Comparitive Study between Proximal Femoral Nailing and Dynamic Hip Screw in Intertrochanteric Fracture of Femur 295
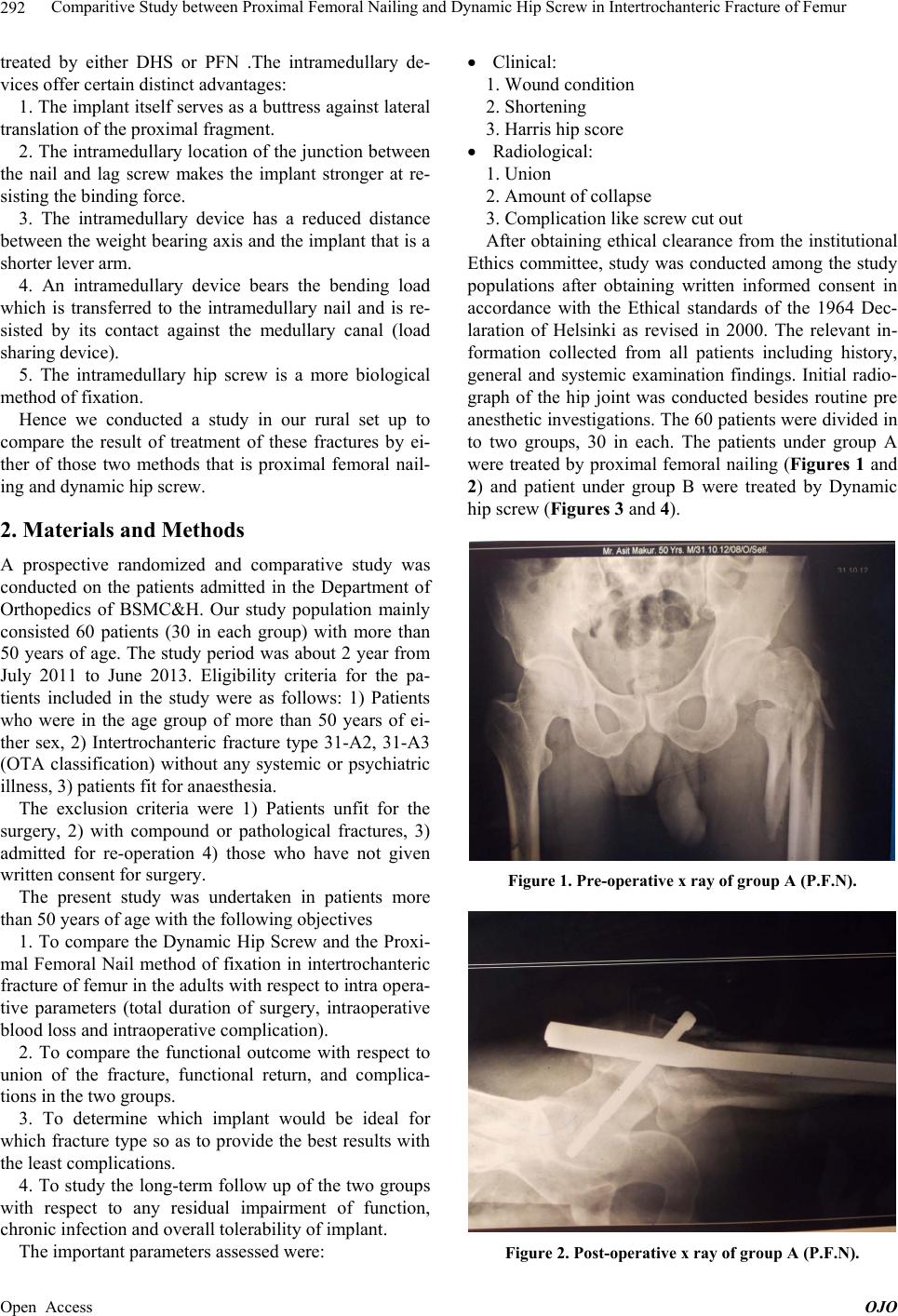
Table 3. Intraoperative complication of PFN.
