Oral and peri-oral signs and symptoms of herbal dentifrices in patients in two oral medicine clinics in Lagos—A preliminary study ()
1. INTRODUCTION
The use of herbal remedies have assumed a global dimension culminating in its being used in the treatment of various ailments in both developed as well as developing countries. This alternative form of therapy appears to be the latest fad, as a number of herbal products are readily available to consumers. Teas, soaps, facial products, colon cleansers, as well as mouth washes and dentifrices are a few of these products.
It is reported that herbal medicines are the mainstay of health care for a large proportion of the population in underdeveloped countries due to a combination of nonavailability of modern medical care, ignorance and poverty [1,2]. Over three-quarters of the population in subSaharan Africa reportedly depend on traditional medicine for primary health care, [3-5]. More than 60% of the Chinese use herbal therapy [6] and a significant part of the rural population in the Indian subcontinent rely on indigenous medical systems that use herbs, ash and heavy metals [7].
The use of herbal medicine has also reportedly increased in developed countries [8]. An estimated onethird to one-half of all Americans practice some form of alternative medicine including use of natural or herbal health care products [9-12] Several authors opined that the use of these products, including dentifrices, has increased significantly in the last decade [13-16].
A number of articles have been written on the efficacy or otherwise of herbal dentifrices. Some reports indicate that the lack of a consensus among dental professionals on the subject matter has made it difficult for dentists to provide information on the product safety and efficacy [17].
Dentists in particular have been advised on the need to be cautious and well informed on the inherent dangers associated with herbal ingredients in dentifrices that lack specific and defined requirements and regulations [17- 21].
A dearth of scientific studies on natural and herbal products in peer reviewed dental literature has also been cited as posing a conundrum for health care professionals in dealing with these products. In addition, few research efforts have been directed toward addressing the potency or quality of herbal ingredients used in these dental products [17]. Reports have also indicated that since only a limited number of in vivo studies on herbal dentifrices have been published, it has not been determined whether they are superior, equivalent or substandard to conventional dentifrices in reducing plaque [18-20].
Herbal toothpastes are readily available to consumers in the open market in Lagos, Nigeria. Marketers of some of the conventional fluoride toothpaste brands in Nigeria have also included herbal variants in their product range.
It is expected that this study will educate and sensitize individuals, and prompt appropriate agencies and institutions on the need to collaborate in evolving the development of a template for research, standardization and regulation of non-conventional toothpastes.
2. MATERIALS AND METHODS
The study which spanned over 12 months was conducted in two separate oral medicine clinics in Lagos; the Randle General Hospital and the Lagos University Teaching Hospital (LUTH) between April 2010 and April 2011. The study population comprised patients seen in the oral medicine clinics with oral mucosal signs and symptoms following daily use of two identified herbal toothpastes.
The identified toothpastes are referred to as Toothpaste A and Toothpaste B for the purpose of this study. The active ingredients in Toothpaste A as indicated on the product package include rosemary, sage, myrrh, eucalyptus, chamomile and other natural oils.
Sodium fluoride, eucalyptus, peppermint, thyme, and aloe vera leaf extract are the active ingredients on the product package in Toothpaste B.
A comprehensive history of the signs and symptoms was obtained from the patients. History included presenting complaints, duration of symptoms, type of herbal dentifrice and the duration of use of herbal product. Additional information on whether or not the use of the toothpaste was based on recommendation by a dental professional was also obtained.
Intra and extra oral examination of the patients was carried out and findings were documented in patient’s clinical notes. Clinical photographs of oral lesions were taken in consenting patients. Patients were given a 2- week recall appointment after being advised to discontinue the use of herbal dentifrice and replace with a conventional fluoride toothpaste of their choice.
Some patients required additional investigations and further treatment. Data analysis was done using the Epi-info 6 software with consultation of a statistician and presented in table format. Significance in association was inferred with p values ≤ 0.5.
No control group was included in this study owing to the incidental nature of the findings during consultation as well as the preliminary nature of the study.
