J. J. H. Elósegui et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 197-201
200
this moment and sometimes other pharmacologic agents
can be employeed to assist uterine relaxation for achiev-
ing correction (tocolytic agents like terbutaline, magne-
sium sulphate and glyceryl trinitrate). If correction is not
obtained with tocolytic agents, general anaesthesia with
halothane may be induced to provide uterine relaxation.
This approach may be specially useful when the woman
is haemodynamically unstable, because halothane anae-
sthesia has fewer potential adverse effects on haemody-
namics [17,20]. About this concern, it is interesting to
note here that epidural analgesia does not help in uterine
reposition, as it does not affect uterine tone [21]. When
uterus is replaced, further agents are recommended to
achieve a powerful-enough uterine contraction able to
prevent uterine reinversion and decrease blood loss. If
these methods fail, surgical intervention might be nece-
ssary.
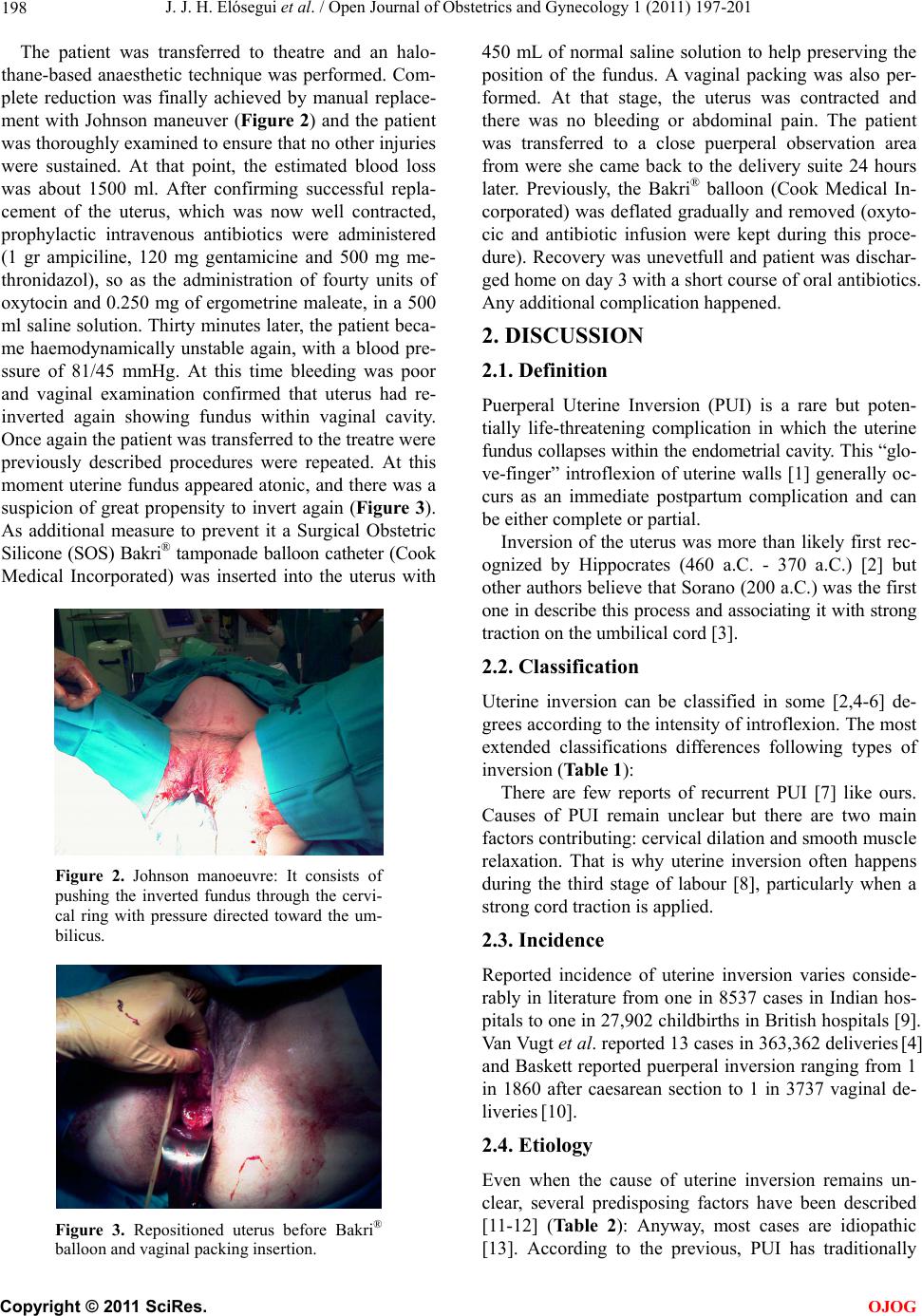
In our case, manual correction of uterine inversion was
made through the vagina by the Johnson maneuver, that
consists on pushing the inverted fundus through the cer-
vical ring with energic pressure directed toward the um-
bilicus [21,22]. It is generally suggested that removal of
the placenta before correction will result in increased
blood loss, so it is not recommended removing it, until
uterus has been replaced. Rates of immediate reduction
vary from 22% to 43% [17].
