I. EL-SAYES ET AL. 11
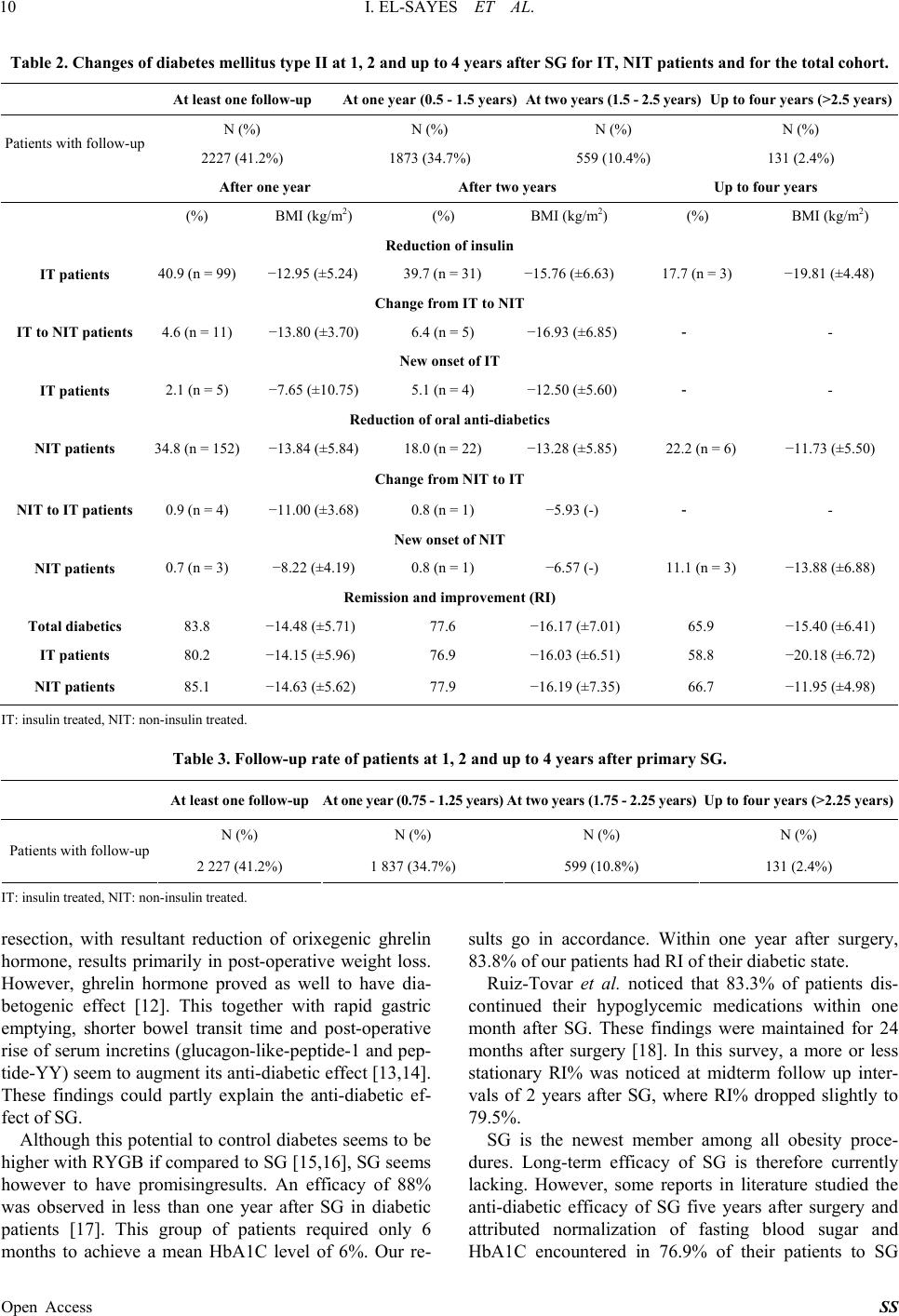
[19]. We noticed that 65.9% of our patients maintained
their diabetes free state with long-term follow up interval
(up to 4 years). Abbatini et al. in analysis of long term ef-
fects of SG noticed an anti-diabetic efficacy, starting by
87.8% one year after surgery, gradually decreasing to
84.6% at two years and further dropped to 76.9% at five
post-operative years. Similarly our cohort showed that
83.8% of patients achieved RI within 1 year after SG.
This percentage dropped gradually to 77.6% at 2 years
and 65.9% up to 4years after operation respectively.
Reports about anti-diabetic efficacy of SG highlighted
a clinical situation of persisting diabetes after operation.
