Paper Menu >>
Journal Menu >>
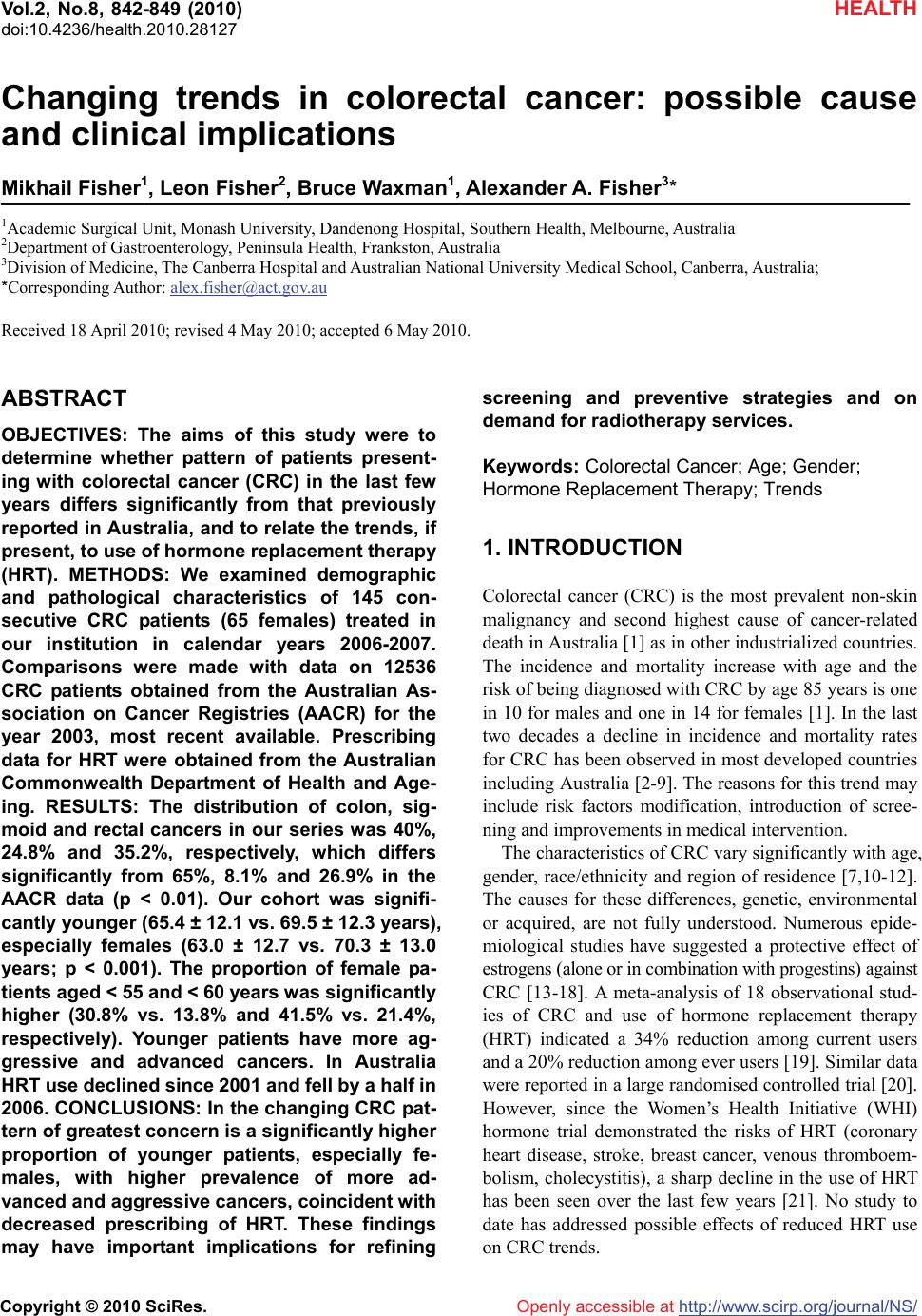 Vol.2, No.8, 842-849 (2010) doi:10.4236/health.2010.28127 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/NS/ HEALTH Changing trends in colorectal cancer: possible cause and clinical implications Mikhail Fisher1, Leon Fisher2, Bruce Waxman1, Alexander A. Fisher3* 1Academic Surgical Unit, Monash University, Dandenong Hospital, Southern Health, Melbourne, Australia 2Department of Gastroenterology, Peninsula Health, Frankston, Australia 3Division of Medicine, The Canberra Hospital and Australian National University Medical School, Canberra, Australia; *Corresponding Author: alex.fisher@act.gov.au Received 18 April 2010; revised 4 May 2010; accepted 6 May 2010. ABSTRACT OBJECTIVES: The aims of this study were to determine whether pattern of patients present- ing with colorectal cancer (CRC) in the last few years differs significantly from that previously reported in Australia, and to relate the trends, if present, to use of hormone replacement therapy (HRT). METHODS: We examined demographic and pathological characteristics of 145 con- secutive CRC patients (65 females) treated in our institution in calendar years 2006-2007. Comparisons were made with data on 12536 CRC patients obtained from the Australian As- sociation on Cancer Registries (AACR) for the year 2003, most recent available. Prescribing data for HRT were obtained from the Australian Commonwealth Department of Health and Age- ing. RESULTS: The distribution of colon, sig- moid and rectal cancers in our series was 40%, 24.8% and 35.2%, respectively, which differs significantly from 65%, 8.1% and 26.9% in the AACR data (p < 0.01). Our cohort was signifi- cantly younger (65.4 ± 12.1 vs. 69.5 ± 12.3 years), especially females (63.0 ± 12.7 vs. 70.3 ± 13.0 years; p < 0.001). The proportion of female pa- tients aged < 55 and < 60 years was significantly higher (30.8% vs. 13.8% and 41.5% vs. 21.4%, respectively). Younger patients have more ag- gressive and advanced cancers. In Australia HRT use declined since 2001 and fell by a half in 2006. CONCLUSIONS: In the changing CRC pat- tern of greatest concern is a significantly higher proportion of younger patients, especially fe- males, with higher prevalence of more ad- vanced and aggressive cancers, coincident with decreased prescribing of HRT. These findings may have important implications for refining screening and preventive strategies and on demand for radiotherapy services. Keywords: Colorectal Cancer; Age; Gender; Hormone Replacement Therapy; Trends 1. INTRODUCTION Colorectal cancer (CRC) is the most prevalent non-skin malignancy and second highest cause of cancer-related death in Australia [1] as in other industrialized countries. The incidence and mortality increase with age and the risk of being diagnosed with CRC by age 85 years is one in 10 for males and one in 14 for females [1]. In the last two decades a decline in incidence and mortality rates for CRC has been observed in most developed countries including Australia [2-9]. The reasons for this trend may include risk factors modification, introduction of scree- ning and improvements in medical intervention. The characteristics of CRC vary significantly with age, gender, race/ethnicity and region of residence [7,10-12]. The causes for these differences, genetic, environmental or acquired, are not fully understood. Numerous epide- miological studies have suggested a protective effect of estrogens (alone or in combination with progestins) against CRC [13-18]. A meta-analysis of 18 observational stud- ies of CRC and use of hormone replacement therapy (HRT) indicated a 34% reduction among current users and a 20% reduction among ever users [19]. Similar data were reported in a large randomised controlled trial [20]. However, since the Women’s Health Initiative (WHI) hormone trial demonstrated the risks of HRT (coronary heart disease, stroke, breast cancer, venous thromboem- bolism, cholecystitis), a sharp decline in the use of HRT has been seen over the last few years [21]. No study to date has addressed possible effects of reduced HRT use on CRC trends. 