Characteristics of HIV Infected Patients with Biopsy Diagnosed Spongiotic Dermatitis
Copyright © 2011 SciRes. WJA
148
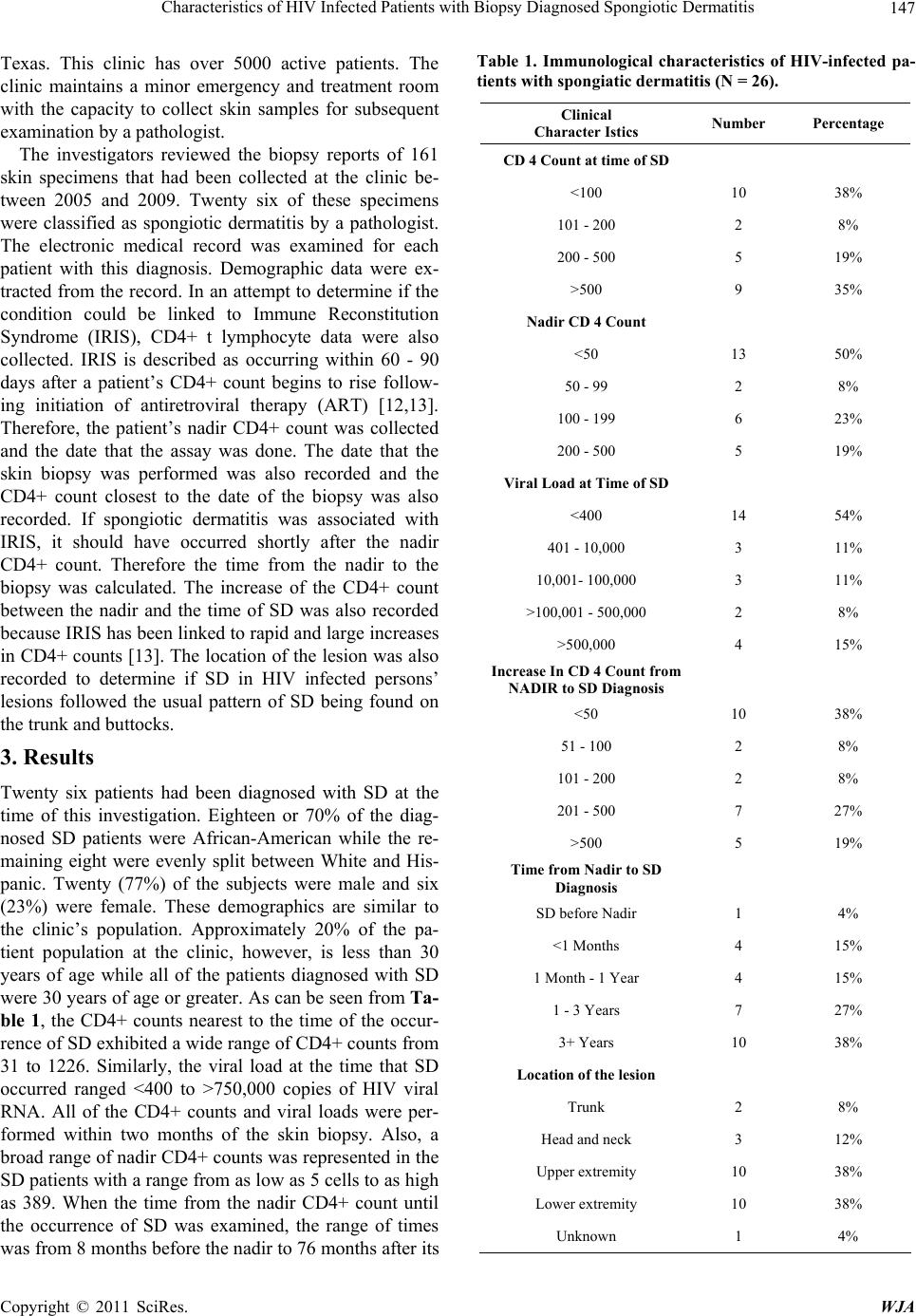
occurrence. The lesions tended to be located on the arms
and legs and only five patients had lesions that were lo-
cated on the trunk or the head and neck.
4. Discussion
This is the first paper that describes SD in HIV infected
persons. It seems that the lesion is not related to the im-
munological state of these patients nor does the level of
virus seem to be factor in its occurrence. Attempts to
relate SD to the time frame that is associated with IRIS
were not successful. Of note, SD in these HIV-infected
patients tended to be located on the extremities, not on
the trunk and buttocks as in non-HIV infected persons.
