 Open Journal of Stomatology, 2013, 3, 411-418 OJST http://dx.doi.org/10.4236/ojst.2013.38069 Published Online November 2013 (http://www.scirp.org/journal/ojst/) Porcelain fracture of metal-ceramic tooth-supported and implant-supported restorations: A review Rola M. Shadid1, Nasrin R. Sadaqah1, Layla Abu-Naba’a2, Wael M. Al-Omari3 1Department of Prosthodontics, Faculty of Dentistry, Arab American University, Jenin, Palestine 2Department of Substitutive Dental Sciences, Faculty of Dentistry, Taibah University, KSA-Formerly Jordan University of Science and Technology, Irbid, Jordan 3Department of Prosthodontics, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan Email: rola_shadeed@yahoo.com Received 31 May 2013; revised 2 July 2013; accepted 21 October 2013 Copyright © 2013 Rola M. Shadid et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Metal-ceramic restorations are widely used in den- tistry with a high degree of general success. However, fracture of these restorations does occur and usually frustrates both the dentist and the patient. Objective: This literature review discusses the factors that may lead to the fracture of these restorations whether they are tooth-supported or implant-supported with the aim of making dentists and technicians aware of these factors to avoid them. Factors reviewed include: tech- nical factors, dentist-related factors, inherent mate- rial properties, direction, magnitude and frequency of applied loads, environmental factors, screw-retained implant-supported restorations, and posterior canti- levered prostheses. Material and Methods: A net- based search in “Pubmed” was performed and com- bined with a manual search. The search was limited to articles written in English. Conclusions: the pub- lished literature revealed that the factors predispos- ing to fracture of metal-ceramic restorations may be related to the technician, dentist, patient, environ- ment, design of the restoration, or to inherent struc- ture of ceramics and others. However, if the dentist and technician understand these factors and respect the physical characteristics of the materials, most of those are avoidable. Keywords: Metal-Ceramic; Fracture; Implant-Supported Restoration; Screw-Retained 1. INTRODUCTION Although most of the concentration today is on all-ce- ramic restorations, metal-ceramic restorations, whether they are tooth-supported or implant-supported, are still considered as the gold standard because of their excellent biocompatibility, consistent esthetics, superior strength, and marginal adaptation. Also, metal-ceramic restora- tions are durable and long-lasting [1]; however, several investigators [2-5] demonstrated that the fracture of ce- ramic veneers is not an uncommon problem in clinical practice and may cause the premature failure of fixed partial dentures. Bragger et al. [6] found that there is an interrelation between porcelain fracture and the long- term survival of the fixed partial denture. The event of porcelain fracture increased the risk for the suprastruc- ture to become a failure at 10 years compared to a supra- structure with no porcelain fracture [6]. Numerous studies [4,5,7] have reported on the out- come of MC restorations supported by natural teeth abutments. In a survey of crown and fixed partial denture failures, Walton et al. [5] found that the incidence of porcelain fracture was the second most common cause of MC fixed partial denture replacement, accounting for 72 (16%) of 451 failed restorations. Also, they found that porcelain fracture was the most common cause of failure with sin- gle crown restorations. This is in agreement with another 7-year follow-up study from Strub et al. [4] who found that porcelain fracture was the most common cause of MC prosthesis failure. A systematic review [7] of 8 papers and 1,192 pros- theses supported by natural teeth abutments showed that veneer fracture was a common complication of metal- ceramic prostheses, with a mean incidence of up to 3% reported for single crowns and FPDs. Regarding implant-supported MC restorations, it has been shown that porcelain fracture is also a common complication in implant-supported restorations [8]. A follow-up study [3] of 92 cement-retained metal- ceramic implant-supported prostheses, including single- OPEN ACCESS 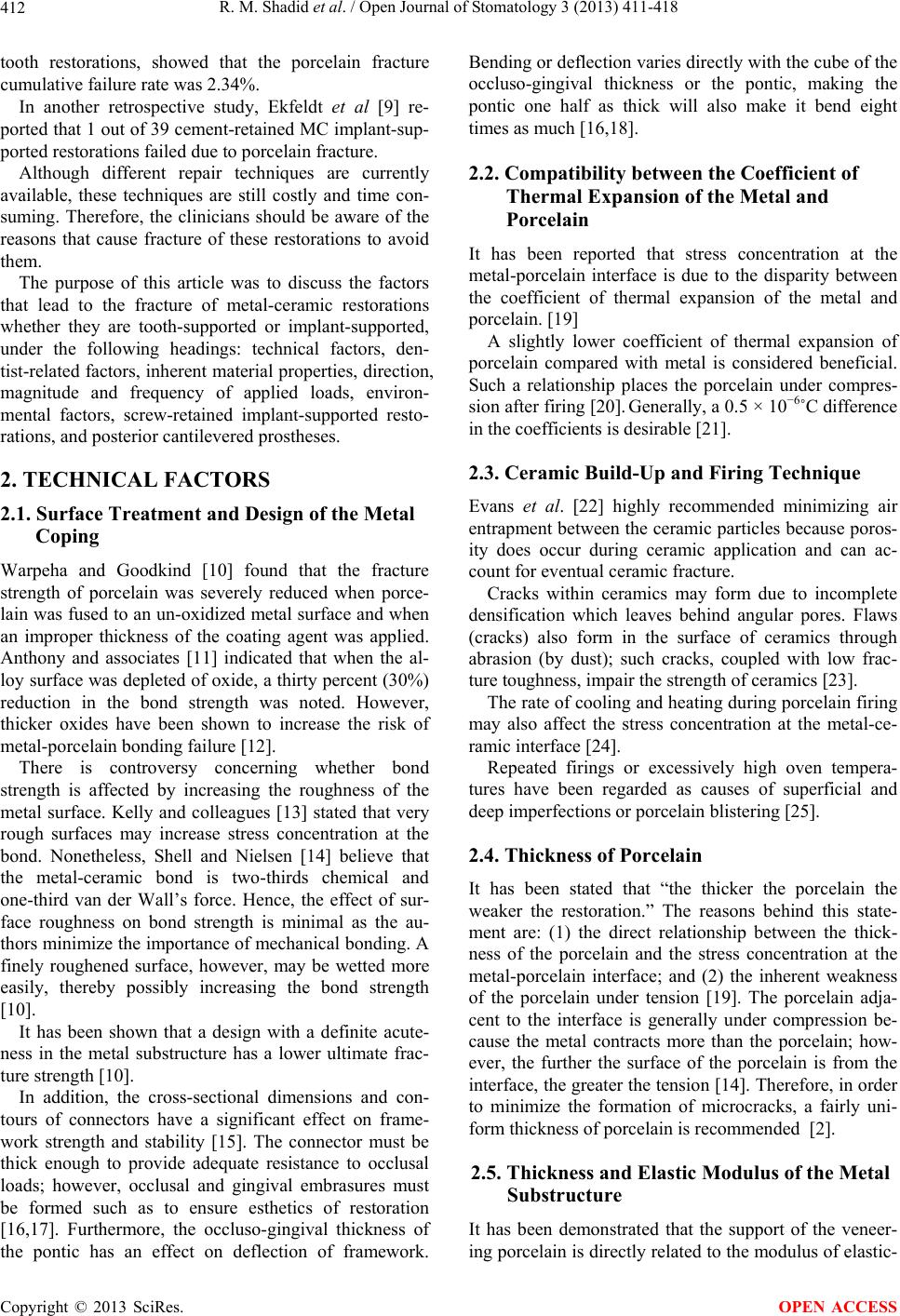 R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 412 tooth restorations, showed that the porcelain fracture cumulative failure rate was 2.34%. In another retrospective study, Ekfeldt et al [9] re- ported that 1 out of 39 cement-retained MC implant-sup- ported restorations failed due to porcelain fracture. Although different repair techniques are currently available, these techniques are still costly and time con- suming. Therefore, the clinicians should be aware of the reasons that cause fracture of these restorations to avoid them. The purpose of this article was to discuss the factors that lead to the fracture of metal-ceramic restorations whether they are tooth-supported or implant-supported, under the following headings: technical factors, den- tist-related factors, inherent material properties, direction, magnitude and frequency of applied loads, environ- mental factors, screw-retained implant-supported resto- rations, and posterior cantilevered prostheses. 