Prostate Cancer Disease Characteristics at the Time of Diagnosis and Initial Treatment Offered in a Tertiary Hospital at Ouagadougou (Burkina Faso) ()
1. Introduction
Prostate cancer (PCa) is the second most common cause of cancer and the sixth leading cause of cancer death among men worldwide with an estimated 899,000 new cases and 258,000 new deaths in 2008 [1]. The International Agency for Research on Cancer (IARC) estimates that PCa is a growing problem in Africa: approximately 57.048 African men will die of PCa in the next two decades [1,2]. Despite this dramatically increase of the disease impact, PCa cases remain under diagnosed and underreported in Sub-Saharan Africa (SSA). Very few data are available for PCa incidence, prevalence, aggressiveness, and mortality in men of Sub-Saharan African countries [1-3]. In Burkina Faso the true burden of PCa is not well evaluated. Previous studies in Burkina Faso are suggestive that PCa knowledge and awareness are pour in the general population [4] and that most cases are diagnosed late [5]. The aim of the present study is to provide more data concerning characteristics of newly diagnosed PCa and an overview of initial treatments offered in the most important urological center of Burkina Faso.
2. Patients and Methods
We performed a prospective and descriptive non-randomized patient’s cohort study. Newly diagnosed PCa cases were included between January 2009 and December 2012 at the urology division of the Yalgado Ouedraogo University Teaching Hospital of Ouagadougou. 168 consecutives cases were enrolled during the study period and their details entered into a database. This study did not need an ethical committee advice in Burkina Faso because it was a medical record chart abstraction study using anonymized data. All the patients had given their verbal informed consent before inclusion in the study. PCa diagnosis was done at histological analysis of transrectal prostate biopsy (TRPB) for all the patients. The variables of interest included age at diagnosis, the clinical symptoms at the time of diagnosis, serum Prostate Specific Antigen (PSA) level, the pathological variables (the histological type and the Gleason score), the stage of tumor and the initial therapeutic options. The existence of metastatic PCa was evaluated through clinical exam and thoraco-abdominal and pelvis computed tomography. Tumor stage was determined according to the 2009 TNM classification.
Descriptive statistics were used to summarize these variables in terms of frequencies, means and standard deviation. A low standard deviation (SD) indicates that the data points are close to the mean (the expected value). When the standard deviation is high, it indicates that the data points are spread out over a large range of values.
We also presented a scatter showing how the number of PCa has evolved over time, precisely from 2009 to 2012. A linear trend is estimated on this graph, showing the relationship between the time (X) and the number of PCa (Y). For this estimation, the R-Squared (R2) is calculated, showing how close the data are to the fitted regression line. The closer it is to 1, the better the fit.
3. Results
3.1. Clinical Findings
At the time of diagnosis, the age of patients ranges from 30 to 95 years, with an average of 68, 59 years and a SD of 9.41 . The majority of the patients (76.2%) were in the 60 - 69 years and 70 - 79 years age brackets (Figure 1). 19 new cases of PCa were recorded in 2009 and the number of diagnosed cases had risen to 68 in 2012 the R2 value was 0.98033 very closer to 1 This represents a 3.6- fold increase in the incidence of PCa in our institution during the four years of the study period (Figure 2). Most patients were symptomatic at the time of diagnosis (95.8%, n = 161). Only 7 patients (4.2%) were asymptomatic. Urinary retention was the first clinical patterns of reference in our center (n = 63, 37.5%). Table 1 lists the

Figure 2. Evolution of the number of PCa diagnosed per year.