This could be encountered in type 1 insulin treated dia-
betics with autoimmune destruction of pancreatic beta
cells. It is therefore recommended to exclude this condi-
tion before surgery to optimize surgical outcome [20].
Schauer et al. similarly noticed an 87% reduction in the
number of patients requiring oral anti-diabetic medica-
tions after surgery vs. only 79% reduction among the
insulin requiring group [21]. In the same way, NIT pa-
tients in our cohort showed a higher RI% than IT at all
follow up intervals. This difference was statistically not
significant.
Although this report demonstrates in our opinion long
term outcome of a relatively recent surgical procedure,
which is lacking in most published studies, our database
lacks however accurate assessment of pre- and post-op-
erative HbA1C levels. This is a limitation in this survey.
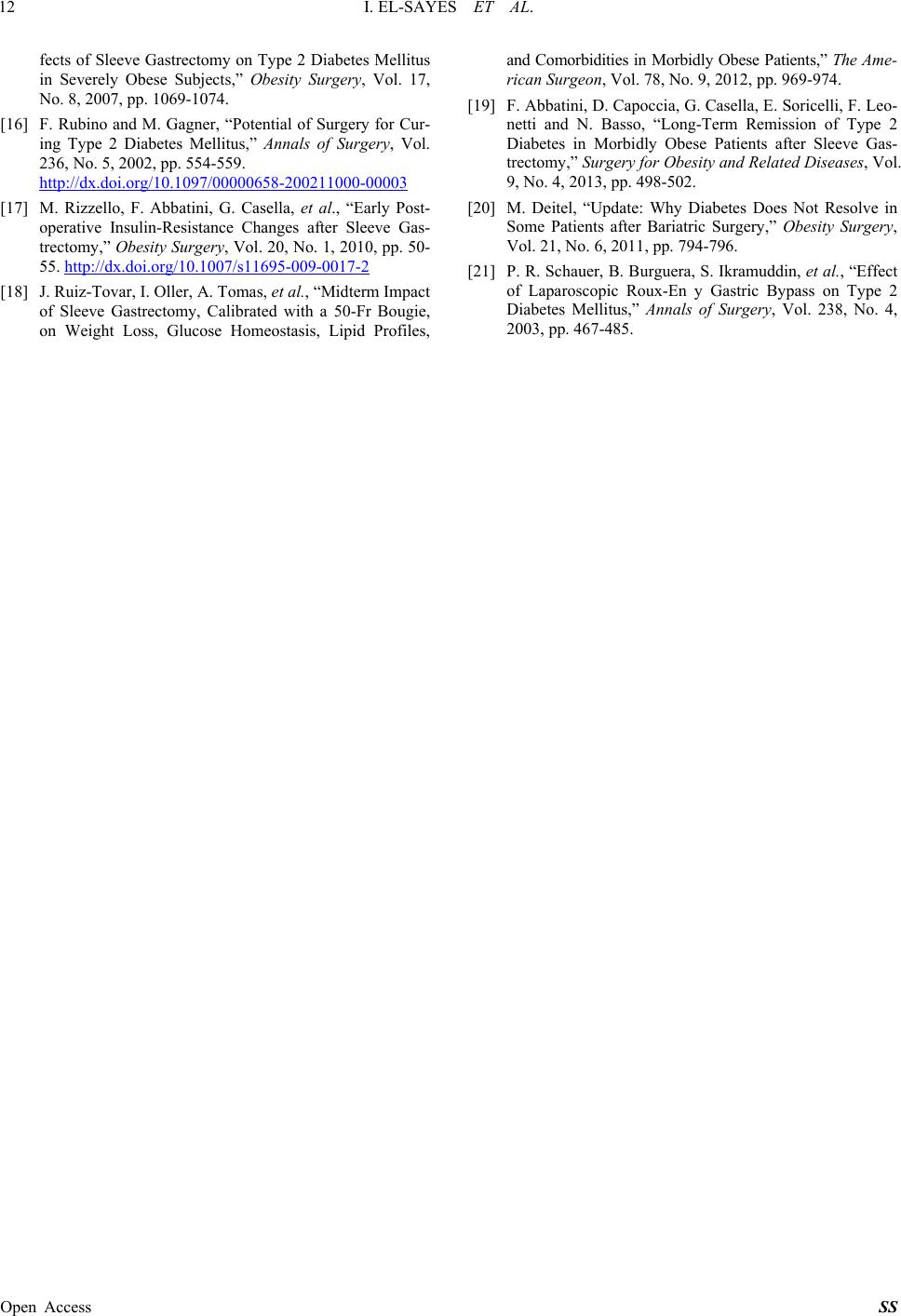
Moreover, the follow up rate for our patients is relatively
low. However, this is attributed to the fact that follow up
of patients is not covered by health insurance service in
Germany.