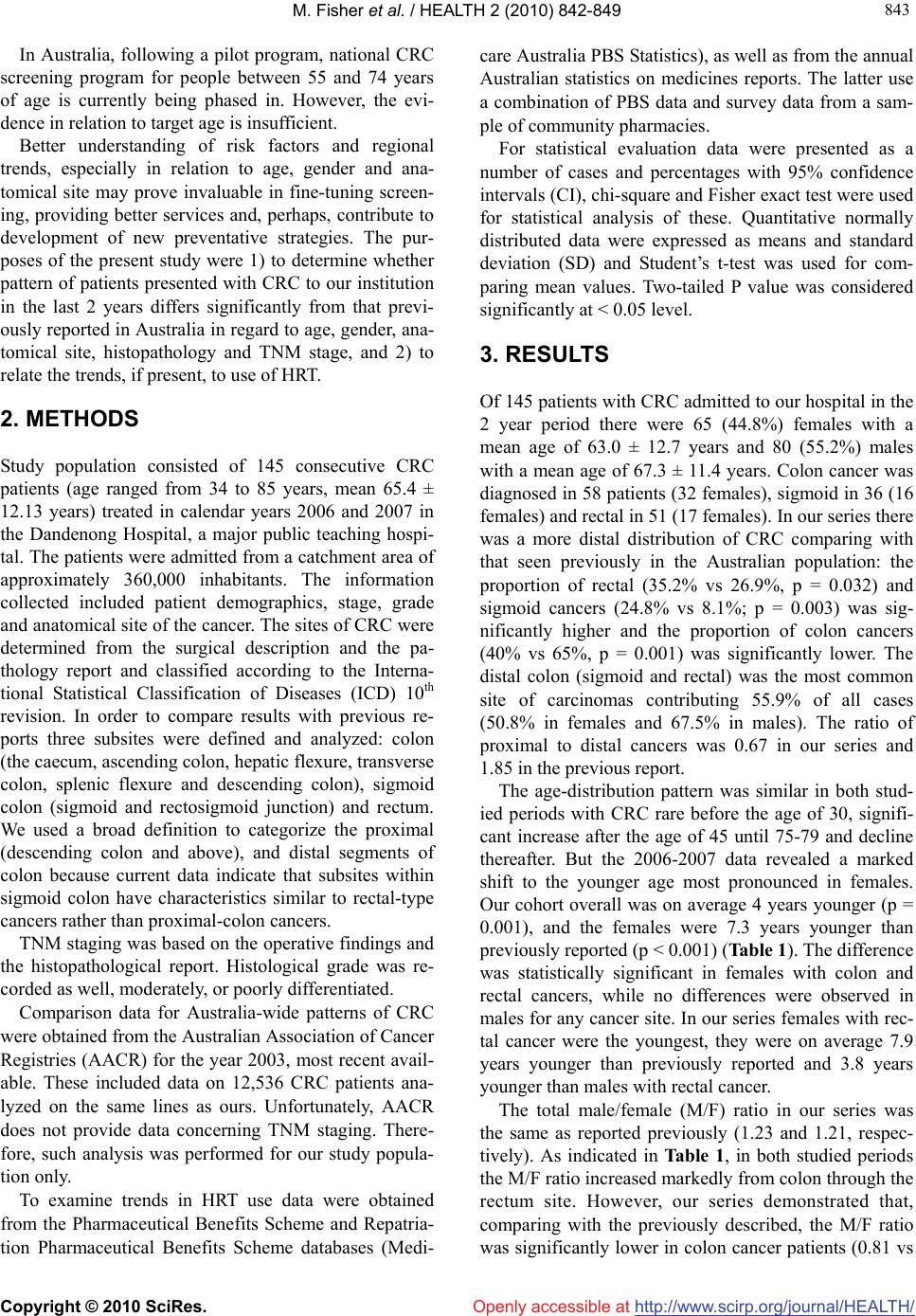 M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 843 843 In Australia, following a pilot program, national CRC screening program for people between 55 and 74 years of age is currently being phased in. However, the evi- dence in relation to target age is insufficient. Better understanding of risk factors and regional trends, especially in relation to age, gender and ana- tomical site may prove invaluable in fine-tuning screen- ing, providing better services and, perhaps, contribute to development of new preventative strategies. The pur- poses of the present study were 1) to determine whether pattern of patients presented with CRC to our institution in the last 2 years differs significantly from that previ- ously reported in Australia in regard to age, gender, ana- tomical site, histopathology and TNM stage, and 2) to relate the trends, if present, to use of HRT. 2. METHODS Study population consisted of 145 consecutive CRC patients (age ranged from 34 to 85 years, mean 65.4 ± 12.13 years) treated in calendar years 2006 and 2007 in the Dandenong Hospital, a major public teaching hospi- tal. The patients were admitted from a catchment area of approximately 360,000 inhabitants. The information collected included patient demographics, stage, grade and anatomical site of the cancer. The sites of CRC were determined from the surgical description and the pa- thology report and classified according to the Interna- tional Statistical Classification of Diseases (ICD) 10th revision. In order to compare results with previous re- ports three subsites were defined and analyzed: colon (the caecum, ascending colon, hepatic flexure, transverse colon, splenic flexure and descending colon), sigmoid colon (sigmoid and rectosigmoid junction) and rectum. We used a broad definition to categorize the proximal (descending colon and above), and distal segments of colon because current data indicate that subsites within sigmoid colon have characteristics similar to rectal-type cancers rather than proximal-colon cancers. TNM staging was based on the operative findings and the histopathological report. Histological grade was re- corded as well, moderately, or poorly differentiated. Comparison data for Australia-wide patterns of CRC were obtained from the Australian Association of Cancer Registries (AACR) for the year 2003, most recent avail- able. These included data on 12,536 CRC patients ana- lyzed on the same lines as ours. Unfortunately, AACR does not provide data concerning TNM staging. There- fore, such analysis was performed for our study popula- tion only. To examine trends in HRT use data were obtained from the Pharmaceutical Benefits Scheme and Repatria- tion Pharmaceutical Benefits Scheme databases (Medi- care Australia PBS Statistics), as well as from the annual Australian statistics on medicines reports. The latter use a combination of PBS data and survey data from a sam- ple of community pharmacies. For statistical evaluation data were presented as a number of cases and percentages with 95% confidence intervals (CI), chi-square and Fisher exact test were used for statistical analysis of these. Quantitative normally distributed data were expressed as means and standard deviation (SD) and Student’s t-test was used for com- paring mean values. Two-tailed P value was considered significantly at < 0.05 level. 3. RESULTS Of 145 patients with CRC admitted to our hospital in the 2 year period there were 65 (44.8%) females with a mean age of 63.0 ± 12.7 years and 80 (55.2%) males with a mean age of 67.3 ± 11.4 years. Colon cancer was diagnosed in 58 patients (32 females), sigmoid in 36 (16 females) and rectal in 51 (17 females). In our series there was a more distal distribution of CRC comparing with that seen previously in the Australian population: the proportion of rectal (35.2% vs 26.9%, p = 0.032) and sigmoid cancers (24.8% vs 8.1%; p = 0.003) was sig- nificantly higher and the proportion of colon cancers (40% vs 65%, p = 0.001) was significantly lower. The distal colon (sigmoid and rectal) was the most common site of carcinomas contributing 55.9% of all cases (50.8% in females and 67.5% in males). The ratio of proximal to distal cancers was 0.67 in our series and 1.85 in the previous report. The age-distribution pattern was similar in both stud- ied periods with CRC rare before the age of 30, signifi- cant increase after the age of 45 until 75-79 and decline thereafter. But the 2006-2007 data revealed a marked shift to the younger age most pronounced in females. Our cohort overall was on average 4 years younger (p = 0.001), and the females were 7.3 years younger than previously reported (p < 0.001) (Table 1). The difference was statistically significant in females with colon and rectal cancers, while no differences were observed in males for any cancer site. In our series females with rec- tal cancer were the youngest, they were on average 7.9 years younger than previously reported and 3.8 years younger than males with rectal cancer. The total male/female (M/F) ratio in our series was the same as reported previously (1.23 and 1.21, respec- tively). As indicated in Table 1, in both studied periods the M/F ratio increased markedly from colon through the rectum site. However, our series demonstrated that, comparing with the previously described, the M/F ratio was significantly lower in colon cancer patients (0.81 vs 