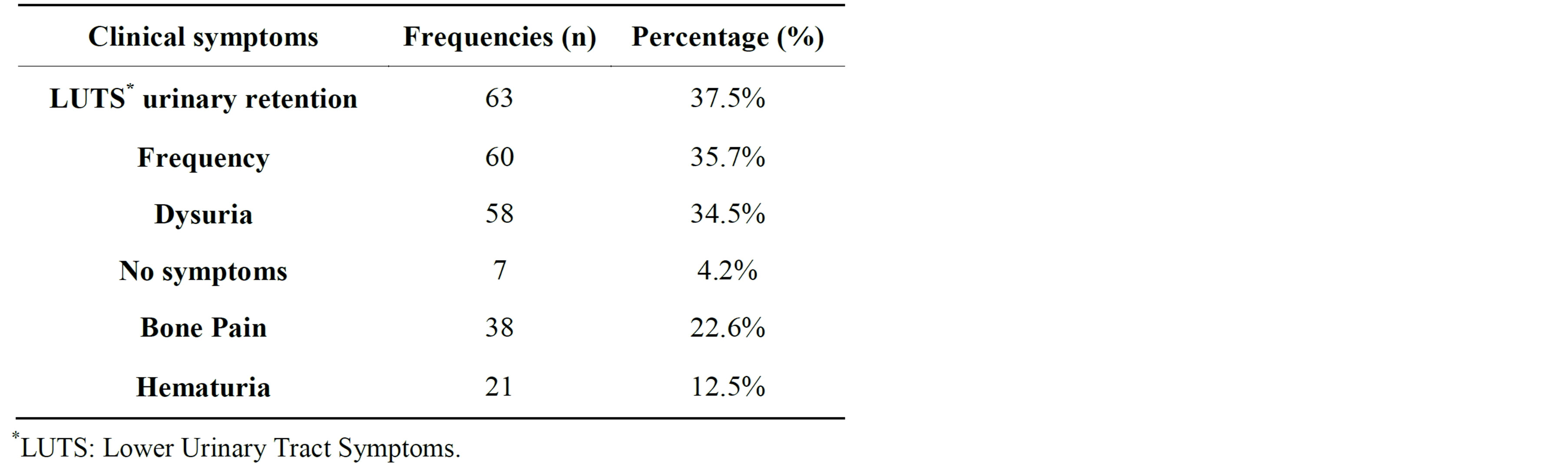
Table 1. Presenting symptoms at diagnosis.
presenting symptoms at the time of diagnosis. The mean duration of symptoms prior to presentation was 11.6 ± 10.9 months with a range of 1 week to 6 years.
The diagnosis of PCa was suspected based on increased PSA without symptoms in only 7 patients (4.2%) and the majority of patients (55.3%, n = 93) on abnormal digital rectal examination (DRE) [Table 2]. Overall mean serum PSA value was 483.3 with a standard deviation of 145.4 ng/ml. The values range from 1 to 7421 and 63 patients (37.5%) had a serum PSA level over than 100 ng/ml (Figure 3).
3.2. PCa Diagnosis and Staging
All the patients had adenocarcinoma on histological
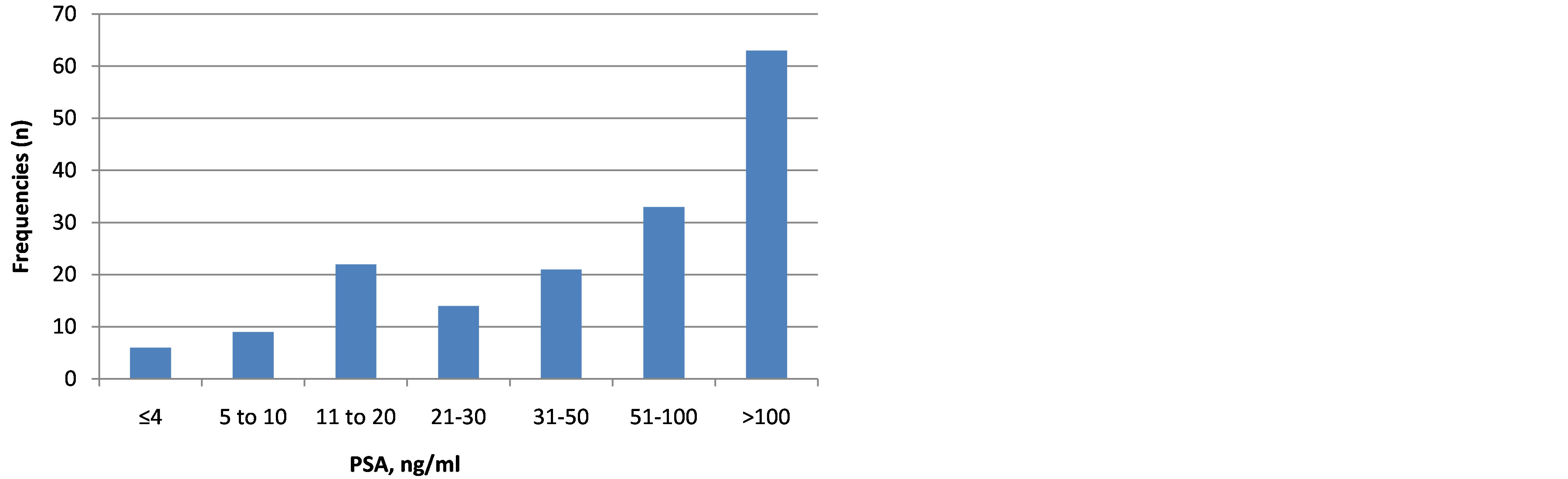
Figure 3. Repartition of patients according to serum PSA level.