2. TECHNICAL FACTORS 2.1. Surface Treatment and Design of the Metal Coping Warpeha and Goodkind [10] found that the fracture strength of porcelain was severely reduced when porce- lain was fused to an un-oxidized metal surface and when an improper thickness of the coating agent was applied. Anthony and associates [11] indicated that when the al- loy surface was depleted of oxide, a thirty percent (30%) reduction in the bond strength was noted. However, thicker oxides have been shown to increase the risk of metal-porcelain bonding failure [12]. There is controversy concerning whether bond strength is affected by increasing the roughness of the metal surface. Kelly and colleagues [13] stated that very rough surfaces may increase stress concentration at the bond. Nonetheless, Shell and Nielsen [14] believe that the metal-ceramic bond is two-thirds chemical and one-third van der Wall’s force. Hence, the effect of sur- face roughness on bond strength is minimal as the au- thors minimize the importance of mechanical bonding. A finely roughened surface, however, may be wetted more easily, thereby possibly increasing the bond strength [10]. It has been shown that a design with a definite acute- ness in the metal substructure has a lower ultimate frac- ture strength [10]. In addition, the cross-sectional dimensions and con- tours of connectors have a significant effect on frame- work strength and stability [15]. The connector must be thick enough to provide adequate resistance to occlusal loads; however, occlusal and gingival embrasures must be formed such as to ensure esthetics of restoration [16,17]. Furthermore, the occluso-gingival thickness of the pontic has an effect on deflection of framework. Bending or deflection varies directly with the cube of the occluso-gingival thickness or the pontic, making the pontic one half as thick will also make it bend eight times as much [16,18]. 2.2. Compatibility between the Coefficient of Thermal Expansion of the Metal and Porcelain It has been reported that stress concentration at the metal-porcelain interface is due to the disparity between the coefficient of thermal expansion of the metal and porcelain. [19] A slightly lower coefficient of thermal expansion of porcelain compared with metal is considered beneficial. Such a relationship places the porcelain under compres- sion after firing [20]. Generally, a 0.5 × 10−6˚C difference in the coefficients is desirable [21]. 2.3. Ceramic Build-Up and Firing Technique Evans et al. [22] highly recommended minimizing air entrapment between the ceramic particles because poros- ity does occur during ceramic application and can ac- count for eventual ceramic fracture. Cracks within ceramics may form due to incomplete densification which leaves behind angular pores. Flaws (cracks) also form in the surface of ceramics through abrasion (by dust); such cracks, coupled with low frac- ture toughness, impair the strength of ceramics [23]. The rate of cooling and heating during porcelain firing may also affect the stress concentration at the metal-ce- ramic interface [24]. Repeated firings or excessively high oven tempera- tures have been regarded as causes of superficial and deep imperfections or porcelain blistering [25]. 2.4. Thickness of Porcelain It has been stated that “the thicker the porcelain the weaker the restoration.” The reasons behind this state- ment are: (1) the direct relationship between the thick- ness of the porcelain and the stress concentration at the metal-porcelain interface; and (2) the inherent weakness of the porcelain under tension [19]. The porcelain adja- cent to the interface is generally under compression be- cause the metal contracts more than the porcelain; how- ever, the further the surface of the porcelain is from the interface, the greater the tension [14]. Therefore, in order to minimize the formation of microcracks, a fairly uni- form thickness of porcelain is recommended [2]. 2.5. Thickness and Elastic Modulus of the Metal Substructure It has been demonstrated that the support of the veneer- ing porcelain is directly related to the modulus of elastic- Copyright © 2013 SciRes. OPEN ACCESS 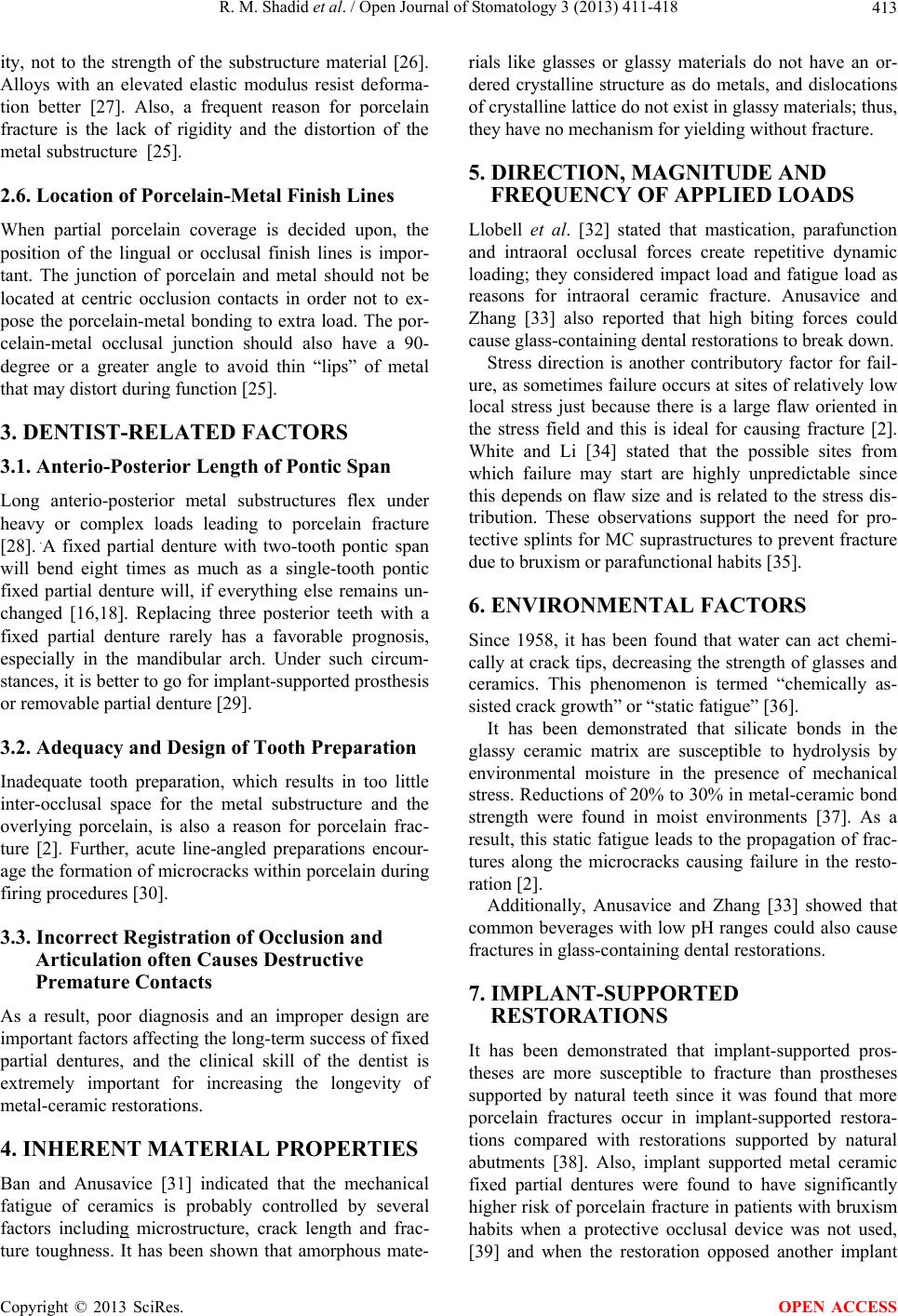 R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 413 ity, not to the strength of the substructure material [26]. Alloys with an elevated elastic modulus resist deforma- tion better [27]. Also, a frequent reason for porcelain fracture is the lack of rigidity and the distortion of the metal substructure [25]. 