Extracellular Fluid Accumulation Predicts Fluid Responsiveness after Hydroxyethyl Starch 70/0.5
Bolus Infusion during Major Abdominal Surgery
419
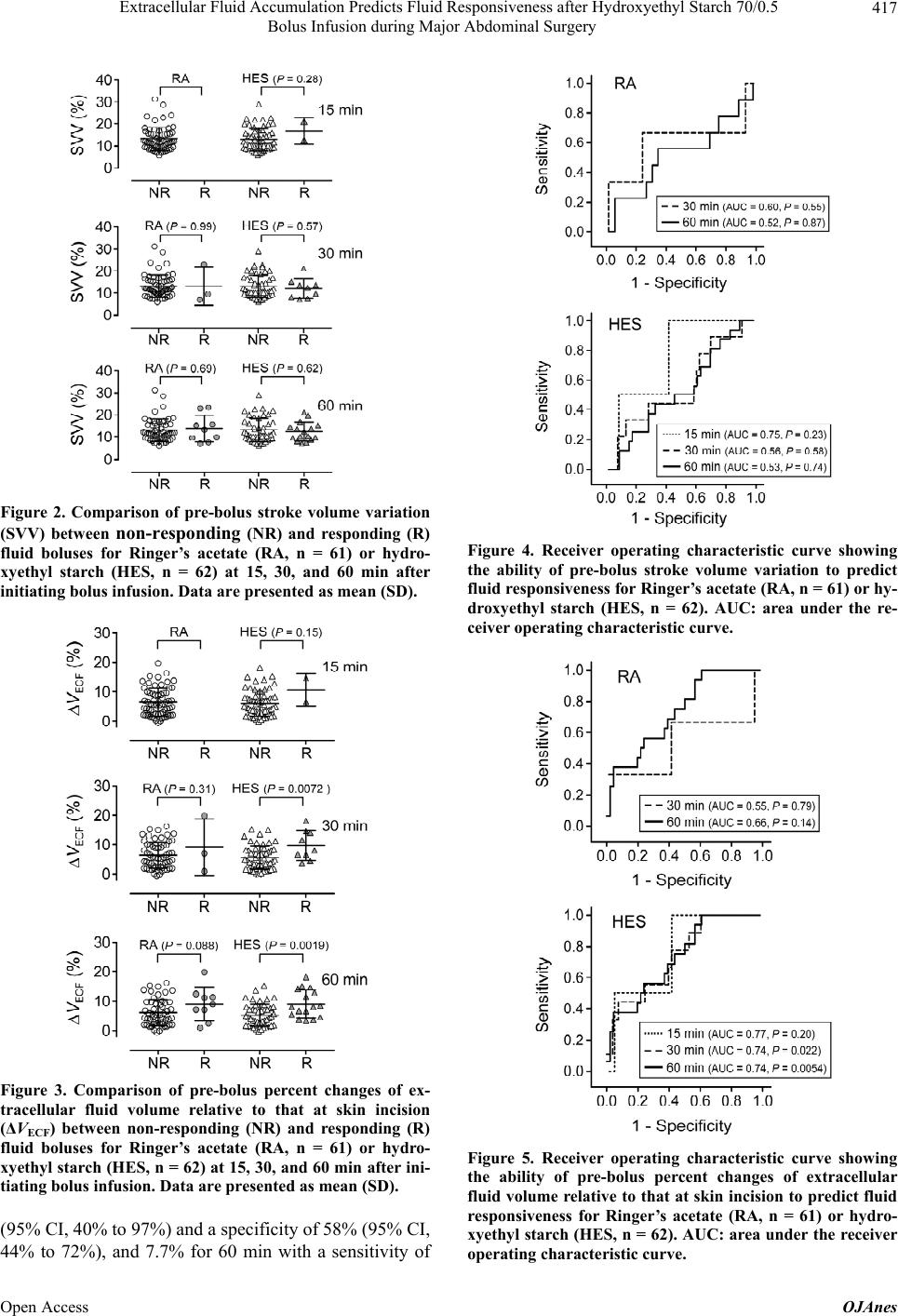
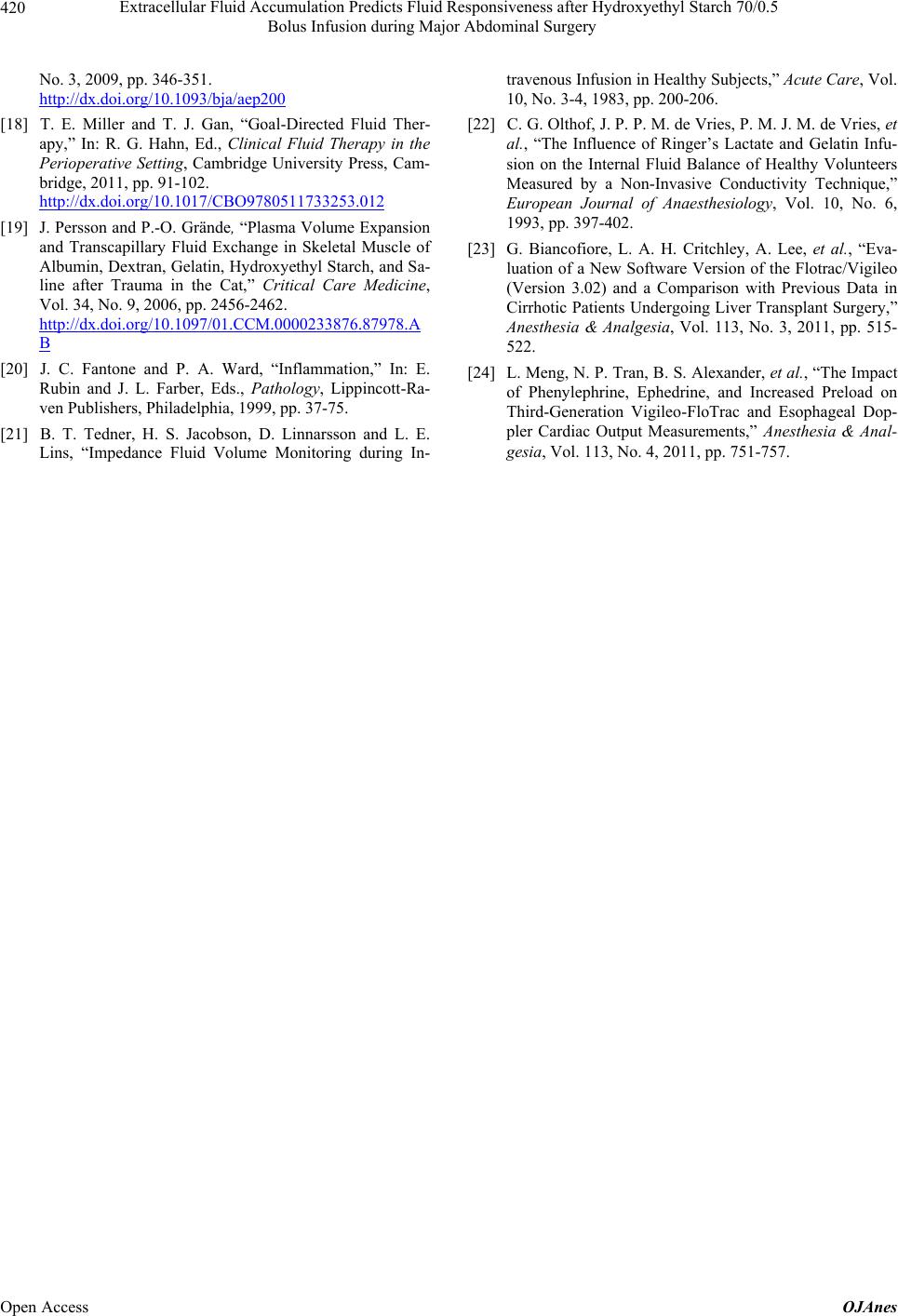
be reduced due to capillary leakage arising from surgical
injury. Yet, upon enhanced accumulation of extracellular
fluid, HES bolus infusion can recover cardiac preload
and fluid responsiveness 30 - 60 min after bolus infusion
by extracting more fluid from the interstitial space. The
threshold of pre-bolus ΔVECF for exerting this effect was
6% - 8%, corresponding to 12 - 16 mL/kg of extracellular
fluid accumulation in the entire body. The dependence of
fluid responsiveness after HES bolus infusion on ex-
tracellular fluid volume should be taken into account
when determining the optimal timing and right volume of
HES infusion for intra- and postoperative use in patients
undergoing major abdominal surgery. Our findings sug-
gest that HES use is preferable during the later stages of
surgery when interstitial fluid accumulates, thereby pre-
venting HES overdose.
In conclusion, our finding suggests that extracellular
fluid volume can predict fluid responsiveness after HES
bolus infusion during major abdominal surgery, which
becomes larger with interstitial fluid accumulation.
5. Acknowledgements
We thank Dr. Maxime Cannesson for critical comments
and valuable suggestions. This work was supported by
Grants-in-Aid for Scientific Research (C) [No. 20591846]
and [No. 24592365] from the Ministry of Education,
Science and Culture of Japan. Tsuneo Tatara received
speaking fees from Edwards Lifesciences and Fresenius
Kabi Japan.
REFERENCES
[1] T. J. Gan, A. Soppitt, M. Maroof, et al., “Goal-Directed
Intraoperative Fluid Administration Reduces Length of
Hospital Stay after Major Surgery,” Anesthesiology, Vol.
97, No. 4, 2002, pp. 820-826.
http://dx.doi.org/10.1097/00000542-200210000-00012
[2] A. Donati, S. Loggi, J.-C. Preiser, et al., “Goal-Directed
Intraoperative Therapy Reduces Morbidity and Length of
Hospital Stay in High-Risk Surgical Patients,” Chest, Vol.