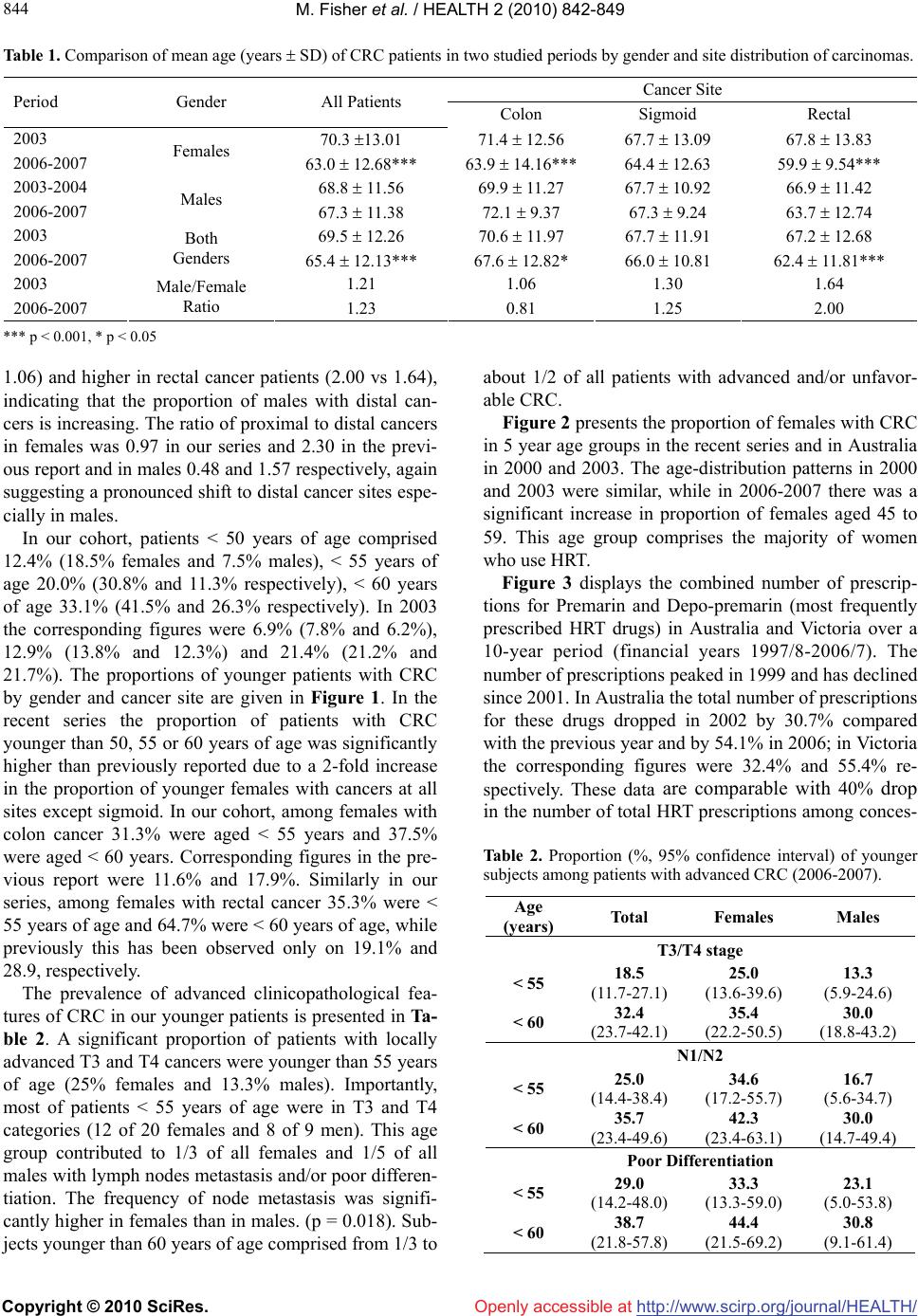 M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 844 Table 1. Comparison of mean age (years SD) of CRC patients in two studied periods by gender and site distribution of carcinomas. Cancer Site Period Gender All Patients Colon Sigmoid Rectal 2003 70.3 13.01 71.4 12.56 67.7 13.09 67.8 13.83 2006-2007 Females 63.0 12.68*** 63.9 14.16***64.4 12.63 59.9 9.54*** 2003-2004 68.8 11.56 69.9 11.27 67.7 10.92 66.9 11.42 2006-2007 Males 67.3 11.38 72.1 9.37 67.3 9.24 63.7 12.74 2003 69.5 12.26 70.6 11.97 67.7 11.91 67.2 12.68 2006-2007 Both Genders 65.4 12.13*** 67.6 12.82* 66.0 10.81 62.4 11.81*** 2003 1.21 1.06 1.30 1.64 2006-2007 Male/Female Ratio 1.23 0.81 1.25 2.00 *** p < 0.001, * p < 0.05 1.06) and higher in rectal cancer patients (2.00 vs 1.64), indicating that the proportion of males with distal can- cers is increasing. The ratio of proximal to distal cancers in females was 0.97 in our series and 2.30 in the previ- ous report and in males 0.48 and 1.57 respectively, again suggesting a pronounced shift to distal cancer sites espe- cially in males. In our cohort, patients < 50 years of age comprised 12.4% (18.5% females and 7.5% males), < 55 years of age 20.0% (30.8% and 11.3% respectively), < 60 years of age 33.1% (41.5% and 26.3% respectively). In 2003 the corresponding figures were 6.9% (7.8% and 6.2%), 12.9% (13.8% and 12.3%) and 21.4% (21.2% and 21.7%). The proportions of younger patients with CRC by gender and cancer site are given in Figure 1. In the recent series the proportion of patients with CRC younger than 50, 55 or 60 years of age was significantly higher than previously reported due to a 2-fold increase in the proportion of younger females with cancers at all sites except sigmoid. In our cohort, among females with colon cancer 31.3% were aged < 55 years and 37.5% were aged < 60 years. Corresponding figures in the pre- vious report were 11.6% and 17.9%. Similarly in our series, among females with rectal cancer 35.3% were < 55 years of age and 64.7% were < 60 years of age, while previously this has been observed only on 19.1% and 28.9, respectively. The prevalence of advanced clinicopathological fea- tures of CRC in our younger patients is presented in Ta- ble 2. A significant proportion of patients with locally advanced T3 and T4 cancers were younger than 55 years of age (25% females and 13.3% males). Importantly, most of patients < 55 years of age were in T3 and T4 categories (12 of 20 females and 8 of 9 men). This age group contributed to 1/3 of all females and 1/5 of all males with lymph nodes metastasis and/or poor differen- tiation. The frequency of node metastasis was signifi- cantly higher in females than in males. (p = 0.018). Sub- jects younger than 60 years of age comprised from 1/3 to about 1/2 of all patients with advanced and/or unfavor- able CRC. Figure 2 presents the proportion of females with CRC in 5 year age groups in the recent series and in Australia in 2000 and 2003. The age-distribution patterns in 2000 and 2003 were similar, while in 2006-2007 there was a significant increase in proportion of females aged 45 to 59. This age group comprises the majority of women who use HRT. Figure 3 displays the combined number of prescrip- tions for Premarin and Depo-premarin (most frequently prescribed HRT drugs) in Australia and Victoria over a 10-year period (financial years 1997/8-2006/7). The number of prescriptions peaked in 1999 and has declined since 2001. In Australia the total number of prescriptions for these drugs dropped in 2002 by 30.7% compared with the previous year and by 54.1% in 2006; in Victoria the corresponding figures were 32.4% and 55.4% re- spectively. These data are comparable with 40% drop in the number of total HRT prescriptions among conces- Table 2. Proportion (%, 95% confidence interval) of younger subjects among patients with advanced CRC (2006-2007). Age (years) Total Females Males T3/T4 stage < 55 18.5 (11.7-27.1) 25.0 (13.6-39.6) 13.3 (5.9-24.6) < 60 32.4 (23.7-42.1) 35.4 (22.2-50.5) 30.0 (18.8-43.2) N1/N2 < 55 25.0 (14.4-38.4) 34.6 (17.2-55.7) 16.7 (5.6-34.7) < 60 35.7 (23.4-49.6) 42.3 (23.4-63.1) 30.0 (14.7-49.4) Poor Differentiation < 55 29.0 (14.2-48.0) 33.3 (13.3-59.0) 23.1 (5.0-53.8) < 60 38.7 (21.8-57.8) 44.4 (21.5-69.2) 30.8 (9.1-61.4) 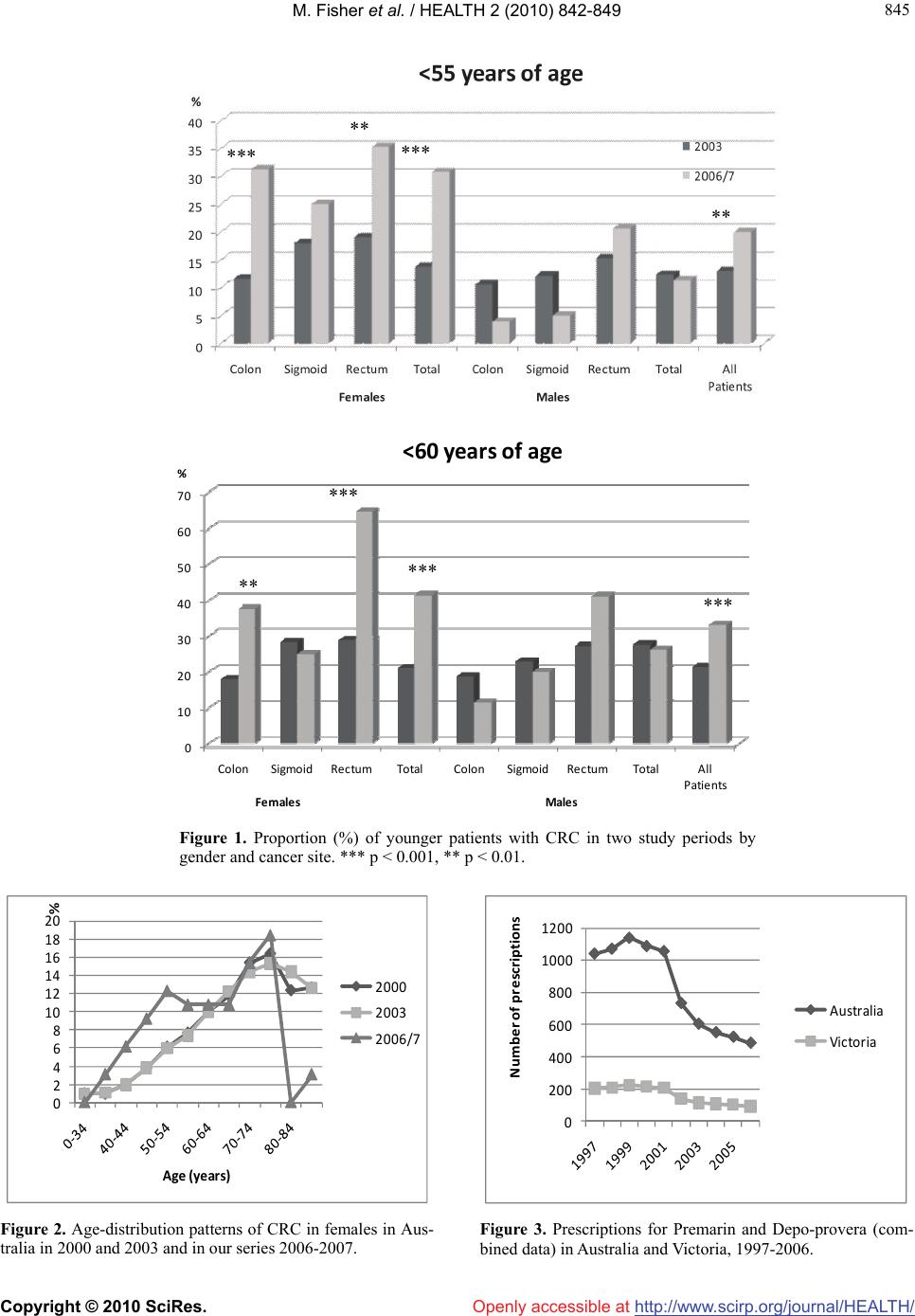 M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/ 845 845 Openly accessible at 0 10 20 30 40 50 60 70 ColonSigmoid RectumTotalColonSigmoid RectumTotalAll Patients % Females Males <60years ofage *** *** *** *** *** ** ** ** Figure 1. Proportion (%) of younger patients with CRC in two study periods by gender and cancer site. *** p < 0.001, ** p < 0.01. 0 2 4 6 8 10 12 14 16 18 20 % Age (years) 2000 2003 2006/7 Figure 2. Age-distribution patterns of CRC in females in Aus- tralia in 2000 and 2003 and in our series 2006-2007. 