Table 2. Indication of prostate biopsy.
analysis of TRPB cores (Figure 4). Most of the patients (60.1%, n = 101) had Gleason score 6 and 67 (39.9%) had Gleason score 7 or higher (Figure 5). Most patients (86.9%, n = 146) had their primary tumor extended over the prostatic capsule (T3-T4 stages) and 13.1% (n = 22) had a localized disease. Table 3 summarized the tumor staging according to the 2009 TNM classification.
3.3. Initial Treatment Offered
Androgen deprivation therapy (ADT) was the first therapeutic option for 121 patients (72%). A total of 73 patients (43.4%) underwent ADT through bilateral orchiectomy that was done as monotherapy and in association with antiandrogen in 16 patients (9.5%). 32 patients (19%) received a medical ADT that consisted of Antiandrogen (ciproterone acetate) 200 - 300 mg daily in 18 patients (10.7%) and luteinizing hormone-releasing hormone (LHRH) analogue (3.75 mg monthly) in 14 (8.3%). 14 patients (8.3%) refused the treatment and discharged against medical advice. Only 3 patients (1.78%) underwent radical prostatectomy. No patient had a radiation therapy because this technic was not available in Burkina Faso. The Figure 6 resumes the initials therapeutic options offered.
4. Discussion
Incidence of PCa varies widely between ethnic populations and countries [1]. The highest rates of this disease are in North America especially in African Americans (228.5 per 100,000 men) and Caribbean men of African descent [1,6]. The reported incidence rates in SSA are
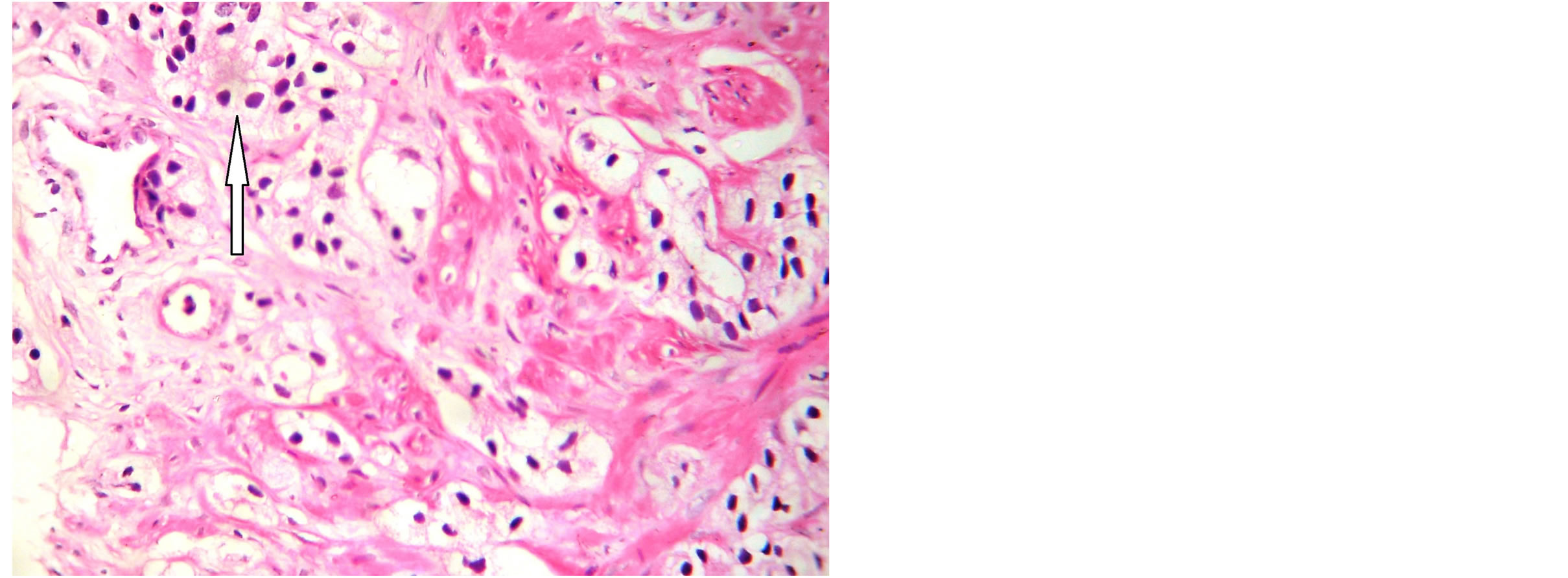
Figure 4. Microphotography ×100: Prostatic adenocarcinoma. Variation of cells sizes, enlarged and hyperchromatic nuclei (arrow). Gleason grade 3.