Complications No of Patient Percentage
Failure to achieve closed
reduction 0 0
Fracture of lateral cortex 0 0
Failure to put derotation screw 3 10%
Fracture displacement by nai l
insertion 1 3.33%
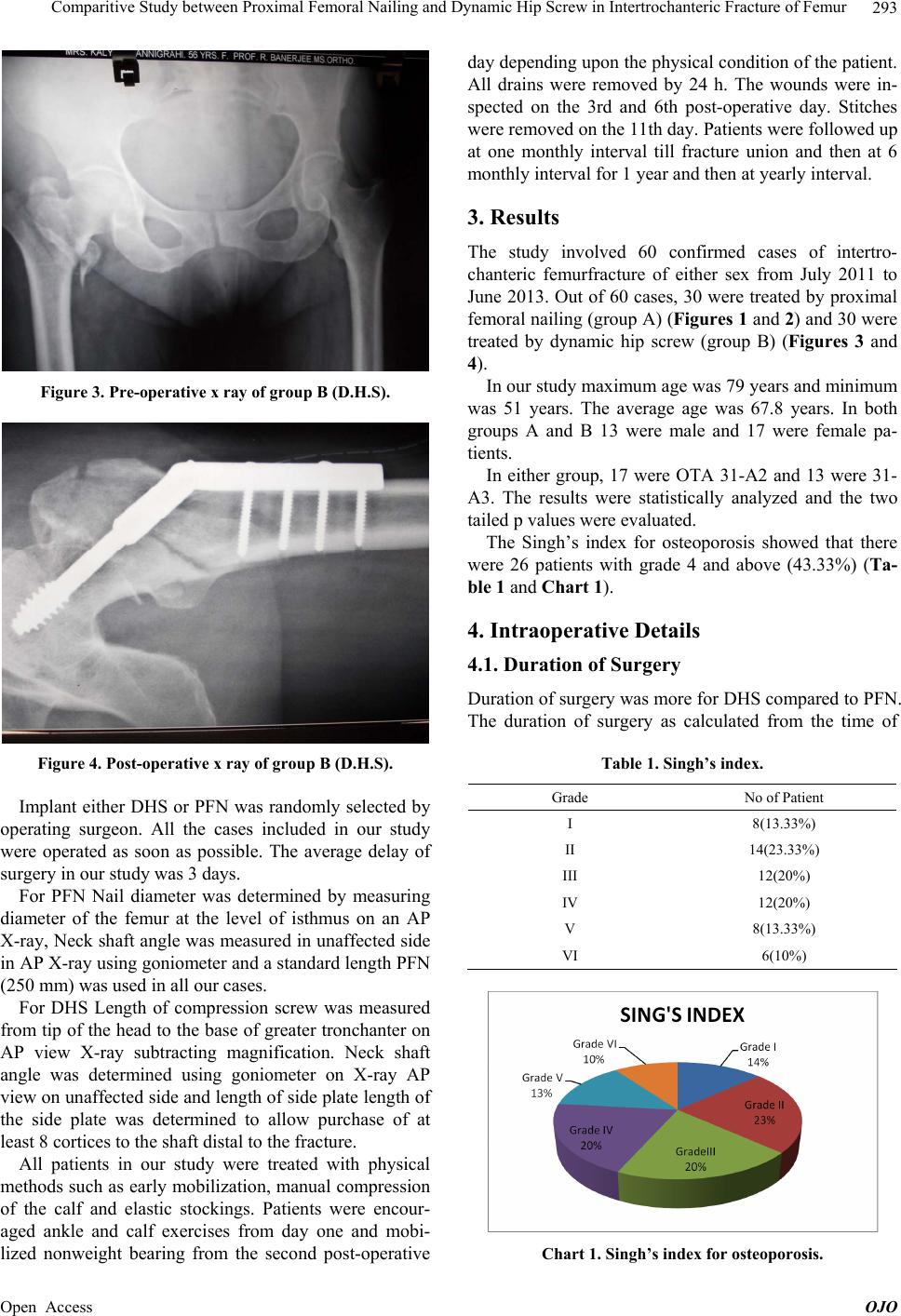
Table 4. Intraoperative complications DHS.