0 200 400 600 800 1000 1200 Numberofprescriptions Australia Vi ctori a Figure 3. Prescriptions for Premarin and Depo-provera (com- bined data) in Australia and Victoria, 1997-2006.  M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 846 sion cardholders in Australia from 2001 to 2003. In this period a similar decline was observed in prescriptions for estrogen-only preparations (39% decrease), and combined estrogen-progestogen preparations (–41%) [22]. 4. DISCUSSION Our study indicates a change in pattern of CRC occur- rence in 2006-2007. Compared with Australian data for 2003 our experience is of more distal cancers, greater proportion of younger patients, especially females, with high prevalence of more advanced and aggressive tu- mors. Several potential explanations for the changes in CRC characteristics observed in our study should be considered. Cancers of proximal and distal colon might differ in their genetic nature, oncofetal antigen expression and evolve through different pathways and may be associ- ated with distinct risk factors [6,23-29]. Proximal tumors compared to distal ones have a higher proportion of DNA microsatellite instability cancers, are more com- mon in women and older patients. Risk factors for these include high intake of red meat and animal fat, low con- sumption of vegetables and fiber, sedentary life style, obesity and lower socioeconomic status. Alcohol con- sumption and smoking [30-32], use of aspirin and non- steroidal anti-inflammatory drugs (NSAID) [33-35] and especially postmenopausal HRT use [15,19,20,36-40] have also an important influence on CRC risk. Although we cannot fully evaluate the possible effects of all the mentioned risk factors for CRC, it seems unlikely that considerable changes in dietary and lifestyle habits oc- curred in our population between 2003 and 2006-2007. However, one variable which may be relevant, namely, a substantial reduction in HRT use, is obvious. In Australia and Victoria after 2001 prescriptions of Premarin and Depo-provera fell by a third in 2002 and by a half in 2006. A similar rapid and substantial drop in total HRT prescriptions from 2001 to 2003 was reported in Austra- lia and New Zealand [22]. Age and gender-related changes in anatomical subsite CRC distribution observed in our study may be attributed, at least in part, to reduced HRT use after 2001. If hormonal factors protect against CRC then the reduced use of HRT should be accompa- nied by an increase in colon cancers in women during early postmenopausal period, as HRT use is associated mainly with reduced risk of colon cancer [14,15,20, 37,41]. Our experience is consistent with such expecta- tions. This study comparing with previous Australian data clearly demonstrated three points: only females with CRC were significantly younger (on average 7.5 years), there was a substantial increase in proportion of females aged 45 to 59 years who comprise the majority of HRT users and the male predominance in colon cancer was reversed (M/F ratio for colon cancer was 0.81 in 2006- 2007 whereas 1.06 in 2003). Notably, the majority of our younger patients had aggressive and advanced CRC. Previous studies indicated that decrease in estrogen level after menopause increases the risk of a colon cancer with poorer differentiation [11,42]. Our findings are in line with the assumption of an approximate 3-5 year time lag between decrease in HRT use and its impact on CRC incidence rate [21,43,44]. In the Women’s Health Initia- tive (WHI) trial the 38% lower risk of CRC observed in women prescribed HRT during the trial phase disap- peared within 3 years of discontinuing HRT [43]. Numerous epidemiological and experimental studies suggested a favorable influence of HRT on CRC risk. It was estimated that estrogens alone or in combination with progestins reduce colon risk by 20-44% in post- menopausal women, and the duration of HRT did not influence risk estimates [19-21]. In the present study a sharp drop in the HRT use after 2001 was associated with 20.1% increase in the proportion of females < 60 years of age with CRC compared to the 2003 data. If this association is causal a further increase in CRC female patients should be expected. Of interest, the substantial decrease in HRT use was associated with a decline of breast cancer incidence in Australia, US and other coun- tries [22,45,46]. The protective effects of estrogen on colonic carcinogenesis are mediated predominately through estrogen receptor β (ER-β) involving both ge- nomic and non-genomic mechanisms [40]. ER-β-knock- out mice demonstrate hyperproliferation, loss of differ- entiation and disordered apoptosis of colonic mucosa, as well as disorganization of mucin