So, those who are treating HIV infected persons may
expect to see SD on occasion and it may appear in un-
usual body sites and at any time during the course of the
infection.
REFERENCES
[1] K. Gupta, “Deciphering Spongiotic Dermatitides,” Indian
Journal of Dermatology Venereolology and Leprology,
Vol. 74, No. 5, 2008, pp. 523-526.
doi:10.4103/0378-6323.44332
[2] M. Jeffries, “What Is Spongiotic Dermatitis?” 2010.
http://ezinearticles.com/?What-Is-Spongiotic-Dermatitis?
&id=1068322
[3] Gruppo Italiano Studi Epidemiologici in Dermatologia
(GISED), “Lichen Planus and Liver Diseases: A Multi-
centre Case-Control Study,” British Medical Journal, Vol.
300, No. 6719, 1990, pp. 227-230.
doi:10.1136/bmj.300.6719.227
[4] R. R. Bonamigo, K. Borges, J. Rietjens, S. Arenzon, L. P.
Blanco and R. Loureiro, “Human T lymphotropic Virus 1
and Hepatitis C Virus as Risk Factors for Inflammatory
Dermatoses in HIV-Positive Patients,” International
Journal of Dermatology, Vol. 43, No. 8, 2004, pp. 568-
570. doi:10.1111/j.1365-4632.2004.02179.x
[5] B. T. Summey, S. E. Bowen and H. B. Allen, “Lichen
Planus-Like Atopic Dermatitis: Expanding the Differen-
tial Diagnosis of Spongiotic Dermatitis,” Journal of Cu-
taneous Pathology, Vol. 35, No. 3, 2008, pp. 311-314.
doi:10.1111/j.1600-0560.2007.00806.x
[6] M. Deguchi, H. Ohtani, E. Sato, Y. Naito, H. Nagura, S.
Aiba and H. Tagami, “Proliferative Activity of CD8(+) T
Cells as an Important Clue to Analyze T Cell-Mediated
Inflammatory Dermatoses,” Archives Dermatology Re-
search, Vol. 293, No. 9, 2001, pp. 442-447.
doi:10.1007/s004030100255
[7] M. M. Khambaty, “Dermatology of the Patient with
HIV,” Emergency Medicine Clinics of North America,
Vol. 28, No. 2, 2010, pp. 355-368.
doi:10.1016/j.emc.2010.01.001
[8] P. K. Ramdial, “Dermatopathological Challenges in the
Human Immunodeficiency Virus and Acquired Immuno-
deficiency Syndrome Era,” Histopathology, Vol. 56, No.
1, 2010, pp. 39-56.
doi:10.1111/j.1365-2559.2009.03456.x
[9] G. E. Rodwell and T. G. Berger, “Pruritus and Cutaneous
Inflammatory Conditions in HIV Disease,” Clinics in
Dermatology, Vol. 18, No. 4, 2000, pp. 479-484.
doi:10.1016/S0738-081X(99)00143-1
[10] D. Rigopoulos, V. Paparizos and A. Katsambas, “Cuta-
neous Markers of HIV Infection,” Clinics in Dermatology,
Vol. 22, No. 6, 2004, pp. 487-498.
doi:10.1016/j.clindermatol.2004.07.007
[11] J. Luther and M. J. Glesby, “Dermatologic Adverse Ef-
fects of Antiretroviral Therapy,” American Journal of
Clinical Dermatology, Vol. 8, No. 6, 2007, pp. 221-233.
doi:10.2165/00128071-200708040-00004
[12] S. Mori and P. Levin, “A Brief Review of Potential
Mechanisms of Immune Reconstitution Inflammatory
Syndrome in HIV Following Antiretroviral Therapy,” In-
ternational Journal of STD & AIDS, Vol. 20, No. 7, 2009,
pp. 447-452. doi:10.1258/ijsa.2009.008521
[13] S. A. Shelburne, F. Visnegarwala, J. Darcourt, E. A.
Graviss, T. P. Giordano, A. C. White Jr. and R. J. Hamill,
“Incidence and Risk Factors for Immune Reconstitution
inflammatory Syndrome during Highly Active Antiretro-
viral Therapy,” AIDS, Vol. 19, No. 4, 2005, pp. 399-406.
doi:10.1097/01.aids.0000161769.06158.8a