The Norwegian Regional Ethics Committee approved the study (ID: 2010/792).
2.1. Study Subjects
2.1.1. Bodybuilders
13 bodybuilders, all men, were recruited from a gym in a suburban area of Oslo. They were actually recruited to participate in a larger study which also involved blood sampling. They were explained the aim of this study and agreed to participate and to declare their use of performance-enhancing substances in the way they found best. Table 1 shows the drugs and doses declared by the participants.
The mean age of the body builders was 41.6 ± 11.3 years, and the median age was 46 years. Screening for psychiatric illness showed none at the time of data collection.
2.1.2. Inmates
16 violent male inmates were recruited from a high security prison outside Oslo. They were actually recruited to participate in a larger study which also involved blood sampling. When blood sampling was mentioned when describing the study, some inmates were reluctant to participate, resulting in a low number of participants. The inmates were all serving longterm sentences, the majority in preventive detention. In Norway, such sentences are not associated with a specific term. The imposition of preventive detention indicates that the court considers the defendant at high risk for reoffending, and therefore as an imminent threat to society. According to Norwegian law, after having served a minimum term not exceeding 10 years, prisoners in preventive detention may ask the court to reconsider their case.
Table 2 shows the inmates’ ages and crime categories.
No serious mental illness was found when screening for psychiatric disorders. Applying the Hospital Anxiety and Depression Scale (HADS) with a cut-off set at 8 points, 5 of 15 inmates exceeded the cut-off for anxiety and 1 for depression. One questionnaire was not completed. The category sex-related violence included brutal violence, where the violent crime may have included rape, molesting or grievous bodily harm. All the inmates completed the AQ-RSV sitting alone in a room in the visiting area outside their departments in the prison.
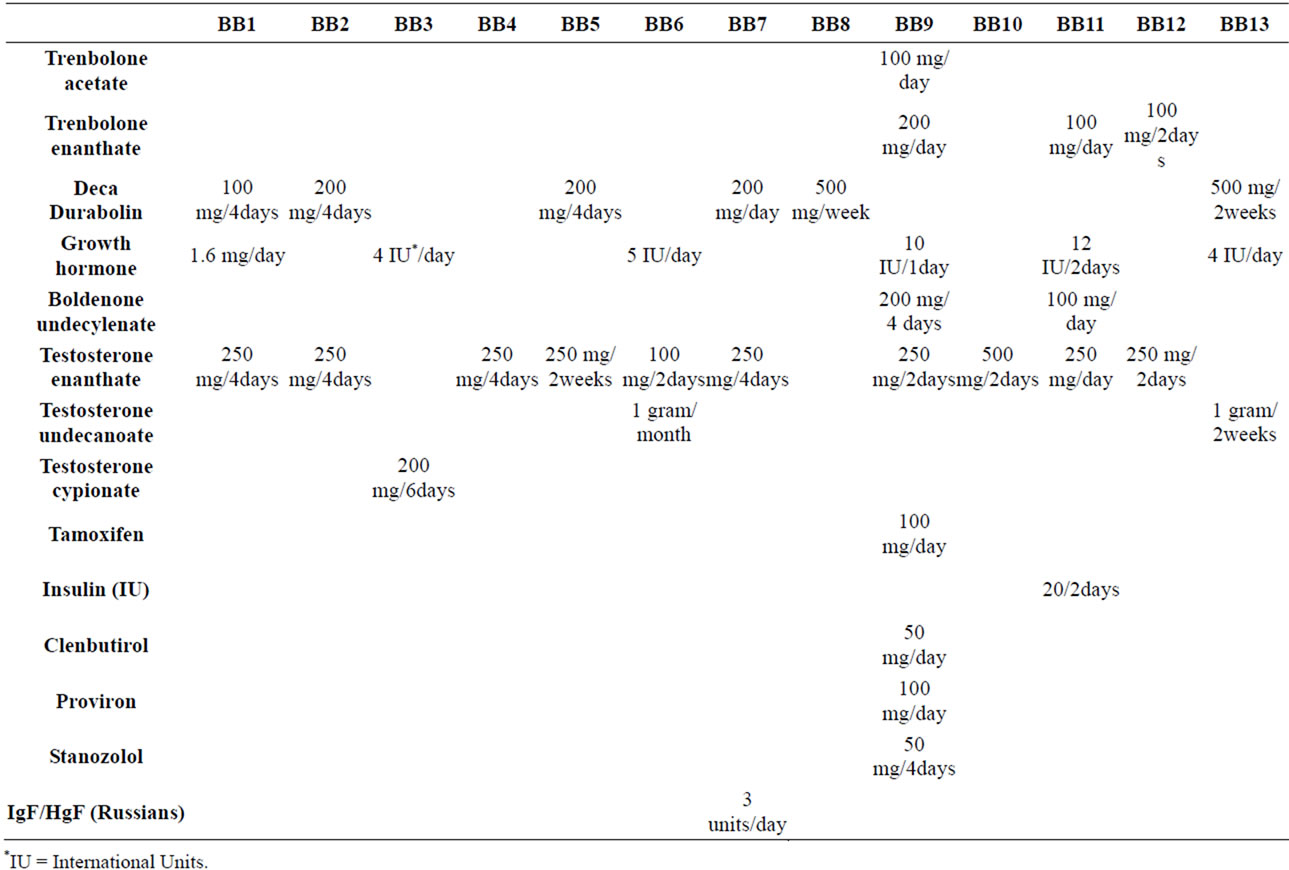
Table 1. Drugs and doses taken by bodybuilders (BB) (Where variations were declared, the highest dosage was chosen).

Table 2. Inmates’ ages and crime categories.
2.1.3. Non-Violent and Non-Steroid Abusing Healthy Men
The 21 control subjects were all men with no criminal record of aggression. They did not have any drug abuse problems and they were all working without restriction in society. In this paper they will be referred to as healthy men. Some were fish market workers, some hospital workers, and some held academic positions. They were actually recruited to participate in a larger study which also involved blood sampling. The mean age of the healthy men was 41.8 ± 10.4 years and the median age was 42 years. Screening for psychiatric illness showed no illness at the time of the data collection.