localization, reduction in the number of hemidesmosomes and loss of tight junctions of colonic epithelium [47], indicating that ER- β plays a pivotal role in maintenance of cellular homeo- stasis in the colon. ER-β is the dominant receptor in hu- man colonic mucosa and seems to be essential for pre- venting malignant transformation of colonic epithelial cells. A significant reduction of ER-β expression has been shown in colon adenocarcinoma cells and this cor- related with tumor dedifferentiation, stage and grade [42,48,49]. Moreover, in the pre-malignant phase of co- lon carcinogenesis ER-β expression is also reduced and inversely correlates with increase of proliferative activity in the adenomatous tissue [50]. It has been shown pre- viously that methylation associated inactivation of es- trogen receptor gene in ageing colorectal mucosa is one of the earliest events predisposing to cancerogenesis [51]. Other postulated mechanisms by which HRT use might reduce CRC risk include the influence of estrogens on bile acids [52,53], insulin and glucose control [54]. 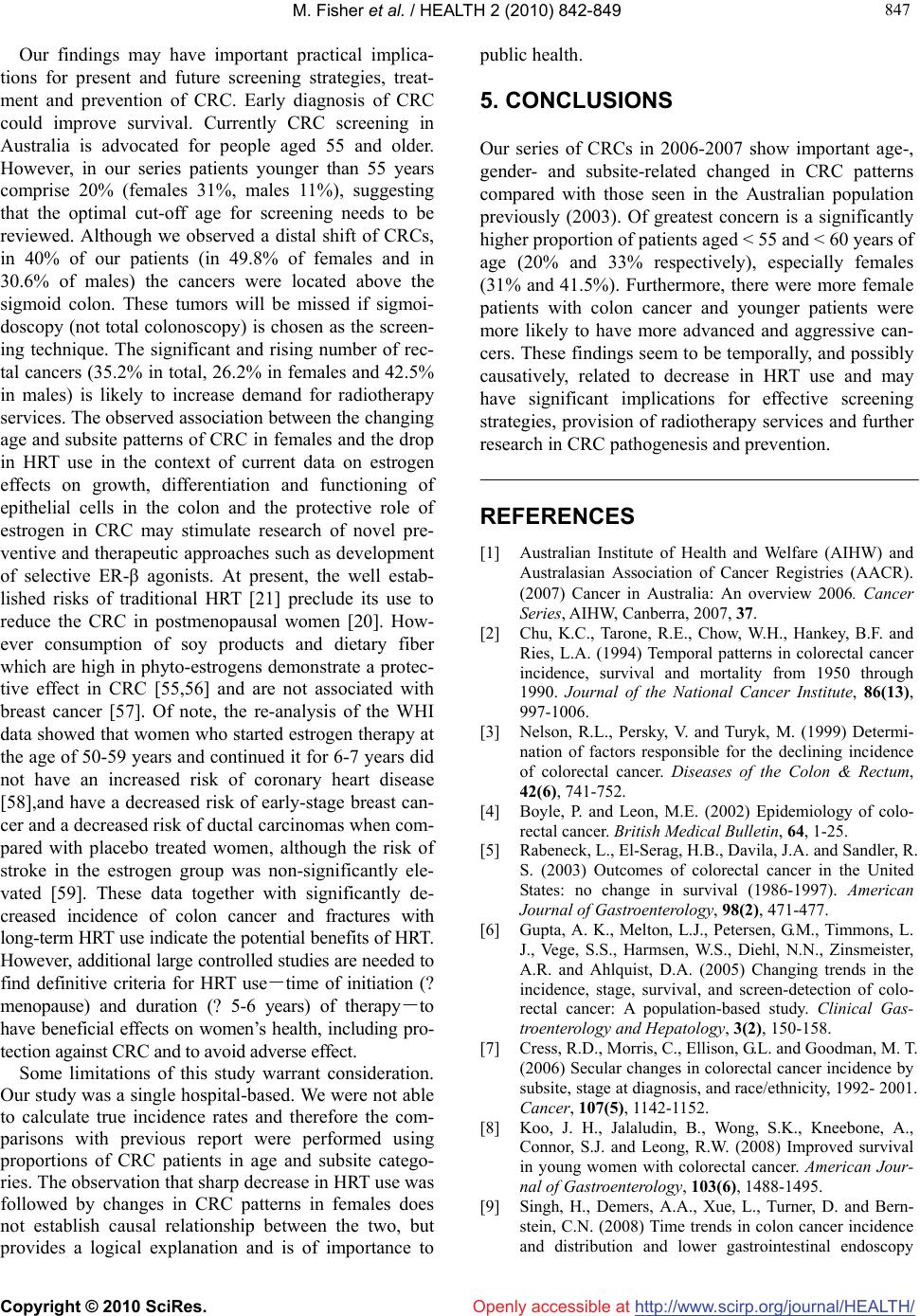 M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/ 847 847 Openly accessible at Our findings may have important practical implica- tions for present and future screening strategies, treat- ment and prevention of CRC. Early diagnosis of CRC could improve survival. Currently CRC screening in Australia is advocated for people aged 55 and older. However, in our series patients younger than 55 years comprise 20% (females 31%, males 11%), suggesting that the optimal cut-off age for screening needs to be reviewed. Although we observed a distal shift of CRCs, in 40% of our patients (in 49.8% of females and in 30.6% of males) the cancers were located above the sigmoid colon. These tumors will be missed if sigmoi- doscopy (not total colonoscopy) is chosen as the screen- ing technique. The significant and rising number of rec- tal cancers (35.2% in total, 26.2% in females and 42.5% in males) is likely to increase demand for radiotherapy services. The observed association between the changing age and subsite patterns of CRC in females and the drop in HRT use in the context of current data on estrogen effects on growth, differentiation and functioning of epithelial cells in the colon and the protective role of estrogen in CRC may stimulate research of novel pre- ventive and therapeutic approaches such as development of selective ER-β agonists. At present, the well estab- lished risks of traditional HRT [21] preclude its use to reduce the CRC in postmenopausal women [20]. How- ever consumption of soy products and dietary fiber which are high in phyto-estrogens demonstrate a protec- tive effect in CRC [55,56] and are not associated with breast cancer [57]. Of note, the re-analysis of the WHI data showed that women who started estrogen therapy at the age of 50-59 years and continued it for 6-7 years did not have an increased risk of coronary heart disease [58],and have a decreased risk of early-stage breast can- cer and a decreased risk of ductal carcinomas when com- pared with placebo treated women, although the risk of stroke in the estrogen group was non-significantly ele- vated [59]. These data together with significantly de- creased incidence of colon cancer and fractures with long-term HRT use indicate the potential benefits of HRT. However, additional large controlled studies are needed to find definitive criteria for HRT use-time of initiation (? menopause) and duration (? 5-6 years) of therapy-to have beneficial effects on women’s health, including pro- tection against CRC and to avoid adverse effect. Some limitations of this study warrant consideration. Our study was a single hospital-based. We were not able to calculate true incidence rates and therefore the com- parisons with previous report were performed using proportions of CRC patients in age and subsite catego- ries. The observation that sharp decrease in HRT use was followed by changes in CRC patterns in females does not establish causal relationship between the two, but provides a logical explanation and is of importance to public health. 