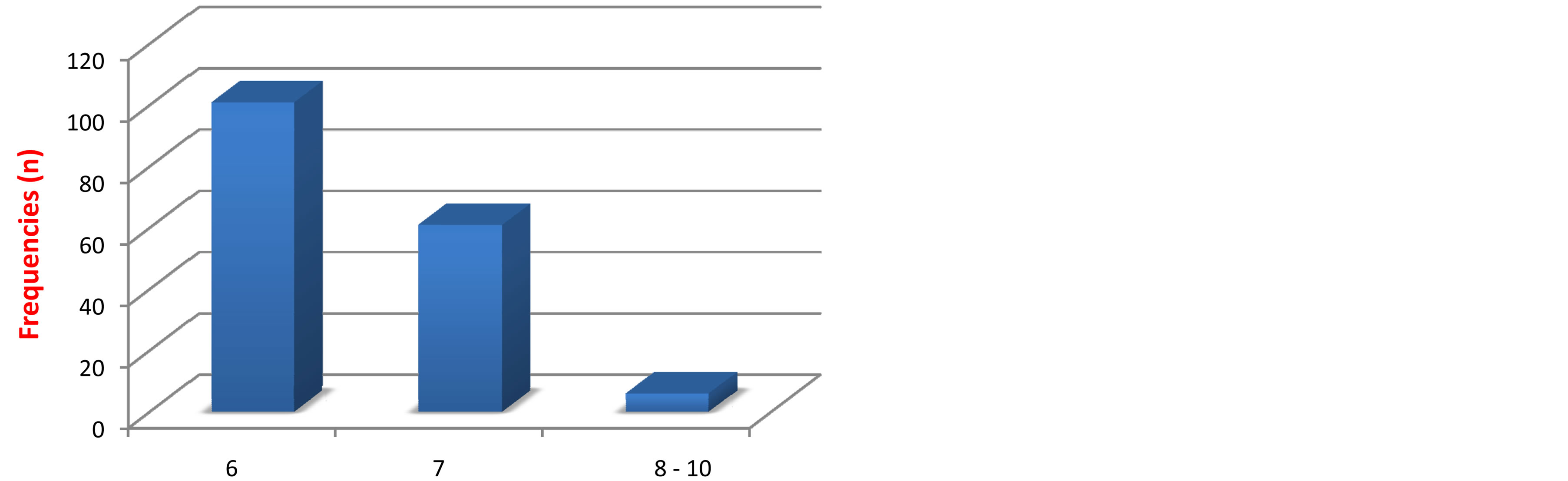
Figure 5. Repartition of patients according to Gleason score.