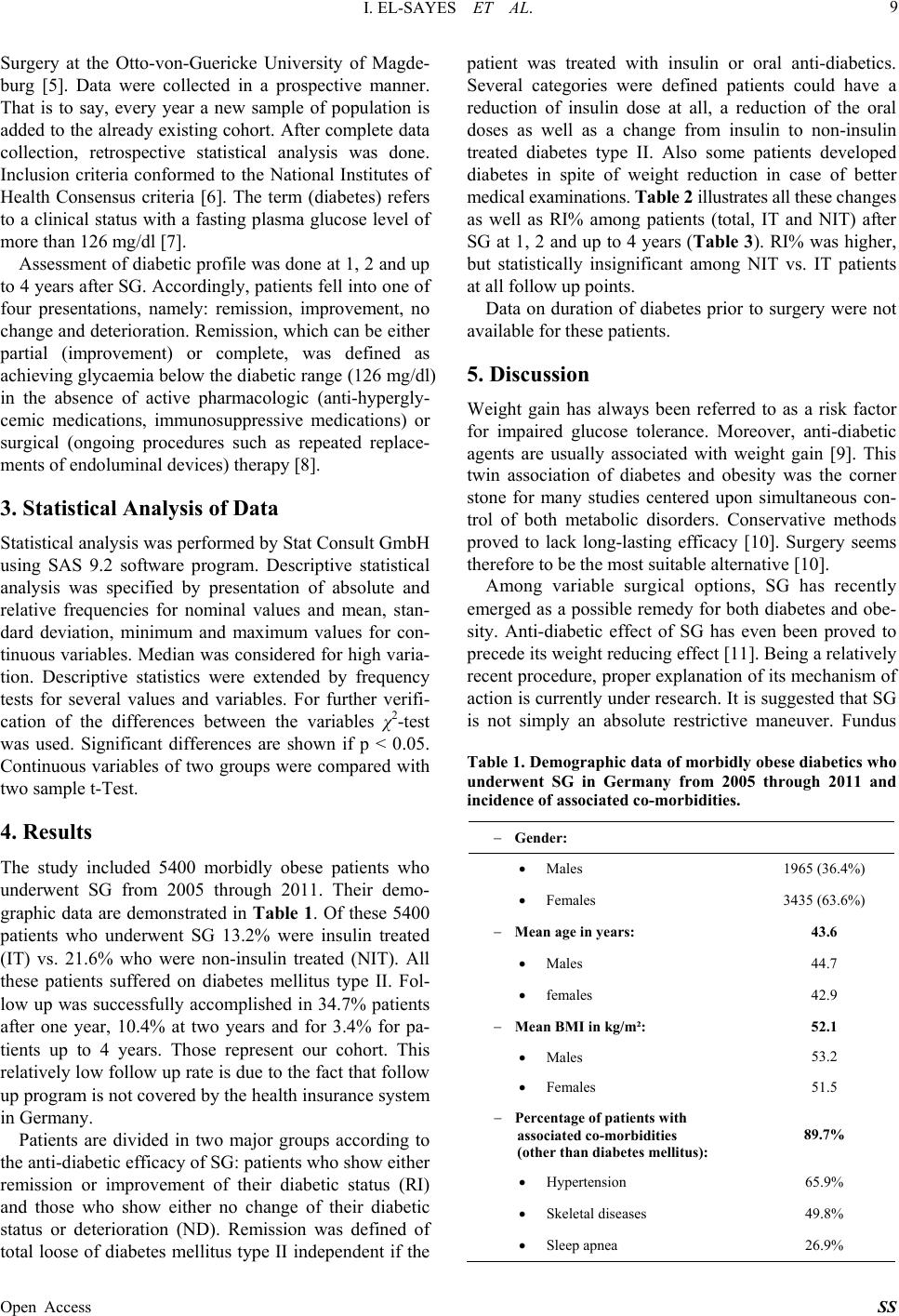
6. Conclusion
In conclusion, SG is rapidly expanding in Germany, due
to its promising results in terms of post-operative weight
loss. Its anti-diabetic efficacy, even in IT patients, seems
also to play a role in its growing popularity. However,
long term assessment of its anti-diabetic efficacy is cur-
rently under evaluation.