2.6. Location of Porcelain-Metal Finish Lines When partial porcelain coverage is decided upon, the position of the lingual or occlusal finish lines is impor- tant. The junction of porcelain and metal should not be located at centric occlusion contacts in order not to ex- pose the porcelain-metal bonding to extra load. The por- celain-metal occlusal junction should also have a 90- degree or a greater angle to avoid thin “lips” of metal that may distort during function [25]. 3. DENTIST-RELATED FACTORS 3.1. Anterio-Posterior Length of Pontic Span Long anterio-posterior metal substructures flex under heavy or complex loads leading to porcelain fracture [28]. .A fixed partial denture with two-tooth pontic span will bend eight times as much as a single-tooth pontic fixed partial denture will, if everything else remains un- changed [16,18]. Replacing three posterior teeth with a fixed partial denture rarely has a favorable prognosis, especially in the mandibular arch. Under such circum- stances, it is better to go for implant-supported prosthesis or removable partial denture [29]. 3.2. Adequacy and Design of Tooth Preparation Inadequate tooth preparation, which results in too little inter-occlusal space for the metal substructure and the overlying porcelain, is also a reason for porcelain frac- ture [2]. Further, acute line-angled preparations encour- age the formation of microcracks within porcelain during firing procedures [30]. 3.3. Incorrect Registration of Occlusion and Articulation often Causes Destructive Premature Contacts As a result, poor diagnosis and an improper design are important factors affecting the long-term success of fixed partial dentures, and the clinical skill of the dentist is extremely important for increasing the longevity of metal-ceramic restorations. 4. INHERENT MATERIAL PROPERTIES Ban and Anusavice [31] indicated that the mechanical fatigue of ceramics is probably controlled by several factors including microstructure, crack length and frac- ture toughness. It has been shown that amorphous mate- rials like glasses or glassy materials do not have an or- dered crystalline structure as do metals, and dislocations of crystalline lattice do not exist in glassy materials; thus, they have no mechanism for yielding without fracture. 5. DIRECTION, MAGNITUDE AND FREQUENCY OF APPLIED LOADS Llobell et al. [32] stated that mastication, parafunction and intraoral occlusal forces create repetitive dynamic loading; they considered impact load and fatigue load as reasons for intraoral ceramic fracture. Anusavice and Zhang [33] also reported that high biting forces could cause glass-containing dental restorations to break down. Stress direction is another contributory factor for fail- ure, as sometimes failure occurs at sites of relatively low local stress just because there is a large flaw oriented in the stress field and this is ideal for causing fracture [2]. White and Li [34] stated that the possible sites from which failure may start are highly unpredictable since this depends on flaw size and is related to the stress dis- tribution. These observations support the need for pro- tective splints for MC suprastructures to prevent fracture due to bruxism or parafunctional habits [35]. 6. ENVIRONMENTAL FACTORS Since 1958, it has been found that water can act chemi- cally at crack tips, decreasing the strength of glasses and ceramics. This phenomenon is termed “chemically as- sisted crack growth” or “static fatigue” [36]. It has been demonstrated that silicate bonds in the glassy ceramic matrix are susceptible to hydrolysis by environmental moisture in the presence of mechanical stress. Reductions of 20% to 30% in metal-ceramic bond strength were found in moist environments [37]. As a result, this static fatigue leads to the propagation of frac- tures along the microcracks causing failure in the resto- ration [2]. Additionally, Anusavice and Zhang [33] showed that common beverages with low pH ranges could also cause fractures in glass-containing dental restorations. 