Apart from Johnson manoeuvre, some authors have
reported the use of hydrostatic pressure [23] caused by
warm water infused into the vagina to reduce uterine in-
version reduction.
When all attempts at manual reduction of the inver-
sion are unsuccessful, surgical correctionis often neces-
sary. The three most common procedures are the Hun-
tington, Haultain and Spinelli ones, but the first one is
considered the elegible. It consists on a laparotomy to
traction round ligaments and uterus to restore normal a-
natomy. Occasionally, as a life-saving measure, emer-
gency peripartum or obstetric hysterectomy is needed to
achieve control of haemorrhage [24].
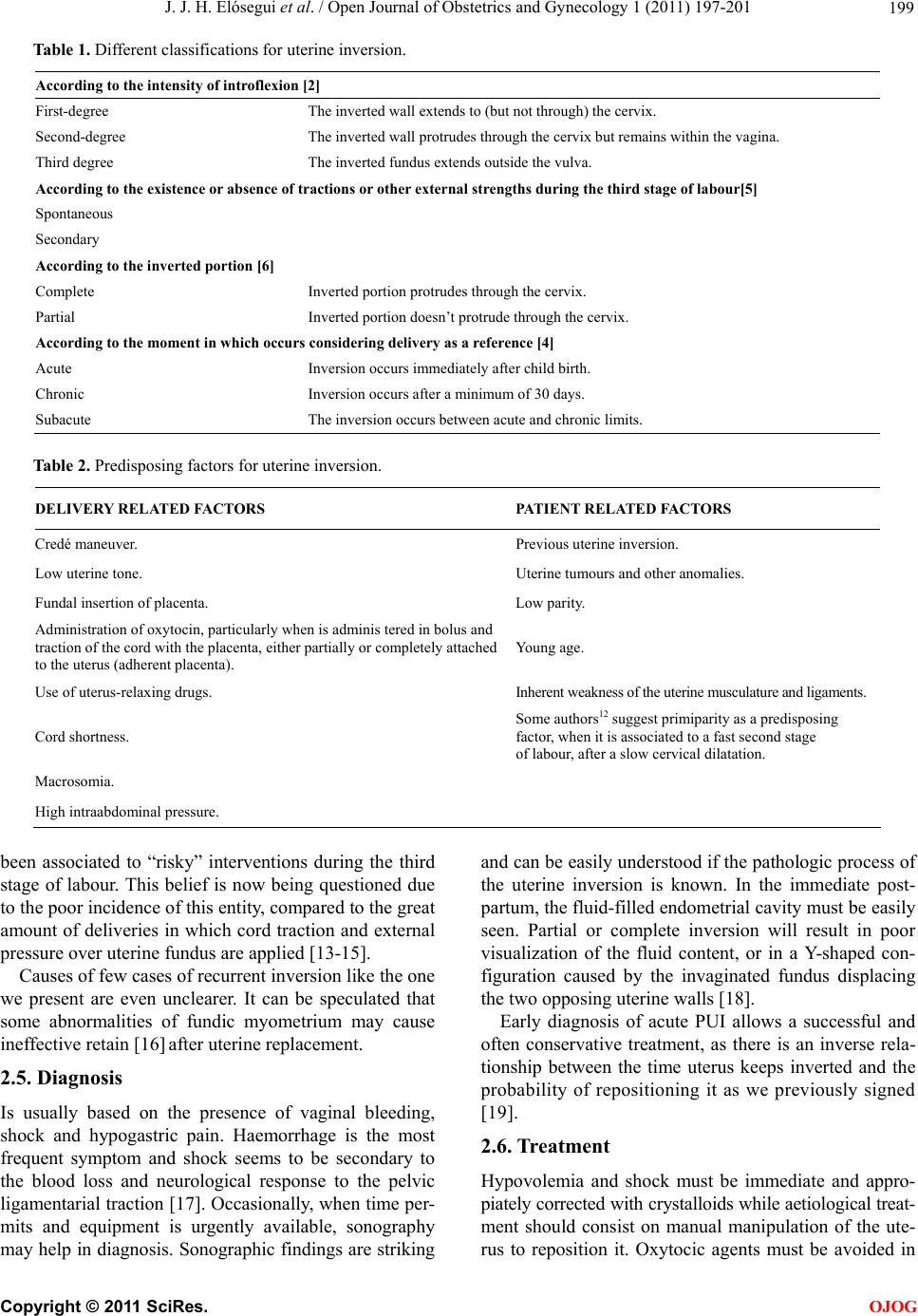
In our case surgical procedure was not necessary and
patient’s reproductive potential was kept, even being a re-
current case of uterine inversion. This conservative ma-
nagement of recurrent uterine inversion was based in
uterus reposition and insertion of a SOS Bakri® balloon
(Cook Medical Incorporated), which conformed to the
contours of the uterine cavity to prevent re-inversion of
the uterus.