3. RESULTS
Observation from the study gave varied clinical signs and symptoms following regular use of the two identified herbal toothpastes. Forty-five patients had symptoms following consistent use of herbal toothpaste over a period of time. A total of 45 patients, 9 (20%) males and 36 (80%) females were seen. The male: female ratio was 1:4. The age range of patients was 14 - 78 years, mean age 45.5 ± 14.9 years. Age and sex distribution in the patients is seen in Table 1.
The duration of use of herbal dentifrices ranged from 2 weeks - 84 months (mean 24 ± 11.5 months) (Table 2).
The duration of symptoms ranged from 1 week - 40 weeks (mean of 11.3 ± 9.5) Table 3.
Similar oral signs and symptoms were noted in both herbal dentifrices identified in this study. These include burning mouth and peppery sensation, mucosal erythema, lichenoid reaction, xerostomia, loss of taste sensation, angio-oedema as well as oral and peri-oral pigmentation. Burning mouth/peppery in the study was used to describe a fiery sensation in the oral cavity associated with an inability to tolerate spicy foods. Soreness of the oral mucosa in this study was described as the sensation of the presence of oral ulcers without any visible ulceration.
The most frequently observed finding was peppery/ burning mouth sensation. Table 4 shows signs, symptoms and frequency of occurrence of the mucosal responses in the study population.
All the patients in this study had more than one mucosal reaction to the identified herbal dentifrices.
In many patients, resolution of symptoms was progressive within 2 weeks of withdrawal of the herbal toothpaste and its replacement with a conventional fluoride toothpaste. Most of the patients however required further treatment.
A statistically significant association was found between the use of the identified herbal dentifrices and the following mucosal signs and symptoms, namely burning/ peppery sensation (p value = 0.000 and confidence interval (CI) 6.32, 19.53), loss of taste sensation (p value = 0.021, CI = 4.53, 22.73), soreness (p value = 0.047, CI = 4.55, 32.87), erythema (p value = 0.044, CI = 4.55, 32.87) and lichenoid straie (p value = 0.000, CI = 0.044, 0.33).
No statistically significant association was found between the use of herbal toothpaste and mucosal signs and symptoms of xerostomia (p value = 0.067, CI = undefined), angular cheilitis (p value = 0.397, CI = 0.46, 4.26)
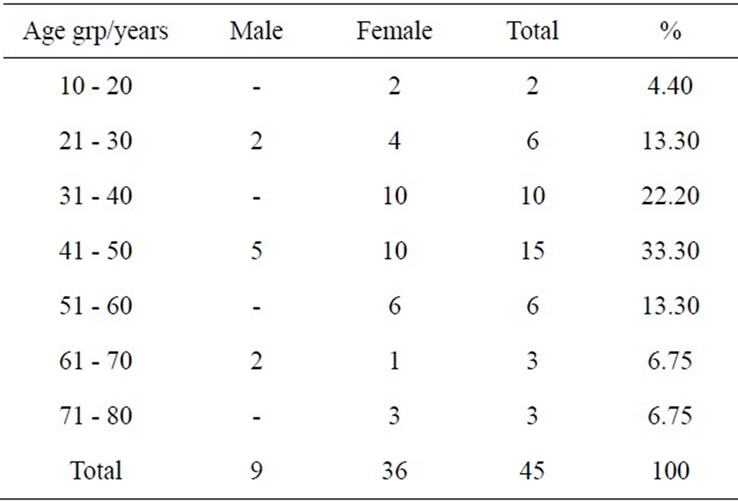
Table 1. Age and gender distribution of patients.