much lower than those among African Americans. Incidence varied substantially by regions in Africa with rates highest in the East (10.7 - 38.1/100,000 men-years), intermediate in the South (14.3 - 21.8), and lowest in the West (4.7 - 19.8) [3]. The access to quality health care services, availability of pathology services and the availability of cancer registries affect how rates of PCa are reported and can explain the differences between
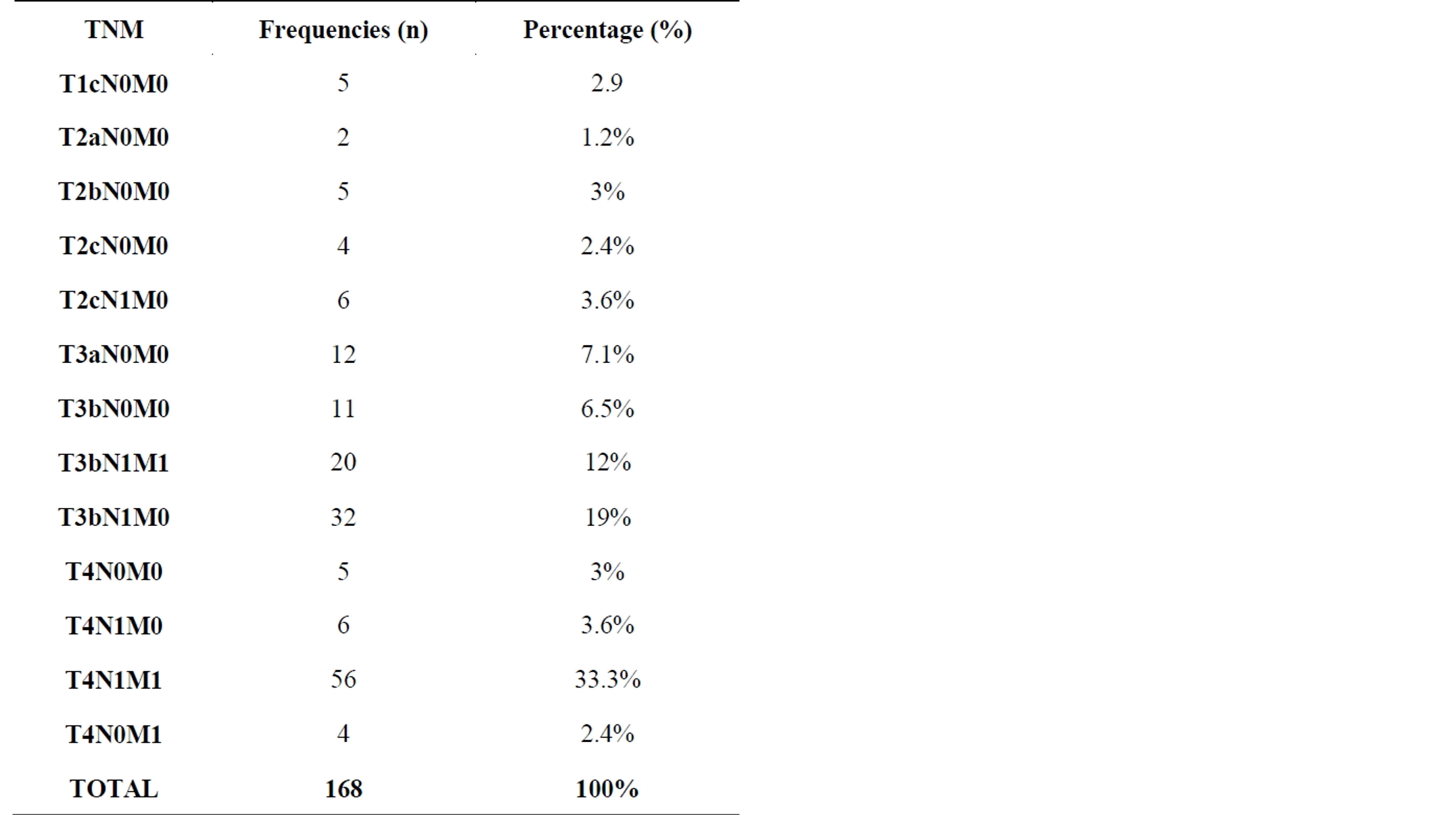
Table 3. Clinical stages according to TNM classification.
African Americans and their ancestry from SSA but also between Sub-Saharan African countries. According to those reasons we can postulate that the true PCa incidence in African men is probably higher than what is reported. This is strengthening by the global increased number of PCa cases in Africa through the last 2 decades [1,3,7,8]. Our study corroborates this trend with the increasing number of cases through the four years of the study (19 in 2009 to 68 in 2012).
In this study the mean age at diagnosis was 68.59 ± 9.41 and patients aged 60 - 69 years and 70 - 79 years had the highest rate of PCa. The age range at the time of diagnosis of PCa in our study is also commonly reported from West Africa where studies from Ghana [9], Nigeria [10] and Senegal [11] recorded a mean age of 65.4, 66.6 and 65 years respectively. The age of diagnosis of PCa in our study is also similar to those reported from the developed world particularly in Europe and North America [12,13]. However, the majority of PCa cases are diagnosed in patients who are asymptomatic in the developed world due to the widespread use of the Prostate Specific Antigen (PSA) blood test [12-14]. 68.7% of PCa cases were diagnosed in the absence of symptoms in the study of Muller [12] from the USA. Contrariwise the majority of patients in our study are symptomatic (95.8%) and presented with LUTS and features of locally advanced or metastatic disease. Numerous studies have found that black men have a higher stage of disease at presentation and are more likely to die of their prostate cancer than their white counterparts [15-17]. Powell [17] evidenced that African Americans have similar pathogenic mechanisms and age at PCa initiation to Caucasians but they have a faster growth rate and/or an earlier transformation to clinically significant PCa. Late presentation of PCa is commonly reported from SSA [5,18-20]. The reason for the late presentation in our environment may be explained by poor awareness of PCa, poverty, inadequate diagnostic facilities and the lack of access to healthcare [2,10,11,19].