7. IMPLANT-SUPPORTED RESTORATIONS It has been demonstrated that implant-supported pros- theses are more susceptible to fracture than prostheses supported by natural teeth since it was found that more porcelain fractures occur in implant-supported restora- tions compared with restorations supported by natural abutments [38]. Also, implant supported metal ceramic fixed partial dentures were found to have significantly higher risk of porcelain fracture in patients with bruxism habits when a protective occlusal device was not used, [39] and when the restoration opposed another implant Copyright © 2013 SciRes. OPEN ACCESS  R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 414 supported metal ceramic restorations [40]. This is because the natural teeth and their periodontal ligaments provide proprioception and early detection of occlusal loads and interferences, while the implants lack this proprioceptive mechanism [41-43]. In addition to loss of shock absorbing feature in the ankylosed implant bone interface, both sensitivity and mobility of natural teeth cannot be duplicated in endosseous implants [44-46]. Therefore this different behavior to masticatory forces may lead to excessive load on the restoration especially if the prosthesis is supported by an implant at one end and a tooth at the other end. Complications of the supra- structure such as fracture of veneering porcelain, and others were observed in 5% - 90% of cases of tooth-im- plant connection [47]. However, it was demonstrated that the use of non-rigid connector decreases the forces on the suprastructure [47]. Screw-Retained Implant-Supported Restorations Since retrievability is an important factor for implant- supported restorations to allow for their easy and safe removal; therefore, the prosthodontic components can be adjusted, the screws can be refastened, and the fractured components can be repaired [48], screw-retained restora- tions are preferred by some clinicians and are recom- mended in some clinical situations [49]. However, it has been shown that the presence of screw-access opening in the occlusal surface of the res- torations significantly decreased porcelain fracture strength [49-56]. This is because the centric contact of the screw-access hole, which is usually developed with the head of the screw or with composite restorative material, may oc- cupy 50% to 66% of the intercuspal occlusal table [57]. Hence, a minimal width of porcelain remains around the screw-access opening and thus, becomes more suscepti- ble to fracture [53]. In addition, it has been shown that the screw-access hole of the screw-retained restoration disrupts the structural continuity of porcelain, thereby modifying the position of the center of mass of the ce- ramic bulk toward which the ceramic shrinks during the sintering process. This will affect the behavior of porce- lain in these restorations compared with their cemented counterparts [58]. 8. POSTERIOR CANTILEVERED PROSTHESES Relatively few studies have been published on the long term efficacy of cantilever bridge work supported by natural teeth. Randow et al. [59] reported a higher fre- quency of failure with cantilevered units than bounded units; the same was stated by Strub et al. [60] who found out that the technical failure rate for cantilever bridges was 12.7% in patients with low-grade periodontitis. Similarly, posterior cantilevered prostheses supported by a relatively small number of implants, seem to be par- ticularly susceptible to fracture[61]. Technical complica- tions (including porcelain fracture) were found to be more frequent for cantilever implant -supported prosthesis than for end implant abutment-supported one [62-64]. Therefore, to increase the success rate of cantilever fixed partial dentures, the leverage effect must be mini- mized by decreasing the pontic size to as small as possi- ble representing a premolar [15,61]. Also, the pontic should possess maximum occluso-gingival height to en- sure rigidity [15]. In addition, considering the different biomechanical demands for cantilever fixed partial den- tures, various occlusal schemes have been advocated; such as freedom in the retrusion/protrusion range on can- tilever, anterior guided lateral movements, and the ab- sence of non-working side contacts on the cantilever [65]. Also, optimal retention from abutments were also rec- ommended [65]. However, in implant-supported cantilever fixed partial dentures, further precautions must be taken into consid- eration. Clinical experiences suggest that the distal can- tilever should not extend more than 2.5 times the anterior posterior spread of the implants under ideal conditions (e.g. no parafunction, no bruxism) [66]. Several biome- chanical studies using an analytical mathematical models [67] and finite element analysis [68] demonstrated that a spread out arrangement of implants in the arch is more significant than the number of implants per se for the distribution of masticatory forces especially if these im- plants will support cantilever prosthesis. In addition to this, the inclination of distal implants reduces the axial force and bending moments independently from the number of abutments when cantilever is needed. This inclination allows simultaneous reduction of the cantile- ver length at the connection abutment-framework and increases the prosthesis support area [69]. Bevilacqua et al. stated that tilted distal implants with consequent re- duction of the posterior cantilevers resulted in decreased stress values for the metal frameworks by 11.5% for 15-degree configuration, 31.3% for 30-degree configure- tion, and 85.6% for the 45-degree configuration [70]. Figures 1 and 2 summarize all of the factors affecting the fracture resistance of metal-ceramic restorations in marco-level and micro-level. 