7. Acknowledgements
We thank the following firms for financially supporting
the study: Johnson & Johnson MEDICAL GmbH, Ethi-
con Endo-Surgery Deutschland, Norderstedt Covidien Deu-
tschland GmbH, Neustadt/Donau Pharm-Allergan GmbH,
Ettlingen.
REFERENCES
[1] G. Almogy, P. F. Crookes and G. J. Anthone, “Longitu-
dinal Gastrectomy as a Treatment for the High-Risk Su-
per-Obese Patient,” Obesity Surgery, Vol. 14, No. 4, 2004,
pp. 492-497.
http://dx.doi.org/10.1381/096089204323013479
[2] M. Deitel, R. D. Crosby and M. Gagner, “The First Inter-
national Consensus Summit for Sleeve Gastrectomy (SG),
New York City, October 25-27, 2007,” Obesity Surgery,
Vol. 18, No. 5, 2008, pp. 487-496.
http://dx.doi.org/10.1007/s11695-008-9471-5
[3] M. Gagner, M. Deitel, T. L. Kalberer, et al., “The Second
International Consensus Summit for Sleeve Gastrectomy,
March 19-21, 2009,” Surgery for Obesity and Related
Diseases, Vol. 5, No. 4, 2009, pp. 476-485.
[4] M. Daskalakis and R. A. Weiner, “Sleeve Gastrectomy as
a Single-Stage Bariatric Operation: Indications and Limi-
tations,” Obesity Facts, Vol. 2, No. S1, 2009, pp. 8-10.
http://dx.doi.org/10.1159/000198239
[5] C. Stroh, R. Weiner, T. Horbach, K. Adipositas, A. Adi-
positaschirurgie, et al., “New Data on Quality Assurance
in Bariatric Surgery in Germany,” Zentralblatta fur Chi-
rurgie, Vol. 138, No. 2, 2013, pp. 180-188.
[6] “NIH Conference Gastrointestinal Surgery for Severe Obe-
sity. Consensus Development Conference Panel,” Annals
of Internal Medicine, Vol. 115, 1991, pp. 956-961.
[7] American Diabetes Association, “ADA Standards of Me-
dical Care in Diabetes—2009,” Diabetes Care, Vol. 32,
No. S1, 2009, pp. S13-S61.
[8] J. B. Buse, S. Caprio, W. T. Cefalu, et al., “How Do We
Define Cure of Diabetes?” Diabetes Care, Vol. 32, No.
11, 2009, pp. 2133-2135.
[9] F. X. Pi-Sunyer, “The Effects of Pharmacologic Agents
for T2DM on Body Weight,” Postgraduate Medicine, Vol.
120, 2008, pp. 5-17.
http://dx.doi.org/10.3810/pgm.2008.07.1785
[10] B. R. Smith, P. Schauer and N. T. Nguyen, “Surgical Ap-
proaches to the Treatment of Obesity: Bariatric Surgery,”
Endocrinology and Metabolism Clinics of North America,
Vol. 37, No. 4, 2008, pp. 943-964.
http://dx.doi.org/10.1016/j.ecl.2008.08.001
[11] J. S. Todkar, S. S. Shah, P. S. Shah and J. Gangwani,
“Long-Term Effects of Laparoscopic Sleeve Gastrectomy
in Morbidly Obese Subjects with Type 2 Diabetes Melli-
tus,” Surgery for Obesity and Related Diseases, Vol. 6,
No. 2, 2010, pp. 142-145.
http://dx.doi.org/10.1016/j.soard.2009.06.008
[12] M. Dietel, M. Ganger, A. L. Erickson and R. D. Crosby,
“Third International Summit: Current Status of Sleeve
Gastrectomy,” Surgery for Obesity and Related Diseases,
Vol. 7, No. 6, 2012, pp. 749-759.
[13] I. Braghetto, C. Davanzo, O. Korn, et al., “Scintigraphic
Evaluation of Gastric Emptying in Obese Patients Sub-
mitted to Sleeve Gastrectomy Compared to Normal Sub-
jects,” Obesity Surgery, Vol. 19, No. 11, 2009, pp. 1515-
1521.
[14] F. Abbatini, D. Capoccia, G. Casella, F. Coccia, F. Leon-
etti and N. Basso, “Type 2 Diabetes in Obese Patients
with Body Mass Index of 30-35 kg/m2: Sleeve Gastrec-
tomy versus Medical Treatment,” Surgery for Obesity and
Related Diseases, Vol. 8, No. 1, 2012, pp. 20-24.
[15] J. Vidal, A. Ibarzabal, J. Nicolau, et al., “Short-Term Ef-
Open Access SS