132, No. 6, 2007, pp. 1817-1824.
http://dx.doi.org/10.1378/chest.07-0621
[3] M. Bundgaard-Nielsen, K. Holte, N. H. Secher and H.
Kehlet, “Monitoring of Peri-Operative Fluid Administra-
tion by Individualized Goal-Directed Therapy,” Acta An-
aesthesiologica Scandinavica, Vol. 51, No. 3, 2007, pp.
331-340.
http://dx.doi.org/10.1111/j.1399-6576.2006.01221.x
[4] C. S. Hartog, M. Bauer and K. Reinhart, “The Efficacy
and Safety of Colloid Resuscitation in the Critically Ill,”
Anesthesia & Analgesia, Vol. 112, No. 1, 2011, pp. 156-
164. http://dx.doi.org/10.1213/ANE.0b013e3181eaff91
[5] C. S. Hartog, M. Kohl and K. Reinhart, “A Systematic
Review of Third-Generation Hydroxyethyl Starch (HES130/
0.4) in Resuscitation: Safety Not Adequately Addressed,”
Anesthesia & Analgesia, Vol. 112, No. 3, 2011, pp. 635-
645. http://dx.doi.org/10.1213/ANE.0b013e31820ad607
[6] D. Chappell, M. Jacob, K. Hofmann-Kiefer, et al., “A
Rational Approach to Perioperative Fluid Management,”
Anesthesiology, Vol. 109, No. 4, 2008, pp. 723-740.
http://dx.doi.org/10.1097/ALN.0b013e3181863117
[7] J.-L. Vincent, “Let’s Give Some Fluid and See What
Happens” versus the “Mini-Fluid Challenge,” Anesthesi-
ology, Vol. 115, No. 3, 2011, pp. 455-456.
http://dx.doi.org/10.1097/ALN.0b013e318229a521
[8] M. Cannesson, “Non-Invasive Guidance of Fluid Ther-
apy,” In: R. G. Hahn, Ed., Clinical Fluid Therapy in the
Perioperative Setting, Cambridge University Press, Cam-
bridge, 2011, pp. 103-111.
http://dx.doi.org/10.1017/CBO9780511733253
[9] T. Tatara, Y. Nagao and C. Tashiro, “Effect of Duration
of Surgery on Fluid Balance during Abdominal Surgery:
A Mathematical Model,” Anesthesia & Analgesia, Vol.
109, No. 1, 2009, pp. 211-216.
http://dx.doi.org/10.1213/ane.0b013e3181a3d3dc
[10] K. Aukland and R. K. Reed, “Interstitial-Lymphatic Me-
chanisms in the Control of Extracellular Fluid Volume,”
Physiological Reviews, Vol. 73, No. 1, 1993, pp. 1-78.
[11] T. Tatara and K. Tsuzaki, “Segmental Bioelectrical Im-
pedance Analysis Improves the Prediction for Extracellu-
lar Water Volume Changes during Abdominal Surgery,”
Critical Care Medicine, Vol. 26, No. 3, 1998, pp. 470-
476.
http://dx.doi.org/10.1097/00003246-199803000-00017
[12] D. Bracco, J.-P. Revelly, M. M. Berger and R. Chioléro,
“Bedside Determination of Fluid Accumulation after Car-
diac Surgery Using Segmental Bioelectrical Impedance,”
Critical Care Medicine, Vol. 26, No. 6, 1998, pp. 1065-
1070.
http://dx.doi.org/10.1097/00003246-199806000-00029
[13] D. Bracco, M. M. Berger, J.-P. Revelly, et al., “Segmen-
tal Bioelectrical Impedance Analysis to Assess Periopera-
tive Fluid Changes,” Critical Care Medicine, Vol. 28, No.
7, 2000, pp. 2390-2396.
http://dx.doi.org/10.1097/00003246-200007000-00034
[14] A. De Lorenzo, A. Andreoli, J. Matthie and P. Withers,
“Predicting Body Cell Mass with Bioimpedance by Using
Theoretical Methods: A Technological Review,” Journal
of Applied Physiology, Vol. 82, No. 5, 1997, pp. 1542-
1558.
[15] V. Nisanevich, I. Felsenstein, G. Almogy, et al., “Effect
of Intraoperative Fluid Management on Outcome after In-
traabdominal Surgery,” Anesthesiology, Vol. 103, No. 1,
2005, pp. 25-32.
http://dx.doi.org/10.1097/00000542-200507000-00008
[16] J. Renner, J. Scholz and B. Bein, “Monitoring Fluid Ther-
apy,” Best Practice & Research Clinical Anaesthesiology,
Vol. 23, No. 2, 2009, pp. 159-171.
http://dx.doi.org/10.1016/j.bpa.2008.12.001
[17] D. Lahner, B. Kabon, C. Marschalek, et al., “Evaluation
of Stroke Volume Variation Obtained by Arterial Pulse
Contour Analysis to Predict Fluid Responsiveness Intra-
operatively,” British Journal of Anaesthesia, Vol. 103,
Open Access OJAnes