The Bakri® tamponade balloon is 58 cm long silicone-
made inflatable balloon with a double lumen shaft, that
is easily removed transvaginally after deflation. Balloon
maximum capacity is 800 mL. and never should be in-
flated with less than 250 mL. However, the recommen-
ded use is up to 500 mL. The tip of the shaft has two
holes for drainage, so ongoing haemorrhage can be de-
tected after application of the balloon [25].
This case describes the exceptional and novedous use
of the SOS Bak ri® balloon (Cook Medical Incorporated)
in the management of recurrent puerperal uterine inver-
sion. To our knowledg e it is on e of the first reports in th e
world of this procedure, perhaps the second one after So-
leymani’s et al description [16] and the first one in a
third degree recurrent puerperal uterine inversion.
3. CONCLUSIONS
Insertion of intrauterine balloon tamponade may be an
effective measure to treat uterine inversion and prevent
its recurrence.
REFERENCES
[1] Morini, A., Angelini, R. and Giardini, G. (1994) Acute
puerperal uterine inversion: A report of 3 cases and an
analysis of 358 cases in the literature. Minerva Gine-
cologica, 46, 115-127.
[2] Siva, A., Zarina, M. and Mukudan, K. (2006) Puerperal
uterine inversion: A report of four cases. Journal of Ob-
stetrics and Gynaecology Research, 32, 341-345.
doi:10.1111/j.1447-0756.2006.00407.x
[3] Das, P. (1940) Inversion of the uterus. British Journal of
Obstetrics and Gynaecology, 47, 525-548.
doi:10.1111/j.1471-0528.1940.tb08843.x
[4] Van Vugt, P.J., Baudoin, P., Blom, V.M. and Van Deursen,
C.T. (1981) Inversio uteri puerperalis. Acta Obstetricia et
Gynecologica Scandinavica, 60, 353-362.
doi:10.3109/00016348109154123
[5] Milenkovic, M. and Khan, J. (2005) Inversion of the
uterus: A serious complication at childbirth. Acta Ob-
stetricia et Gynecologica Scandinavica, 84, 95-106.
doi:10.1111/j.0001-6349.2005.0254b.x
[6] Simó, M., Peñalva, G. and Domingo, X. (1992) Inversión
uterina obstétrica: Caso clínico y revisión del tema. Acta
Ginecológica, 49, 141-143.
[7] O’Connor, C.M. (1977) Recurrent postpartum uterine in-
version. British Journal of Obstetrics Gynaecology, 84,
789-790. doi:10.1111/j.1471-0528.1977.tb12494.x
[8] Bell, J.E. Jr., Wilson, G.F. and Wilson, L.A. (1953)
Puerperal inversion of the uterus. American Journal of
Obstettics Gynecology, 66, 767-780.
[9] Mehra, U. and Ostapowicz, F. (1976) Acute puerperal
inversion of the uterus in a primipara. Obstetrics and
Gynecology, 47, 30-32.
[10] Baskett, T.F. (2002) Acute uterine inversion. Review of
40 cases. Journal of Obstetrics and Gynaecology Canada,
24, 953-956.
[11] Vavilis, D., Tsolakidis, D., Goutzioulis, A.D. and Bontis,
J.N. (2008) Complete uterine inversion during caesarean.
Cases Journal, 1, 127. doi:10.1186/1757-1626-1-127
[12] Hostetler, D.R. and Bosworth, M.F. (2000) Uterine In-
version. A life-theatening Obstetric emergency. Journal
of the American Board of Family Practice, 3, 120-123.
[13] Parikshit, D.T. and Niranjan, M.M. (2004) Pregnancy
outcome after operative correction of puerperal uterine
inversion. Archives of Gynecology and Obstetrics, 69,
C
opyright © 2011 SciRes. OJOG