Another salient finding in the present study is the high level of serum PSA (483.3 ± 145.4 ng/ml) at the time of diagnosis of PCa. Several studies have observed a higher age-specific serum PSA values in black men without prostate cancer compared to white men [21-23]. Despite those suggestive data, the race-specific PSA is controversial and more detailed studies are needed to elucidate if this is a result of genetic predisposition or timing in the diagnosis of PCa [21-23]. In another hand, reported prostate cancer cases from Africa shared a common elevated PSA level [10,19,24]. Niang [11] in Senegal and Heyns [24] in South Africa reported a mean PSA value of 1447.5 ng/mL and 766.1 ng/mL respectively. Except the possible race-specific PSA this could be relevant to late presentation of PCa and the absence of appropriate approaches to screening in Africa.
In a recent review on PCa incidence, aggressiveness, and mortality in men of African descent Reebeck et al. [2] found that the tumor stage distribution differed substantially by geography, with a larger proportion of stage T3/T4 tumors in Africa than other locations. Our study where stage T3/T4 was predominant (86.9%) is coherent with the findings of this review. Advanced and highgrade PCa among black men from the USA, Caribbean and other sub-Saharan African countries suggests an element of shared genetics disadvantage of high-risk disease but may also be due to differences in screening and availability of diagnosis resources(PSA, pathologists, urologists) [2,15,25].
Bilateral orchiectomy is a common and widely used surgical procedure for advanced and metastatic PCa in Burkina Faso and generally in the developing world. At the opposite, the use of surgical ADT is declining in developed countries due to the availability of medical ADT which are considered to be equally effective in reducing testosterone levels as orchiectomy with less psychological effect [26,27]. Surgical orchidectomy is a less expensive treatment comparatively with medical ADT. This is the mains reason that justifies the widespread use of bilateral orchidectomy in SSA [11,19,23]. Moreover many patients in our environment are reluctant to receive medication (8.3% of patients in our study refused the treatment) and lost to follow-up after hospitalization. Therefore, bilateral orchiectomy is a single and safe method to ensure that treatment is maintained.
Radical prostatectomy remains the gold standard for treatment of organ confined prostate cancer [28,29]. Only 3 radical prostatectomies (1.8% of patients) were done in our study. It has been noted that access of patients with localized PCa to radical prostatectomy in SSA is low mainly due to lack of expertise in the procedure of open radical prostatectomy and advanced disease at diagnosis [11,23,27]. However curative management of prostate cancer through radical prostatectomy and radiotherapy depends on early detection of the disease. The development of a well-planned national screening program can be a way to increase early diagnosis and improve PCa outcomes in Burkina Faso and other countries in SSA.
The mains limitations of this study are: 1) data reported here are limited to one medical center and are not representative of all the population of Burkina Faso; 2) PSA testing and prostate biopsy are not readily available and many PCa are probably excluded in this study. Despite those limitations this study have the merit to complete data from Burkina Faso and provide an overview of newly diagnosed PCa characteristics and treatment in the most important referral center for patients with urological diseases from all over the country. Further multicentric studies are needed to better access the PCa epidemiology disease characteristics and treatment outcomes in Burkina Faso.
5. Conclusion
An increase in the diagnosis of PCa in our country was observed in this study. The diagnosis of prostate cancer was usually tardive in Burkina Faso. Treatment often involves surgical ADT for socioeconomic reasons. Prostatectomy was only very seldom indicated. Screening for PCa could help detect earlier stage PCa and improve the treatment outcome in Burkina Faso.
Abbreviations
PCa: Prostate Cancer SSA: Sub-Saharan Africa TRPB: Transrectal Prostate Biopsy DRE: Digital Rectal Examination PSA: ProstateSpecific Antigen ADT: Androgen Deprivation Therapy LUTS: Lower Urinary Tract Symptoms
NOTES