Z. W. Huang et al. / Journal of Biosciences and Medicines 1 (2013) 6-10
Copyright © 2013 SciRes. JBM
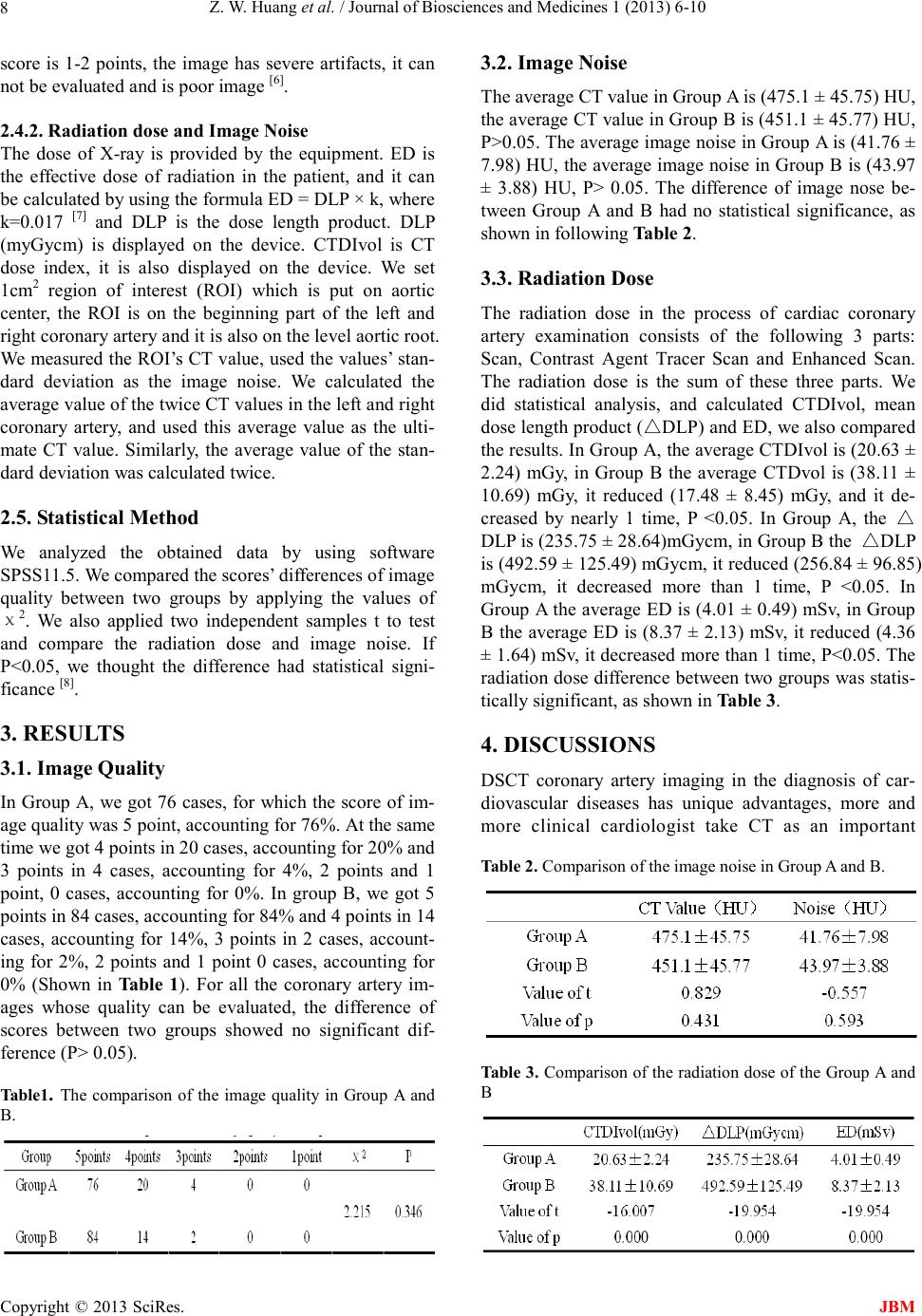
examination tool for non-invasive coronary artery imag-
ing, it can be used as a supplement Cardiovascular Angi-
ography, sometimes it can even replace Cardiovascular
Angiography. In the process of the entire examination of
DSCT, X-ray dose is large, the radiation hazards it pro-
duces gets more and more attention. In order to follow
the principle of ALARA (as low as reasonable achieva-
ble), many scholars have done a lot of research in this
respect, including hardware, software and optimizing
programs of scan, such as Heart Bowtie, ECG Current
Control, Cardiac noise subtraction filter, etc [9]. But the
factors which affect the image quality are complex, some
of these factors are closely related and influence each
other. Some parameter settings may improve the image
quality, but on the other hand, they may reduce the im-
age quality in another aspect. So we must comprehen-
sivel y co ns i de r, and separately set the parameters of scan
according to the different clinical needs. But it is diffi-
cult for us to balance the various factors to obtain
high-quality images in order to improve the diagnostic
rate. Cur ren tl y, the re i s no sta nda rd for q ualit y co ntr ol i n
cor onar y arter y ima gi ng o f Dua l-So urce CT in o ur co un-
try.