Intraoperative
complication No of patient Percentage
Improper ins ertion of
compression screw 2 6.66%
varus angulation 2 6.66%
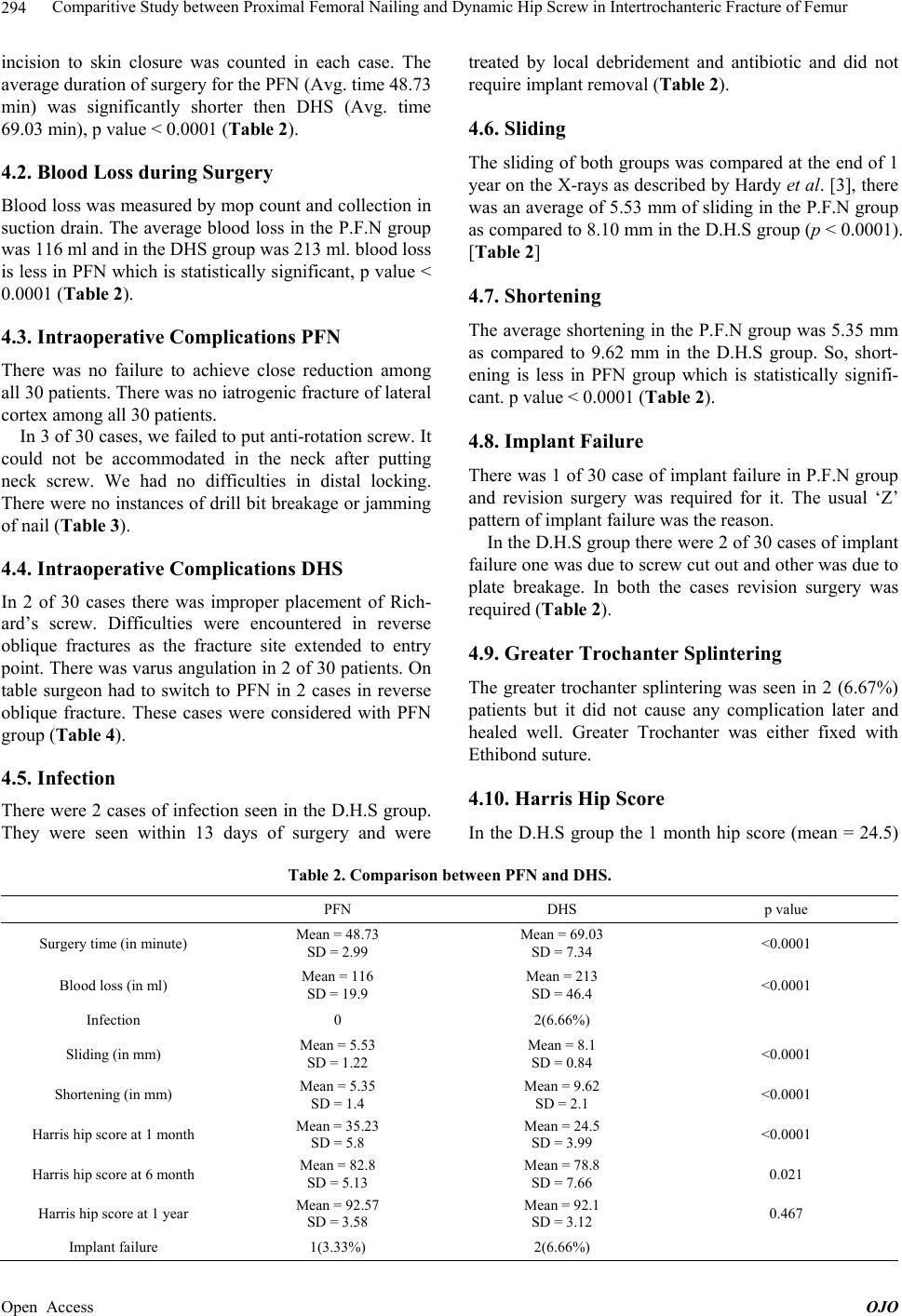
was less than that of the P.F.N group (mean = 35.23), p <
0.0001, in 6 month hip score in DHS (mean = 78.8) was
also less than that of PFN (mean = 82.8) , p value = 0.021.