5. CONCLUSIONS Our series of CRCs in 2006-2007 show important age-, gender- and subsite-related changed in CRC patterns compared with those seen in the Australian population previously (2003). Of greatest concern is a significantly higher proportion of patients aged < 55 and < 60 years of age (20% and 33% respectively), especially females (31% and 41.5%). Furthermore, there were more female patients with colon cancer and younger patients were more likely to have more advanced and aggressive can- cers. These findings seem to be temporally, and possibly causatively, related to decrease in HRT use and may have significant implications for effective screening strategies, provision of radiotherapy services and further research in CRC pathogenesis and prevention. REFERENCES [1] Australian Institute of Health and Welfare (AIHW) and Australasian Association of Cancer Registries (AACR). (2007) Cancer in Australia: An overview 2006. Cancer Series, AIHW, Canberra, 2007, 37. [2] Chu, K.C., Tarone, R.E., Chow, W.H., Hankey, B.F. and Ries, L.A. (1994) Temporal patterns in colorectal cancer incidence, survival and mortality from 1950 through 1990. Journal of the National Cancer Institute, 86(13), 997-1006. [3] Nelson, R.L., Persky, V. and Turyk, M. (1999) Determi- nation of factors responsible for the declining incidence of colorectal cancer. Diseases of the Colon & Rectum, 42(6), 741-752. [4] Boyle, P. and Leon, M.E. (2002) Epidemiology of colo- rectal cancer. British Medical Bulletin, 64, 1-25. [5] Rabeneck, L., El-Serag, H.B., Davila, J.A. and Sandler, R. S. (2003) Outcomes of colorectal cancer in the United States: no change in survival (1986-1997). American Journal of Gastroenterology, 98(2), 471-477. [6] Gupta, A. K., Melton, L.J., Petersen, G.M., Timmons, L. J., Vege, S.S., Harmsen, W.S., Diehl, N.N., Zinsmeister, A.R. and Ahlquist, D.A. (2005) Changing trends in the incidence, stage, survival, and screen-detection of colo- rectal cancer: A population-based study. Clinical Gas- troenterology and Hepatology, 3(2), 150-158. [7] Cress, R.D., Morris, C., Ellison, G.L. and Goodman, M. T. (2006) Secular changes in colorectal cancer incidence by subsite, stage at diagnosis, and race/ethnicity, 1992- 2001. Cancer, 107(5), 1142-1152. [8] Koo, J. H., Jalaludin, B., Wong, S.K., Kneebone, A., Connor, S.J. and Leong, R.W. (2008) Improved survival in young women with colorectal cancer. American Jour- nal of Gastroenterology, 103(6), 1488-1495. [9] Singh, H., Demers, A.A., Xue, L., Turner, D. and Bern- stein, C.N. (2008) Time trends in colon cancer incidence and distribution and lower gastrointestinal endoscopy 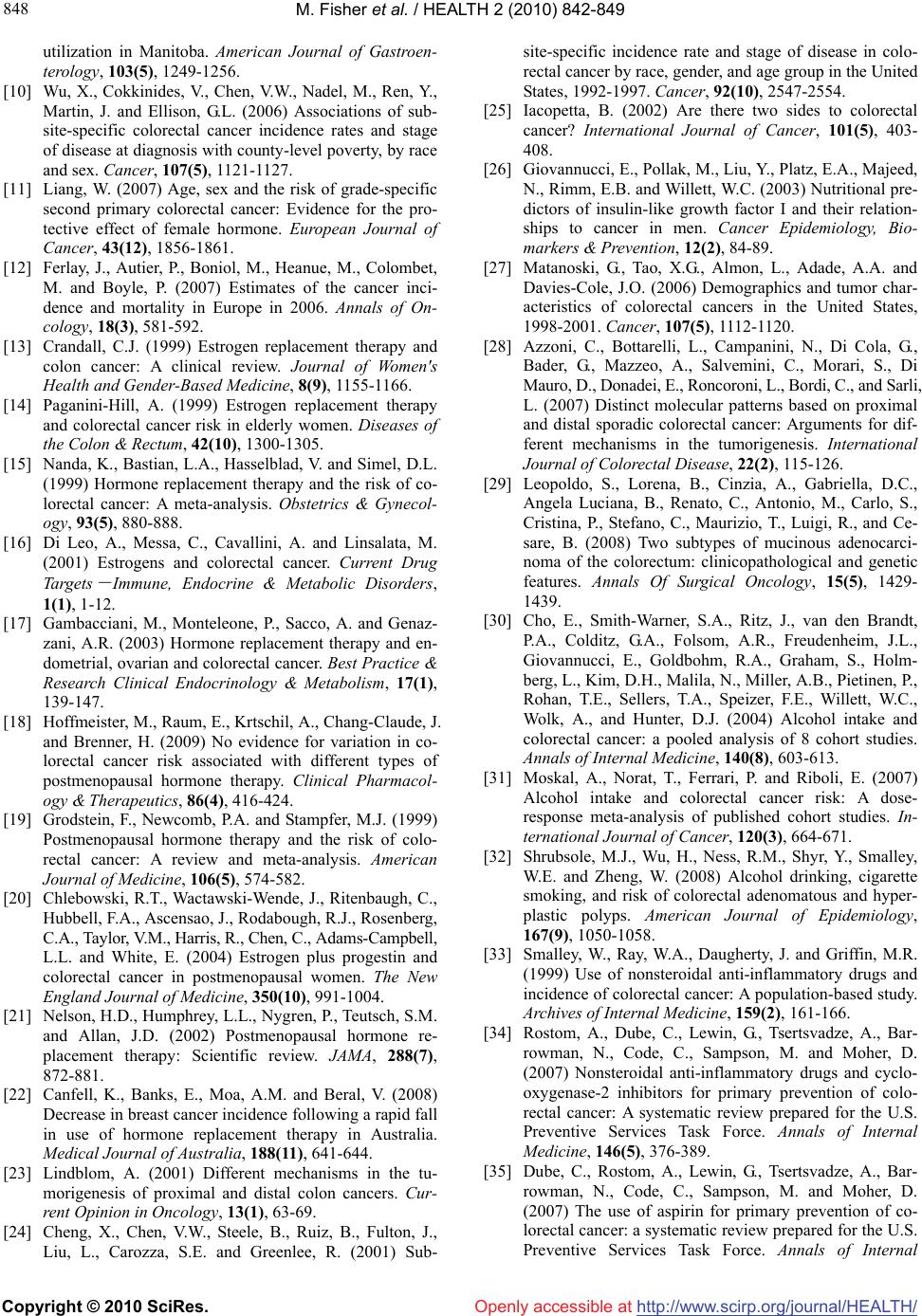 M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 848 utilization in Manitoba. American Journal of Gastroen- terology, 103(5), 1249-1256. [10] Wu, X., Cokkinides, V., Chen, V.W., Nadel, M., Ren, Y., Martin, J. and Ellison, G.L. (2006) Associations of sub- site-specific colorectal cancer incidence rates and stage of disease at diagnosis with county-level poverty, by race and sex. Cancer, 107(5), 1121-1127. [11] Liang, W. (2007) Age, sex and the risk of grade-specific second primary colorectal cancer: Evidence for the pro- tective effect of female hormone. European Journal of Cancer, 43(12), 1856-1861. [12] Ferlay, J., Autier, P., Boniol, M., Heanue, M., Colombet, M. and Boyle, P. (2007) Estimates of the cancer inci- dence and mortality in Europe in 2006. Annals of On- cology, 18(3), 581-592. [13] Crandall, C.J. (1999) Estrogen replacement therapy and colon cancer: A clinical review. Journal of Women's Health and Gender-Based Medicine, 8(9), 1155-1166. [14] Paganini-Hill, A. (1999) Estrogen replacement therapy and colorectal cancer risk in elderly women. Diseases of the Colon & Rectum, 42(10), 1300-1305. [15] Nanda, K., Bastian, L.A., Hasselblad, V. and Simel, D.L. (1999) Hormone replacement therapy and the risk of co- lorectal cancer: A meta-analysis. Obstetrics & Gynecol- ogy, 93(5), 880-888. [16] Di Leo, A., Messa, C., Cavallini, A. and Linsalata, M. (2001) Estrogens and colorectal cancer. Current Drug Targets - Immune, Endocrine & Metabolic Disorders, 1(1), 1-12. [17] Gambacciani, M., Monteleone, P., Sacco, A. and Genaz- zani, A.R. (2003) Hormone replacement therapy and en- dometrial, ovarian and colorectal cancer. Best Practice & Research Clinical Endocrinology & Metabolism, 17(1), 139-147. [18] Hoffmeister, M., Raum, E., Krtschil, A., Chang-Claude, J. and Brenner, H. (2009) No evidence for variation in co- lorectal cancer risk associated with different types of postmenopausal hormone therapy. Clinical Pharmacol- ogy & Therapeutics, 86(4), 416-424. [19] Grodstein, F., Newcomb, P.A. and Stampfer, M.J. (1999) Postmenopausal hormone therapy and the risk of colo- rectal cancer: A review and meta-analysis. American Journal of Medicine, 106(5), 574-582. [20] Chlebowski, R.T., Wactawski-Wende, J., Ritenbaugh, C., Hubbell, F.A., Ascensao, J., Rodabough, R.J., Rosenberg, C.A., Taylor, V.M., Harris, R., Chen, C., Adams-Campbell, L.L. and White, E. (2004) Estrogen plus progestin and colorectal cancer in postmenopausal women. The New England Journal of Medicine, 350(10), 991-1004. [21] Nelson, H.D., Humphrey, L.L., Nygren, P., Teutsch, S.M. and Allan, J.D. (2002) Postmenopausal hormone re- placement therapy: Scientific review. JAMA, 288(7), 872-881. [22] Canfell, K., Banks, E., Moa, A.M. and Beral, V. (2008) Decrease in breast