So far, people have paid more and more attention to
the potential hazards of ionizing radiation in CT. When
ionizing radiation is wo rk ing on human body, it can
produce biological impacts and do harm to human body.
The break of the structure of DNA double helix in hu-
man body is the critical damage to the cells. Radiation
induces gene mutations or the break of the double helix
structure, the distortion increases, and eventually, the
radiation can lead to cancer [10]. The reports pointed out
that for every more radiation dose of 10mSv, the mortal-
ity rate will increase by 0.04% [11]. The actual radiation
dose of CT examination is 2-5 times the dose of effec-
tive radiation [12]. The dose of effective radiation mainly
comes from the enhanced period. In the aspect of opti-
mizing scanning program, people mostly focus on con-
trolling the radiation dose of enhanced period. In most
cases, the image quality and the radiation dose have the
inverse relationship. To balance the relationship between
them, we need to change the fixed scan mode. In prac-
tical application, we should pay attention to the individ-
ual conditions of the different patients, such as the size
of the heart, breast size of the female patient s and cardi-
othoracic ratio, etc. According to these conditions, we
determine the appropriate scan mode and scan parame-
ters. So we can achieve the personalized and reasonable
scanning. A recent survey, which is an international re-
search for radiation dose in coronary artery CTA, dis-
plays that the radiation dose in different hospitals have
obvi ous gap , fro m an a vera ge of 5 mSv to an a verage of
30 mSv. This demonstrates that reasonable scan mode
can effectively reduce the radiation dose [13]. Therefore,
on the premise that the ima ge quality meets the require-
ments of clinical diagnosis, it becomes important for us
to effectively reduce the radiation dose in the CTA ex-
amination of coronary artery, and this can reduce the
radiation damage caused by human factors.
Reducing the radiation dose is generally divided into
two categorie s: new low-dose technology and optimizing
scan parameters. The new scanning technology uses the
ECG current modulation technique, Prospective ECG
Trigger Scan Technology and noise red uction al gorithms.
The methods of optimizing scan parameters are lowering
tube current, lowering tube voltage, reducing the scan
rage of Z-axis and reducing the number of scans based
on body mass or body mass index (BMI). In this article,
in order to reduce the radiation dose, we used the tech-
nology of regulating the dose of heart electric pulse
(AUTO), and this technology belongs to retrospective
cardiac-gated i magin g techniq ue. T hrough t he stud y and
analysis, we concluded that the regulation technology of
dose of heart electric pulse (AUTO) can make the image
quality completely meets the requirements of clinical
diagnosis, and compared with the conventional full dose
(OFF), thi s techno logy can significa ntly reduce the radi-
ation dose of (4.36 ± 1.64) mSv, the radiation dose de-
creased more than 1 time. Of course, it also has inade-
quacies: 1. Data acqui sition is not ca rried o ut throughout
the whole cardiac cycle, and we can not analyze the car-
diac function. 2. If the patient’s heart rate in unstable, it
is easy for us to select the wrong full-dose regions. 3. In
the non-full-dose exposure regions of the R-R interval,
the image quality is a little bit worse than that of the
image in full-dose regions. 4. If there are heart prema-
ture beats in the scan, we can not edit the ECG.
The study has t he follo wing limitatio ns. T he ind ividu-
alized scan mode according the patient’s BMI was not
adopted, the radiation dose still has some space to be
reduced, a nd i n thi s a sp ec t t he study s ho uld b e c o nti nue d.
If the post-processing of image only uses one of the two
periods in image reconstruction, we can only reconstruct
the image of one period, therefore the radiation dose will
be reduced by 1 time, and in this aspect can be studied
much fur t her.
REFERENCES
[1] Lei ZHUANG, Jihong GAN, Jianjun LIU.
Diagnosis of coronary artery disease by dual source
CT coronary angiography. Medical Journal of
National Defending Forces in Northwest China,
2010, 31 (4): 273-275.
[2] Yuan Zhao, Hong Pu. Comparatively Studying the
Application of Dual Source CT in Coronary