M. S. GOND ET AL.
342
defect and was contained behind the ascending colon
creating a retroperitoneal bulge. The caecum and as-
cending colon were mobilised after incising the perito-
neal fold along the ascend ing colon. The herniated small
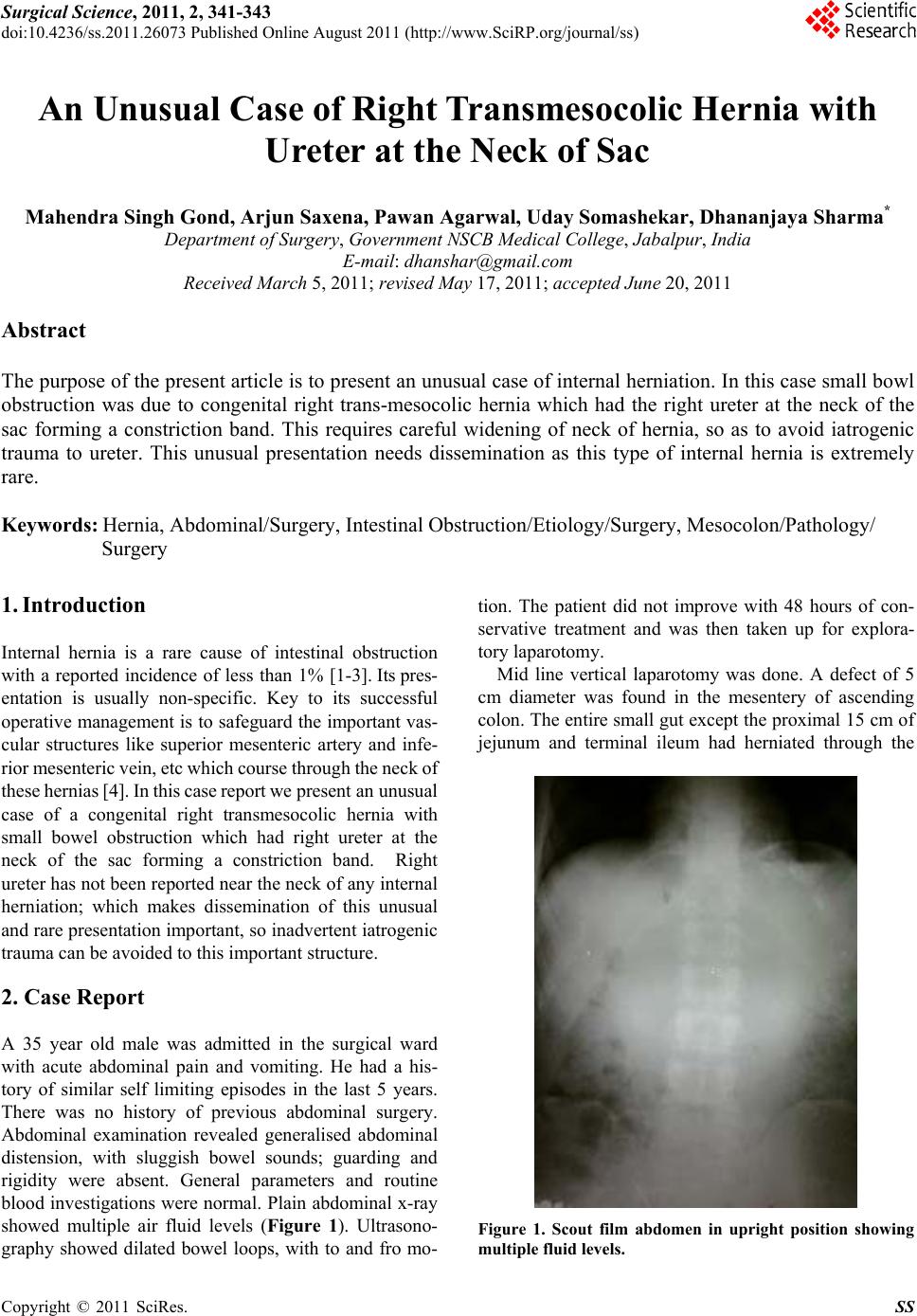
bowel was viable but congested. A tubular structure was
found in the neck of hernia sac, which on closer inspec-
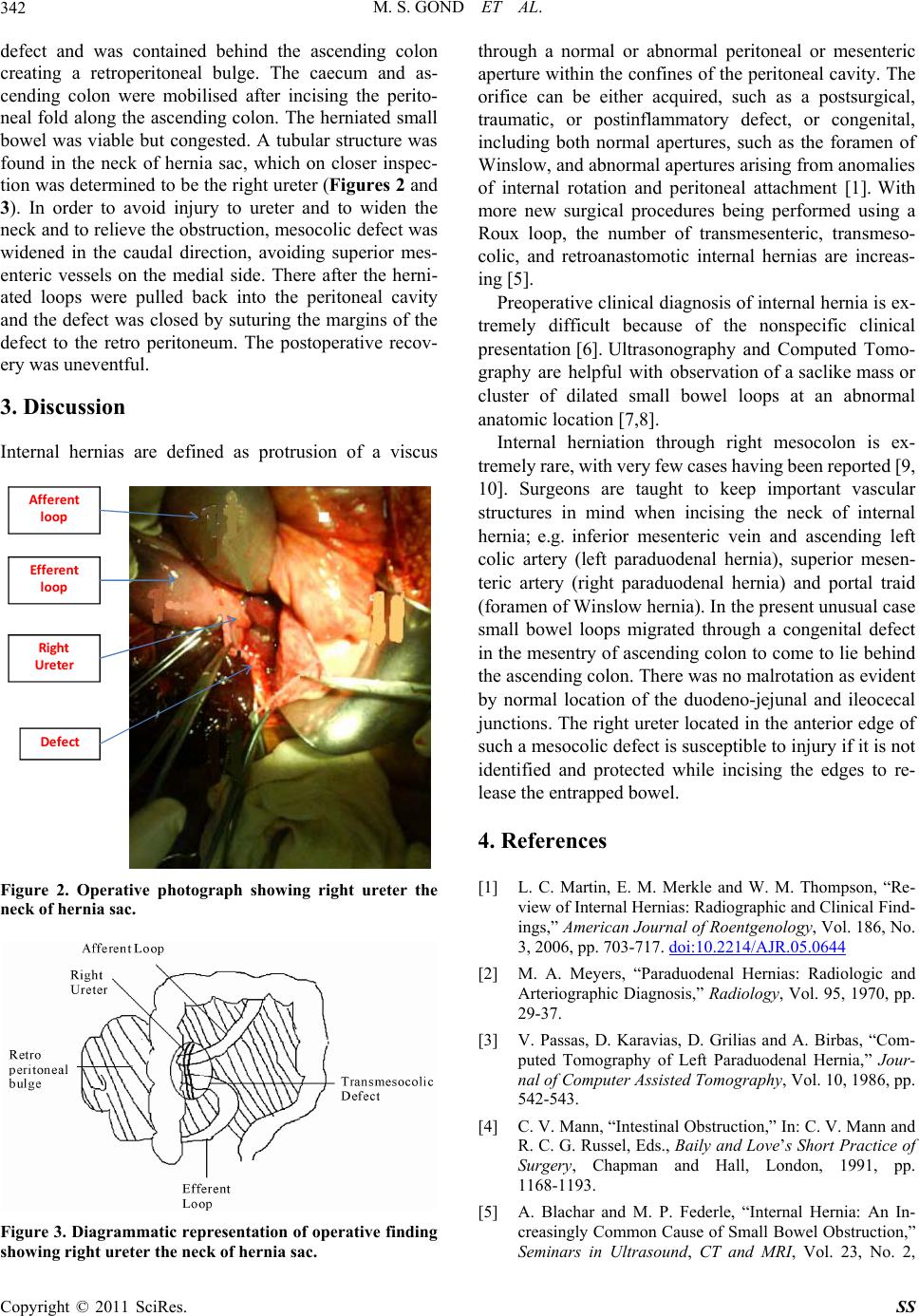
tion was determined to be the right ureter (Figures 2 and
3). In order to avoid injury to ureter and to widen the
neck and to relieve the obstruction, mesocolic defect was
widened in the caudal direction, avoiding superior mes-
enteric vessels on the medial side. There after the herni-
ated loops were pulled back into the peritoneal cavity
and the defect was closed by suturing the margins of the
defect to the retro peritoneum. The postoperative recov-
ery was uneventful.