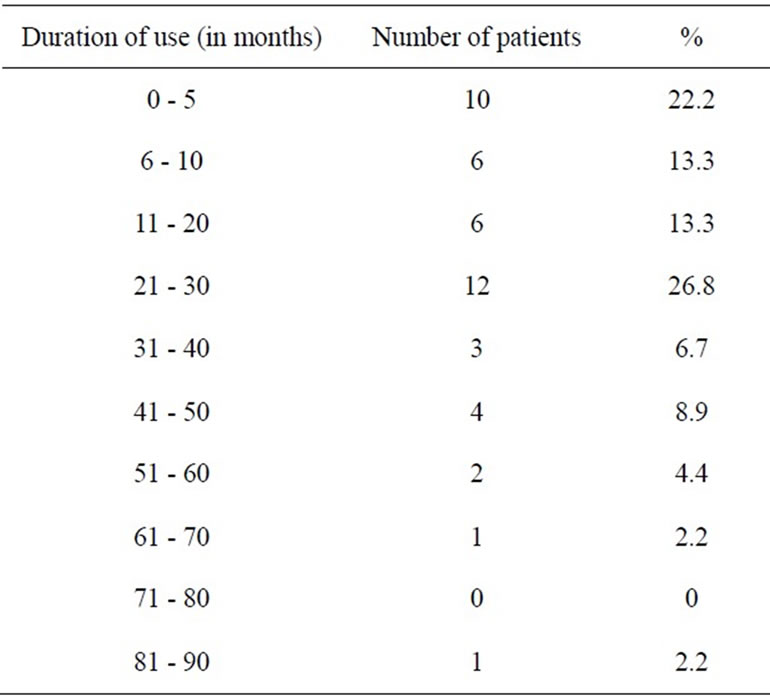
Table 2. Duration of usage of herbal toothpastes A and B.

Table 3. Duration of signs and symptoms prior to consultation.
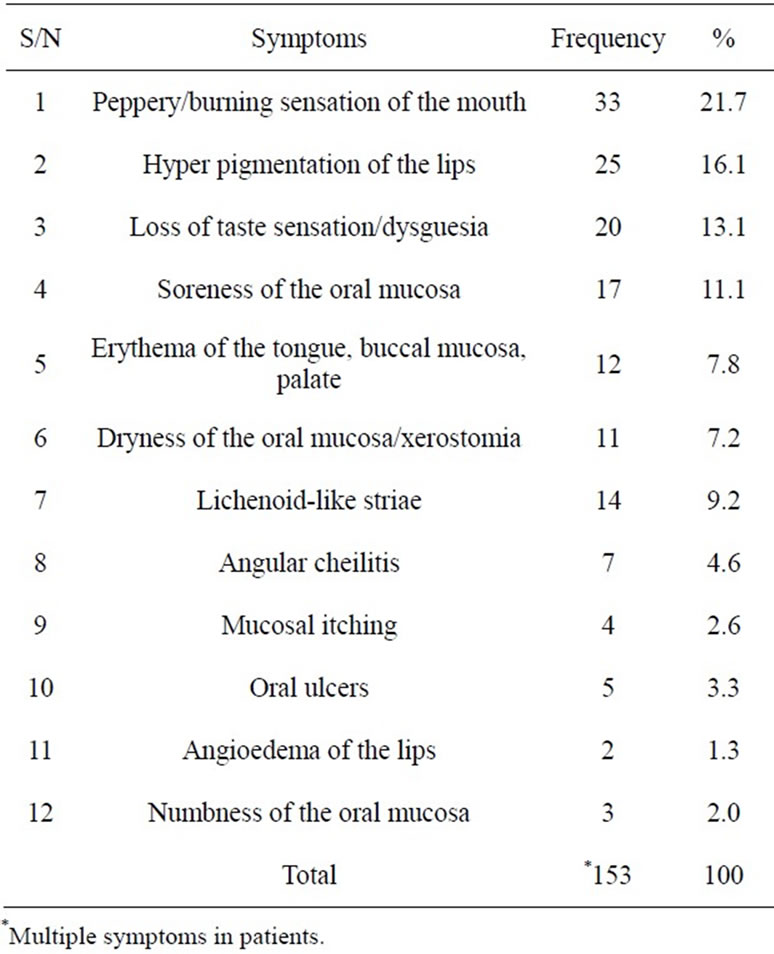
Table 4. Distribution of symptoms observed in study group.
mucosal itching (p value = 0.587, CI = undefined), angiooedema (p value = 0.76, CI = undefined) and numbness (p value = 0.644, CI = undefined).