However this difference disappeared with the two group
after 1 year follow up being same (D.H.S-92.1 and
P.F.N-92.57). p value = 0.467 (Table 2 and Chart 2).
5. Discussion
The development of the dynamic hip screw in the 1960’s
saw a revolution in the management of unstable fractures.
The device allowed compression of the fracture site
without complications of screw cut-out and implant
breakage associated with a nail plate. However, the ex-
tensive surgical dissection, blood loss and surgical time
required for this procedure often made it a contraindica-
tion in the elderly with co-morbidities. The implant also
failed to give good results in extremely unstable and the
reverse obli que fracture.
In the early 90s intramedullary devices were developed
for fixation of Intertrochanteric fractures. These devices
0
10
20
30
40
50
60
70
80
90
100
at 1 monthat 6 monthat 1 year
P.F.N.
D.H.S.
Chart 2. Harris hip score.
had numerous biomechanical and biological advantages
over the conventional dynamic hip screw [4-6]. Long
term studies, however, revealed that the use of these de-
vices was associated with higher intra operative and late
complication often requiring revision surgery. This has
led to modifications in the device and technique of the
intramedullary devices.
In our study we found:
Less operative time in PFN group
Less operative b l o od loss in PFN gro up
Early return to daily activities.
Less complication in PFN group like less infection,
less sliding, less limb length discrepancy compared to
DHS group.
The plate and screw device will weaken the bone me-
chanically. The common causes of fixation failure are
instability of the fractures, osteoporosis, and the lack of
anatomical reduction, failure of fixation device and in-
correct placement of the screw.
We found the proximal femoral nail to be more useful
in unstable and reverse oblique patterns.
Hence PFN is much superior to DHS in management
of fracture intertrochanteric femur.
REFERENCES
[1] D. Carter and W. Hayes, “The Compressive Behavior of
Bone as a Two-Phase Porous Structure,” The Journal of
Bone & Joint Surgery, Vol. 59A, No. 7, 1977, pp. 954-
962.
[2] B. Gullberg, O. Johnell and J. A. Kanis, “World Wide
Projection for Hip Fracture,” Osteoporosis International,
Vol. 7, No. 5, 1997, pp. 407-413.
http://dx.doi.org/10.1007/PL00004148
[3] L. J. Melton, A. E. Kearns, E. J. Atkinson, et al., “Secular
Trends in Hip Fracture Incidence and Recurrence,” Os-
teoporosis International, Vol. 20, No. 5, 2009, pp. 687-
694. http://dx.doi.org/10.1007/s00198-008-0742-8
[4] D. Hardy, P. Descamps, P. Krallis, et al., “Use of an In-
tramedullary Hip Screw Compared with a Compression
Hip Screw with a Plate for Intertrochanteric Femoral
Fractures. A Prospective Randomized Study of One Hun-
dred Patients,” The Journal of Bone & Joint Surgery, Vol.
80, 1998, pp. 618-630.
[5] J. M. Spivak, J. D. Zuckerma n and F. J. Kumme, “Fa tigue
Failure of Sliding Hip Screw in Hip Fractures. A Report
of Three Cases,” Journal of Orthopaedic Trauma, 1991,
Vol. 3, pp. 325-331.
http://dx.doi.org/10.1097/00005131-199109000-00012
[6] K. S. Leung, W. S. So, W. Y. Shen and P. W. Hui, “Gam-
ma Nails and Dynamic Hip Screws for Pertrochanteric
Fractures. A Randomized Prospective Study in Elderly
Patients,” The Bone & Joint Journal, Vol. 74, 1992, pp.
345-351.
Open Access OJO