9. CONCLUSION The published literature revealed that many different factors may cause fracture of metal-ceramic tooth-sup- ported and implant-supported restorations. These factors may be related to the technician, dentist, environment, design of the restoration, or to inherent structure of ce- Copyright © 2013 SciRes. OPEN ACCESS  R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 415 Figure 1. Macro-level variables affecting fracture resistance of metal-ceramic restorations. These include: Tooth preparations A (adequate tooth preparation, sufficient inter-occlusal space, rounded line-angles of preparations); Support type B (Tooth vs. implant); Surface integrity of crown C (screw vs. cement-ret- ained); Occlusion factors D (avoidance of premature contacts, design cusps to guide occlusal forces in favorable directions, avoidance of parafunctions and bruxism/clenching habits); Connector variables E (the cross-sectional shape, dimensions, contours of connections within framework); Pontic variables (the occluso-gingival height, occlusal table area, length of pon- tic span); Partial coverage variables (location of porcelain- metal finish lines away from occlusal loads); Cantilever vari- ables F (posterior length of cantilever in relation to support span, occlusal engagement vs freedom of movement, direction of forces on cantilever area, width of occlusal table area of cantilevered section, occluso-gingival height); Diet variables G (beverages with low pH ranges, biting hard food or structures accidently or habitually). Figure 2. Micro-level variables affecting fracture resistance of metal-ceramic Restorations. These include: Metal variables (thickness A, roughness B); Oxide layer variables (presence, thickness, uniformity C, surface roughness D, wetting ability); Metal-porcelain junction variables (rounded internal angles E, 90-degree or a greater external angles at porcelain-metal junc- tion F); Porcelain layer variables (various thickness at different locations not exceed 2 mm G; Smoothness and polishing of surface H); Physical properties (compatibility between coeffi- cient of thermal expansion of metal and porcelain CTE, elastic modulus of metal EM, mechanical fatigue resistance of porce- lain, static fatigue resistance of porcelain under humidity); Porcelain impurities (air voids J, cracks internal K, or external L, dust impurity M); Porcelain firing procedures (rate of cool- ing and heating N, Number of repeated firings O, excessively high oven temperatures P). ramics and others. Straussberg et al. [71] said: “to obtain the optimum results inherent in porcelain-fused-to-gold restorations, the dentist must understand and respect the physical characteristics of the materials and guide the design and fabrication of the restoration so as to exploit their strengths and compensate for their weaknesses.” REFERENCES [1] Walton, T.R. (2002) An up to 15-year longitudinal study of 515 metal-ceramic FPDs: Part 1. Outcome. Interna- tional Journal of Prosthodontics, 15, 439-445. [2] Ozcan, M. (2003) Fracture reasons in ceramic-fused- to-metal restorations. Journal of Oral Rehabilitation, 30, 265-269. http://dx.doi.org/10.1046/j.1365-2842.2003.01038.x [3] Singer, A. and Serfaty, V. (1996) Cement-retained im- plant-supported fixed partial dentures: A 6-month to 3-year follow-up. International Journal of Oral & Max- illofacial Implants, 11, 645-649. [4] Strub, J.R., Stiffler, S. and Scharer, P. (1988) Cause of failure following oral rehabilitation: Biological versus technical factors. Quintessence International, 19, 215- 222. [5] Walton, J.N., Gardner, F.M. and Agar J.R. (1986) A sur- vey of crown and fixed partial denture failures: length of service and reasons for replacement. Journal of Pros- thetic Dentistry, 56, 416-421. http://dx.doi.org/10.1016/0022-3913(86)90379-3 [6] Bragger, U., Karoussis, I., Persson, R., et al. (2005) Tech- nical and biological complications/failures with single crowns and fixed partial dentures on implants: A 10-year prospective cohort study. Clinical Oral Implants Re- search, 16, 326-334. http://dx.doi.org/10.1111/j.1600-0501.2005.01105.x [7] Goodacre, C.J., Bernal, G., Rungcharassaeng, K., et al. (2003) Clinical complications in fixed prosthodontics. Journal of Prosthetic