2.2. The Aggression Questionnaire—Revised Swedish Version (AQ-RSV)
The Swedish version of the AQ [25] was developed for research into clinical aggression based on the US American version of the AQ [21]. For validation, the test was mailed to 781 randomly selected individuals aged 20 - 40 years. Of these, 497 tests were evaluable (64%). The results with the American and the Swedish versions were comparable for the correlations between the four aggression subscales and alpha coefficients, indicating internal consistency.
The Swedish and Norwegian cultures and languages are very close, which means that the AQ-RSV can be directly applied in a Norwegian population. The AQRSV operates with cut-off values that classify the test subjects into three categories. “Normal” scores are between 0 and 39 points, “Elevated” scores between 40 and 68 points, and “Pronounced” scores between 69 and 87 points.
2.3. The Bryant and Smith Shortened and Refined Aggression Questionnaire (BS-AQ) [26]
For comparison with this scale [26], the 12 corresponding questions to those on the BS-AQ were identified on the AQ-RSV and the respective scores were selected for the analyses.
2.4. Statistics
SPSS for Windows, version 15.0.1 (SPSS Inc. SPSS 15.0.1-November 2006. SPSS for Windows, Chicago, SPSS Inc.) was used for calculating ANOVA and the t-test for independent samples. A p value ≤ 0.05 was considered statistically significant.
3. RESULTS
3.1. Aggression
3.1.1. Total Aggression
The AQ-RSV total aggression score for the inmates amounted to a mean of 40.4 ± 16.1. The corresponding values for the healthy men were 16.9 ± 7.3 and for the bodybuilders 25.5 ± 12.4. Both scores were significantly lower than in the inmates (p = 0.000 and p = 0.01 respectively). The difference between the mean scores in the bodybuilders and the healthy men was also significant (p = 0.01).
Applying the cut-off suggested by the authors of the AQ-RSV, i.e. normal between 0 and 39, all the total scores in the bodybuilders were normal except one “elevated”, and none of the healthy men had total AQ-RSV score higher than 39. Only 7 of the inmates scored higher than 39, leaving 9 within the normal range.
3.1.2. Aggression Subgroups
In Table 3 the total scores for the three groups are broken down into the 4 AQ-RSV subgroups of aggression.
Table 3 shows that a statistically significant difference in aggression was found only for the Physical Aggression subscale when comparing the bodybuilders to the healthy men (c). It is also evident that the inmates’ scores (b) reflected more aggression among the violent inmates than