cancer incidence following a rapid fall in use of hormone replacement therapy in Australia. Medical Journal of Australia, 188(11), 641-644. [23] Lindblom, A. (2001) Different mechanisms in the tu- morigenesis of proximal and distal colon cancers. Cur- rent Opinion in Oncology, 13(1), 63-69. [24] Cheng, X., Chen, V.W., Steele, B., Ruiz, B., Fulton, J., Liu, L., Carozza, S.E. and Greenlee, R. (2001) Sub- site-specific incidence rate and stage of disease in colo- rectal cancer by race, gender, and age group in the United States, 1992-1997. Cancer, 92(10), 2547-2554. [25] Iacopetta, B. (2002) Are there two sides to colorectal cancer? International Journal of Cancer, 101(5), 403- 408. [26] Giovannucci, E., Pollak, M., Liu, Y., Platz, E.A., Majeed, N., Rimm, E.B. and Willett, W.C. (2003) Nutritional pre- dictors of insulin-like growth factor I and their relation- ships to cancer in men. Cancer Epidemiology, Bio- markers & Prevention, 12(2), 84-89. [27] Matanoski, G., Tao, X.G., Almon, L., Adade, A.A. and Davies-Cole, J.O. (2006) Demographics and tumor char- acteristics of colorectal cancers in the United States, 1998-2001. Cancer, 107(5), 1112-1120. [28] Azzoni, C., Bottarelli, L., Campanini, N., Di Cola, G., Bader, G., Mazzeo, A., Salvemini, C., Morari, S., Di Mauro, D., Donadei, E., Roncoroni, L., Bordi, C., and Sarli, L. (2007) Distinct molecular patterns based on proximal and distal sporadic colorectal cancer: Arguments for dif- ferent mechanisms in the tumorigenesis. International Journal of Colorectal Disease, 22(2), 115-126. [29] Leopoldo, S., Lorena, B., Cinzia, A., Gabriella, D.C., Angela Luciana, B., Renato, C., Antonio, M., Carlo, S., Cristina, P., Stefano, C., Maurizio, T., Luigi, R., and Ce- sare, B. (2008) Two subtypes of mucinous adenocarci- noma of the colorectum: clinicopathological and genetic features. Annals Of Surgical Oncology, 15(5), 1429- 1439. [30] Cho, E., Smith-Warner, S.A., Ritz, J., van den Brandt, P.A., Colditz, G.A., Folsom, A.R., Freudenheim, J.L., Giovannucci, E., Goldbohm, R.A., Graham, S., Holm- berg, L., Kim, D.H., Malila, N., Miller, A.B., Pietinen, P., Rohan, T.E., Sellers, T.A., Speizer, F.E., Willett, W.C., Wolk, A., and Hunter, D.J. (2004) Alcohol intake and colorectal cancer: a pooled analysis of 8 cohort studies. Annals of Internal Medicine, 140(8), 603-613. [31] Moskal, A., Norat, T., Ferrari, P. and Riboli, E. (2007) Alcohol intake and colorectal cancer risk: A dose- response meta-analysis of published cohort studies. In- ternational Journal of Cancer, 120(3), 664-671. [32] Shrubsole, M.J., Wu, H., Ness, R.M., Shyr, Y., Smalley, W.E. and Zheng, W. (2008) Alcohol drinking, cigarette smoking, and risk of colorectal adenomatous and hyper- plastic polyps. American Journal of Epidemiology, 167(9), 1050-1058. [33] Smalley, W., Ray, W.A., Daugherty, J. and Griffin, M.R. (1999) Use of nonsteroidal anti-inflammatory drugs and incidence of colorectal cancer: A population-based study. Archives of Internal Medicine, 159(2), 161-166. [34] Rostom, A., Dube, C., Lewin, G., Tsertsvadze, A., Bar- rowman, N., Code, C., Sampson, M. and Moher, D. (2007) Nonsteroidal anti-inflammatory drugs and cyclo- oxygenase-2 inhibitors for primary prevention of colo- rectal cancer: A systematic review prepared for the U.S. Preventive Services Task Force. Annals of Internal Medicine, 146(5), 376-389. [35] Dube, C., Rostom, A., Lewin, G., Tsertsvadze, A., Bar- rowman, N., Code, C., Sampson, M. and Moher, D. (2007) The use of aspirin for primary prevention of co- lorectal cancer: a systematic review prepared for the U.S. Preventive Services Task Force. Annals of Internal  M. Fisher et al. / HEALTH 2 (2010) 842-849 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 849 849 Medicine, 146(5), 365-375. [36] Hebert-Croteau, N. (1998) A meta-analysis of hormone replacement therapy and colon cancer in women. Cancer Epidemiology, Biomarkers & Prevention, 7(8), 653-659. [37] Prihartono, N., Palmer, J.R., Louik, C., Shapiro, S. and Rosenberg, L. (2000) A case-control study of use of postmenopausal female hormone supplements in relation to the risk of large bowel cancer. Cancer Epidemiology, Biomarkers & Prevention, 9(4), 443-447. [38] Nichols, H.B., Trentham-Dietz, A., Hampton, J.M. and Newcomb, P.A. (2005) Oral contraceptive use, reproduc- tive factors, and colorectal cancer risk: Findings from Wisconsin. Cancer Epidemiology, Biomarkers & Preven- tion, 14(5), 1212-1218. [39] Murff, H.J., Shrubsole, M.J., Smalley, W.E., Wu, H., Shyr, Y., Ness, R.M. and Zheng, W. (2007) The interac- tion of age and hormone replacement therapy on colon adenoma risk. Cancer Detection and Prevention, 31(2), 161-165. [40] Kennelly, R., Kavanagh, D.O., Hogan, A.M. and Winter, D.C. (2008) Oestrogen and the colon: Potential mecha- nisms for