Dentistry, 90, 31-41. http://dx.doi.org/10.1016/S0022-3913(03)00214-2 [8] Zarb, G.A. and Smith, A. (1990) The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto study. Part III: Problems and complications en- countered. Journal of Prosthetic Dentistry, 64, 185-194. http://dx.doi.org/10.1016/0022-3913(90)90177-E [9] Ekfeldt, A., Carlsson, G.E. and Borjesson G. (1994) Clinical evaluation of single-tooth restorations supported by osseointegrated implants: A retrospective study. In- ternational Journal of Oral & Maxillofacial Implants, 9, 179-183. [10] Warpeha, W.S. and Goodkind, R.J. (1976) Design and technique variables affecting fracture resistance of metal- ceramic restorations. Journal of Prosthetic Dentistry, 35, 291-298. http://dx.doi.org/10.1016/0022-3913(76)90253-5 [11] Anthony, D.H., Burnett, A.P., Smith, D.L., et al. (1970) Shear test for measuring bonding in cast gold alloy-por- celain composites. Journal of Dental Research, 49, 27-33. Copyright © 2013 SciRes. OPEN ACCESS  R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 416 http://dx.doi.org/10.1177/00220345700490012601 [12] Craig, R.G. and Powers, J.M. (2002) Restorative dental materials. 11th edition. Mosby, St. Louis, 580. [13] Kelly, M., Asgar, K. and O’Brien, W.J. (1969) Tensile strength determination of the interface between porcelain fused to gold. Journal of Biomedical Materials Research, 3, 403-408. http://dx.doi.org/10.1002/jbm.820030302 [14] Shell, J.S. and Nielsen, J.P. (1962) Study of the bond between gold alloys and porcelain. Journal of Dental Re- search, 41, 1424-1437. http://dx.doi.org/10.1177/00220345620410062101 [15] Riley, E.J. (1977) Ceramo-metal restoration. State of the science. Dental Clinics of North America, 21, 669-682. [16] Shillingburg, H.T., Hobo, S., Whitsett, L.D., Jacobi, R. and Brackett, S.E. (1997) Fundamentals of fixed prost- hodontics, 3rd edition, Quintessence Publishing Co, Chi- cago, 89-94. [17] Caputo, A.A. and Standlee, J.P. (1987) Biomechanics in clinical dentistry. Quintessence Publishing Co., Inc., Chi- cago, 123-149. [18] Palmqvist, S. and Soderfeldt, B. (1994) Multivariate analyses of factors influencing the longevity of fixed par- tial dentures, retainers, and abutments. Journal of Pros- thetic Dentistry, 71, 245-250. http://dx.doi.org/10.1016/0022-3913(94)90462-6 [19] Tuccillo, J.J. and Nielsen, J.P. (1972) Shear stress meas- urements at a dental porcelain-gold bond interface. Jour- nal of Dental Research, 51, 626-633. http://dx.doi.org/10.1177/00220345720510026301 [20] Pang, I.C., Gilbert, J.L., Chai, J., et al. (1995) Bonding characteristics of low-fusing porcelain bonded to pure ti- tanium and palladium-copper alloy. Journal of Prosthetic Dentistry, 73, 17-25. http://dx.doi.org/10.1016/S0022-3913(05)80267-7 [21] Craig, R.G. (1993) Restorative dental materials. 9th ed. Mosby, St. Louis, 492. [22] Evans, D., Barghi, N., Malloy C, et al. (1990) The influ- ence of condensation method on porosity and body por- celain. Journal of Prosthetic Dentistry, 63, 380-389. http://dx.doi.org/10.1016/0022-3913(90)90224-Z [23] Ritter, J.E. (1995) Predicting lifetimes of materials and material structures. Dental Materials, 11, 142-146. http://dx.doi.org/10.1016/0109-5641(95)80050-6 [24] Nielsen, J.P. and Tuccillo, J.J. (1972) Calculations of interfacial stress in dental porcelain bonded to gold alloy substrate. Journal of Dental Research, 51, 1043-47. http://dx.doi.org/10.1177/00220345720510040901 [25] Barreto, M.T. (1984) Failure in ceramometal fixed resto- rations. Journal of Prosthetic Dentistry, 51, 186-189. http://dx.doi.org/10.1016/0022-3913(84)90256-7 [26] Campbell, S.D. (1989) A comparative strength study of metal ceramic and all-ceramic esthetic materials: Mo- dulus of rupture. Journal of Prosthetic Dentistry, 62, 476- 479. http://dx.doi.org/10.1016/0022-3913(89)90184-4 [27] Suansuwan, S. and Swain, M. (1999) New approach for evaluating metal porcelain interfacial bonding. Interna- tional Journal of Prosthodontics, 12, 547-552. [28] Reuter, J.E. and Brose, M.O. (1984) Failures in full crown retained dental bridges. British Dental Journal, 157, 61-63. http://dx.doi.org/10.1038/sj.bdj.4805411 [29] Rosenstiel, S.F., Land, M.F. and Fujimoto, J. (2001) Con- temporary fixed prosthodontics, 3rd edition. Mosby, St Louis, 73. [30] Burke, F.J. (1996) Fracture resistance of teeth restored with dentin-bonded crowns: the effect of increased tooth preparation. Quintessence International, 27, 115-121. [31] Ban, S. and Anusavice, K.J. (1990) Influence of test method on failure stress of brittle dental materials. Jour- nal of Dental Research, 69, 1791-1799. http://dx.doi.org/10.1177/00220345900690120201 [32] Llobell, A., Nichlls, J.I., Kois, J.C., et al. (1992) Fatigue life of porcelain repair systems. International