3. Discussion
Internal hernias are defined as protrusion of a viscus
Afferent
loop
Efferent
loop
Ri g h t
Ureter
De fe c t
Figure 2. Operative photograph showing right ureter the
neck of hernia sac.
Figure 3. Diagrammatic representation of operative finding
showing right ureter the neck of hernia sac.
through a normal or abnormal peritoneal or mesenteric
aperture within the confines of the peritoneal cavity. The
orifice can be either acquired, such as a postsurgical,
traumatic, or postinflammatory defect, or congenital,
including both normal apertures, such as the foramen of
Winslow, and abnormal apertures arising from anomalies
of internal rotation and peritoneal attachment [1]. With
more new surgical procedures being performed using a
Roux loop, the number of transmesenteric, transmeso-
colic, and retroanastomotic internal hernias are increas-
ing [5].
Preoperative clinical diagnosis of internal hernia is ex-
tremely difficult because of the nonspecific clinical
presentation [6]. Ultrasonography and Computed Tomo-
graphy are helpful with observation of a saclike mass or
cluster of dilated small bowel loops at an abnormal
anatomic location [7,8].
Internal herniation through right mesocolon is ex-
tremely rare, with very few ca ses having been rep orted [9,
10]. Surgeons are taught to keep important vascular
structures in mind when incising the neck of internal
hernia; e.g. inferior mesenteric vein and ascending left
colic artery (left paraduodenal hernia), superior mesen-
teric artery (right paraduodenal hernia) and portal traid
(foramen of Winslow hernia). In the present unusual case
small bowel loops migrated through a congenital defect
in the mesentry of ascending co lon to come to lie behind
the ascending colon. There was no malrotation as evident
by normal location of the duodeno-jejunal and ileocecal
junctions. The right ureter located in the anterior edge of
such a mesocolic defect is susceptible to injury if it is not
identified and protected while incising the edges to re-
lease the entrapped bowel.
4. References
[1] L. C. Martin, E. M. Merkle and W. M. Thompson, “Re-
view of Internal Hernias: Radiographic and Clinical Find-
ings,” American Journal of Roentgenology, Vol. 186, No.
3, 2006, pp. 703-717. doi:10.2214/AJR.05.0644
[2] M. A. Meyers, “Paraduodenal Hernias: Radiologic and
Arteriographic Diagnosis,” Radiology, Vol. 95, 1970, pp.
29-37.
[3] V. Passas, D. Karavias, D. Grilias and A. Birbas, “Com-
puted Tomography of Left Paraduodenal Hernia,” Jour-
nal of Computer Assisted Tomography, Vol. 10, 1986, pp.
542-543.
[4] C. V. Mann, “Intestinal Obstruction,” In: C. V. Mann and
R. C. G. Russel, Eds., Baily and Love’s Short Practice of
Surgery, Chapman and Hall, London, 1991, pp.
1168-1193.
[5] A. Blachar and M. P. Federle, “Internal Hernia: An In-
creasingly Common Cause of Small Bowel Obstruction,”
Seminars in Ultrasound, CT and MRI, Vol. 23, No. 2,
Copyright © 2011 SciRes. SS