cancer prevention. Lancet Oncology, 9(4), 385- 391. [41] Rizk, D.E., Helal, T.E., Mason, N. and Berg, B. (1998) Non-evidence of estrogen receptors in the rectal mucosa. International Urogynecology Journal and Pelvic Floor Dysfunction, 9(3), 136-139. [42] Konstantinopoulos, P.A., Kominea, A., Vandoros, G., Sykiotis, G.P., Andricopoulos, P., Varakis, I., Sotiropou- lou-Bonikou, G. and Papavassiliou, A.G. (2003) Oestro- gen receptor beta (ERbeta) is abundantly expressed in normal colonic mucosa, but declines in colon adenocar- cinoma paralleling the tumour's dedifferentiation. Euro- pean Journal of Cancer, 39(9), 1251-1258. [43] Heiss, G., Wallace, R., Anderson, G.L., Aragaki, A., Bere- sford, S.A., Brzyski, R., Chlebowski, R.T., Gass, M., LaCroix, A., Manson, J.E., Prentice, R.L., Rossouw, J. and Stefanick, M.L. (2008) Health risks and benefits 3 years after stopping randomized treatment with estrogen and progestin. JAMA, 299(9), 1036-1045. [44] Chan, J.A., Meyerhardt, J.A., Chan, A.T., Giovannucci, E. L., Colditz, G.A. and Fuchs, C.S. (2006) Hormone re- placement therapy and survival after colorectal cancer diagnosis. Journal of Clinical Oncology, 24(36), 5680- 5686. [45] Clarke, C.A. and Glaser, S.L. (2007) Declines in breast cancer after the WHI: Apparent impact of hormone ther- apy. Cancer Causes Control, 18(8), 847-852. [46] Ravdin, P.M., Cronin, K.A., Howlader, N., Berg, C.D., Chlebowski, R.T., Feuer, E.J., Edwards, B.K. and Berry, D.A. (2007) The decrease in breast-cancer incidence in 2003 in the United States. The New England Journal of Medicine, 356(16), 1670-1674. [47] Wada-Hiraike, O., Warner, M. and Gustafsson, J.A. (2006) New developments in oestrogen signalling in colonic epithelium. Biochemical Society Transactions, 34(6), 1114-1116. [48] Foley, E.F., Jazaeri, A.A., Shupnik, M.A., Jazaeri, O. and Rice, L.W. (2000) Selective loss of estrogen receptor beta in malignant human colon. Cancer Research, 60(2), 245- 248. [49] Jassam, N., Bell, S.M., Speirs, V. and Quirke, P. (2005) Loss of expression of oestrogen receptor beta in colon cancer and its association with Dukes' staging. Oncology Reports, 14(1), 17-21. [50] Di Leo, A., Barone, M., Maiorano, E., Tanzi, S., Piscitelli, D., Marangi, S., Lofano, K., Ierardi, E., Principi, M. and Francavilla, A. (2008) ER-beta expression in large bowel adenomas: implications in colon carcinogenesis. Diges- tive and Liver Disease, 40(4), 260-266. [51] Issa, J.P., Ottaviano, Y.L., Celano, P., Hamilton, S.R., Davidson, N.E. and Baylin, S.B. (1994) Methylation of the oestrogen receptor CpG island links ageing and neo- plasia in human colon. Nature Genetics, 7(4), 536-540. [52] McMichael, A.J. and Potter, J.D. (1980) Reproduction, endogenous and exogenous sex hormones, and colon cancer: A review and hypothesis. Journal of the National Cancer Institute, 65(6), 1201-1207. [53] Alberts, D. S., Martinez, M.E., Hess, L.M., Einspahr, J.G., Green, S. B., Bhattacharyya, A. K., Guillen, J., Krutzsch, M., Batta, A. K., Salen, G., Fales, L., Koonce, K., Parish, D., Clouser, M., Roe, D., and Lance, P. (2005) Phase III trial of ursodeoxycholic acid to prevent colorectal ade- noma recurrence. Journal of the National Cancer Insti- tute, 97(11), 846-853. [54] Saydah, S.H., Platz, E.A., Rifai, N., Pollak, M.N., Bran- cati, F.L. and Helzlsouer, K.J. (2003) Association of markers of insulin and glucose control with subsequent colorectal cancer risk. Cancer Epidemiology, Biomarkers & Prevention, 12(5), 412-418. [55] Adlercreutz, H. (2002) Phyto-oestrogens and cancer. Lan- cet Oncology, 3(6), 364-373. [56] Hogan, A.M., Collins, D., Sheehan, K., Zierau, O., Baird, A.W. and Winter, D.C. (2010) Rapid effects of phytoes- trogens on human colonic smooth muscle are mediated by oestrogen receptor beta. Molecular and Cellular En- docrinology, 320(1-2), 106-110. [57] Hedelin, M., Lof, M., Olsson, M., Adlercreutz, H., Sandin, S. and Weiderpass, E. (2008) Dietary phytoestrogens are not associated with risk of overall breast cancer but diets rich in coumestrol are inversely associated with risk of estrogen receptor and progesterone receptor negative breast tumors in Swedish women. Journal of Nutrition, 138(5), 938-945. [58] Rossouw, J.E., Prentice, R.L., Manson, J.E., Wu, L., Barad, D., Barnabei, V.M., Ko, M., LaCroix, A.Z., Mar- golis, K.L. and Stefanick, M.L. (2007) Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA, 297(13), 1465- 1477. [59] Stefanick, M.L., Anderson, G.L., Margolis, K.L., Hendrix, S.L., Rodabough, R.J., Paskett, E.D., Lane, D.S., Hubbell, F.A., Assaf, A.R., Sarto, G.E., Schenken, R.S., Yasmeen, S., Lessin, L. and Chlebowski, R.T. (2006) Effects of conjugated equine estrogens on breast cancer and mam- mography screening in postmenopausal women with hysterectomy. JAMA, 295(14), 1647-1657. |