Journal of Prosthodontics, 5, 205-213. [33] Anusavice, K.J. and Zhang, N.Z. (1998) Chemical dura- bility of Dicor and fluorocanasite-based glass-ceramics. Journal of Dental Research, 77, 1553-1559. http://dx.doi.org/10.1177/00220345980770071101 [34] White, S.N., Li, Z.C., Yu, Z., et al. (1997) Relationship between static, chemical and cyclic mechanical fatigue in feldspathic porcelain. Dental Materials, 13, 103-110. http://dx.doi.org/10.1016/S0109-5641(97)80019-X [35] Bragger, U., Aeschlimann, S., Burgin, W., et al. (2001) Biological and technical complications and failures with fixed partial dentures (FPD) on implants and teeth after four to five years of function. Clinical Oral Implants Re- search, 12, 26-34. http://dx.doi.org/10.1034/j.1600-0501.2001.012001026.x [36] Charles, R.J. (1958) Static fatigue of glass. II. Journal of Applied Physics, 29, 1554-1560. http://dx.doi.org/10.1063/1.1722992 [37] Sherill, C.A. and O’brein, W.J. (1974) Transverse strength of aluminous and feldspathic porcelain. Journal of Dental Research, 53, 683-690. http://dx.doi.org/10.1177/00220345740530032801 [38] Pjetursson, B.E., Brägger, U., Lang, N.P. and Zwahlen, M. (2007) Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clini- cal Oral Implants Research, 18, 97-113. http://dx.doi.org/10.1111/j.1600-0501.2007.01439.x [39] Kreissl, M.E., Gerds, T., Muche, R., Heydecke, G. and Strub, J.R. (2007) Technical complications of implant- supported fixed partial dentures in partially edentulous cases after an average observation period of 5 years. Clinical Oral Implants Research, 18, 720-726. http://dx.doi.org/10.1111/j.1600-0501.2007.01414.x [40] Kinsel, R.P. and Lin, D. (2009) Retrospective analysis of porcelain failures of metal ceramic crowns and fixed par- tial dentures supported by 729 implants in 152 patients: patient-specific and implant specific predictors of ce- ramic failure. Journal of Prosthetic Dentistry, 101, 388- 394. http://dx.doi.org/10.1016/S0022-3913(09)60083-4 [41] Misch, C.E. (2005) Dental implant prosthetics. Mosby, Inc., St. Louis, 457-475. [42] Keller, D., Hammerle, C.H.F. and Lang, N.P. (1996) Copyright © 2013 SciRes. OPEN ACCESS  R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 417 Thresholds for tactile sensitivity perceived with dental implants remain unchanged during a healing phase of 3 months. Clinical Oral Implants Research, 7, 48-54. http://dx.doi.org/10.1034/j.1600-0501.1996.070106.x [43] Hammerle, C.H.F., Wagner, D., Bragger, U., Lussi, A., Karayiannis, A., Joss, A. and Lang, N.P. (1995) Thres- hold of tactile sensitivity perceived with dental endosse- ous implants and natural teeth. Clinical Oral Implants Re- search, 6, 83-90. http://dx.doi.org/10.1034/j.1600-0501.1995.060203.x [44] Schutle, W. (1995) Implants and the periodontium. In- ternational Dental Journal, 45, 16-26. [45] Jacobs, R. and van Steenberghe, D. (1994) Role of pe- riodontal ligament receptors in the tactile function of teeth: A review. Journal of Periodontal Research, 29, 153-167. http://dx.doi.org/10.1111/j.1600-0765.1994.tb01208.x [46] Manly, R.S., Pfaffman, C., Lathorp, D.D. and Keyser, J. (1952) Oral sensory thresholds of persons with natural and artificial dentitions. Journal of Dental Research, 31, 305-312. http://dx.doi.org/10.1177/00220345520310030201 [47] Hoffmann, O. and Zafiropoulos, G.G. (2012) The Tooth- Implant Connection: A Review. Journal of Oral Implan- tology, 38, 194-200. http://dx.doi.org/10.1563/AAID-JOI-D-10-00071 [48] Chiche, G.J. and Pinault, A. (1991) Considerations for fabrication of implant-supported posterior restorations. The International Journal of Prosthodontics, 4, 37-44. [49] Shadid, R.M. and Sadaqa, N. (2012) A comparison be- tween screw vs. cement retained implant prostheses: A literature review. Journal of Oral Implantology, 38, 298- 307. http://dx.doi.org/10.1563/AAID-JOI-D-10-00146 [50] Shadid, R.M., Abu-Naba’a, L., Al-Omari, W.M., Asfar, K.R. and EI Masoud, B.M. (2011) Effect of an occlusal screw-access hole on the fracture resistance of perma- nently cemented implant crowns: A laboratory study. The International Journal of Prosthodontics, 24, 267-269. [51] Al-Omari, W.M., Shadid, R., Abu-Naba'a, L. and El Ma- soud, B. (2010) Porcelain fracture resistance of screw- retained, cement-retained, and screw-cement-retained im- plant-supported metal ceramic posterior crowns. Journal of Prosthodontics, 19, 263-273. http://dx.doi.org/10.1111/j.1532-849X.2009.00560.x [52] Karl, M., Graef, F., Taylor, T.D. and Heckmann, S.M. (2007) In vitro effect of load cyclingon metal-ceramic cement and screw-retained implant restorations. The Journal of Prosthetic Dentistry, 97, 137-140. http://dx.doi.org/10.1016/j.prosdent.2007.01.001 [53] Torrado, E., Ercoli, C., Al Mardini, M., Graser, G.N., Tallents, R.H. and Cordaro, L. (2004) A comparison of the porcelain fracture resistance of screw-retained and cement-retained implant-supported metal-ceramic crowns. Journal of Prosthetic Dentistry, 91, 532-537. http://dx.doi.org/10.1016/j.prosdent.2004.03.014 [54] Guichet, D.L., Caputo, A.A., Choi, H. and Sorensen, J.A. (2000) Passivity of fit and marginal opening in screw- or cement-retained implant fixed partial denture designs. The International Journal of Oral & Maxillofacial Im- plants, 15, 239-246. [55] Chee, W., Felton, D.A., Johnson, P.F. and Sullivan, D.Y. (1999) Cemented versus screw-retained implant prosthe- ses: Which is better? The International Journal of Oral & Maxillofacial Implants, 14, 137-141. [56] Hebel, K.S. and Gajjar, R.C. (1997) Cement-retained versus screw-retained implant restoration: Achieving op- timal occlusion and esthetics in implant dentistry. Journal of Prosthetic Dentistry, 77, 28-35. http://dx.doi.org/10.1016/S0022-3913(97)70203-8 [57] Vigolo, P., Givani, A., Majzoub, Z. and Cordioli, G. (2004) Cemented versus screw-retained implant-sup- ported single-tooth crowns: A 4-year prospective clinical study. The International Journal of Oral & Maxillofacial Implants, 19, 260-265. [58] Zarone, F., Sorrentino, R., Traini, T., Di lorio, D. and Ca- puti, S. (2007) Fracture resistance of implant-supported screw- versus cement-retained porcelain fused to metal single crowns: SEM fractographic analysis. Dental Mate- rials, 23, 296-301. http://dx.doi.org/10.1016/j.dental.2005.10.013 [59] Randow, K., Glantz, P.O. and Zoger, B. (1986) Technical failures and some related clinical complications in exten- sive fixed prosthodontics. An epidemiological study of long-term clinical quality. Acta Odontologica Scandina- vica, 44, 241-255. http://dx.doi.org/10.3109/00016358608997726 [60] Strub, J.R., Linter, H. and Marinello, C. (1989) Rehabili- tation of partially edentulous patients using cantilever bridges, a retrospective study. The International Journal of Periodontics & Restorative Dentistry, 9, 364-375. [61] Rangert, B., Jemt, T. and Jorneus, L. (1989) Forces and moments on Brånemark implants. The International Jour- nal of Oral & Maxillofacial Implants, 4, 241-247. [62] Pjetursson, B.E., Tan, K., Lang, N.P., Brägger, U., Egger, M. and Zwahlen, M. (2004) A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Cli- nical Oral Implants Research, 15, 667-676. http://dx.doi.org/10.1111/j.1600-0501.2004.01120.x [63] Hälg, G.A., Schmid, J. and Hämmerle, C.H. (2008) Bone level changes at implants supporting crowns or fixed par- tial dentures with or without cantilevers. Clinical Oral Implants Research, 19, 983-990. http://dx.doi.org/10.1111/j.1600-0501.2008.01556.x [64] Zurdo, J., Romão, C. and Wennström, J.L. (2009) Sur- vival and complication rates of implant-supported fixed partial dentures with cantilevers: A systematic review. Clinical Oral Implants Research, 20, 59-66. http://dx.doi.org/10.1111/j.1600-0501.2009.01773.x [65] Laurell, L., Lundgren, D., Falk, H. and Hugoson, A. (1991) Long term prognosis of extensive polyunit canti- levered fixed partial dentures. The Journal of Prosthetic Dentistry, 66, 545-552. http://dx.doi.org/10.1016/0022-3913(91)90521-W [66] Misch, C.E. (2005) Dental implant prosthetics. Mosby, Inc., St. Louis, 317. [67] Skalak, R. (1983) Biomechanical considerations in os- seointegrated prostheses. The Journal of Prosthetic Den- Copyright © 2013 SciRes. OPEN ACCESS  R. M. Shadid et al. / Open Journal of Stomatology 3 (2013) 411-418 Copyright © 2013 SciRes. 418 OPEN ACCESS tistry, 49, 843-848. http://dx.doi.org/10.1016/0022-3913(83)90361-X [68] Bellini, C.M., Romeo, D., Galbusera, F., Taschieri, S., Raimondi, M.T., Zampelis, A. and Francett, L. (2009) Comparison of tilted versus nontilted implant-supported prosthetic designs for the restoration of the edentulous mandible: A biomechanical study. The International Journal of Oral & Maxillofacial Implants, 24, 511-517. [69] Naconecy, M.M., Geremia, T., Cervieri, A., Teixeira, E.R. and Shinka, R.S. (2010) Effect of the number of abut- ments on biomechanics of Brenamark prosthesis with straight and tilted distal implants. Journal of Applied oral Science, 18, 178-185. http://dx.doi.org/10.1590/S1678-77572010000200013 [70] Bevilacqua, M., Tealdo, T., Menini, M., Pera, F., Mosso- lov, A., Drago, C. and Pera, P. (2011) The influence of cantilever length and implant inclination on stress distri- bution in maxillary implant-supported fixed dentures. Journal of Prosthetic Dentistry, 105, 5-13. http://dx.doi.org/10.1016/S0022-3913(10)60182-5 [71] Straussberg, G., Katz, G. and Kuwata, M. (1966) Design of gold supporting structures for fused porcelain restora- tions. The Journal of Prosthetic Dentistry, 16, 928-936. http://dx.doi.org/10.1016/0022-3913(66)90015-1.
|