All respondents indicated that the choice of the particular herbal toothpaste was not based on recommendation by a dentist or other oral health care professional. Figures 1-4 show clinical photographs of lesions seen.
Figure 1 shows circumoral pigmentation;
Figure 2 shows labial and intra-oral pigmentation;
Figure 3 shows erythema of the vermillion border and oral mucosa;
Figure 4 shows gingival erythema.
4. DISCUSSION
Observation from this study suggests that regular use of some herbal dentifrices may result in adverse oral and peri-oral mucosal responses. The study population cuts across all age groups and patients exhibited varying duration of exposure to the implicated herbal dentifrices. There was also variation in duration of symptoms prior to presentation for oral consultation .The varying mucosal responses to the herbal dentifrice and the variation in time frame for such responses may suggest individual reactions to the use of herbal dentifrices. The factors responsible for this variation may need to be identified and considered during clinical trials of non-conventional toothpastes.
The role of the interplay of hormonal factors in female patients may be inconclusive in spite of the female preponderance in this preliminary study. This may need to

Figure 2. Labial and intraoral hyperpigmentation.
be clarified in subsequent studies.
Statistically significant association seen between the use of the herbal dentifrices and mucosal responses of burning mouth/peppery sensation, loss of taste sensation, soreness and erythema suggests that these symptoms may not always be attributed to vitamin deficiencies or anaemias in patients presenting in the oral diagnosis clinic. Lichenoid straie may represent a form of allergic reaction similar to lichenoid drug reaction Further studies may also need to ascertain role of atopy or allergic reactions in responses to use of herbal dentifrice.
No significant association was seen in xerostomia, hyper pigmentation, angular cheilitis, mucosal itching angio-oedema and numbness.
All respondents in this study indicated that their choice of herbal dentifrice was not based on professional recommendation. This may not be unconnected with reports that consumer acceptance of herbal medicines is partly based on the incorrect assumption that “natural” equals safe [22]. The ready availability of herbal dentifrices in the market coupled with the lack of restrictions to their purchase and use may also contribute to the consumers’ procurement without professional consultation. As the popularity of natural medicines and dentifrices continues to rise, dental professionals are said to be in a position to provide information to patients regarding their efficacy and safety. The lack of professional consensus on the subject is said to have made this difficult [23].
Most literature on herbal dentifrices focus on their efficacy over conventional toothpastes rather than on mucosal responses to their use. In a study spanning over six months conducted in 1998 at the College of Dentistry, New York University, Estafan et al. reported that herbal toothpaste and gum therapy were superior to conventional toothpaste in the reduction of plaque and stains [24]. These findings were at variance with a previous study conducted in Northern Ireland 1995 by Mullally et al. who concluded that the herbal based toothpaste was as effective as conventionally formulated dentifrice in the control of plaque and gingivitis. This group of researchers carried out a 6-week study to assess the efficacy of a herbal based toothpaste on the control of plaque and gingivitis [25]. In a related study in India, George and his team also compared the efficacy of a herbal based toothpaste over a conventional brand in the control of plaque and gingivitis. Their conclusion corroborated those of Mullaly et al. that neither had an advantage over the other in the control of plaque and gingivitis [26].
A randomized, double blind controlled trial conducted in the School of Dentistry Ibirapuera, Brazil by Ozaki et al. also reported that there was no significant difference in reduction of gingivitis in those using a herbal dentifrice against those using a non-herbal dentifrice [27].
These studies were largely short term studies conducted mainly to assess the superiority of one over the other with respect to the patient’s periodontal condition. No record was made on the oral mucosal effects in the study group following use of the herbal dentifrice.
In 2007, Anil reported three cases of plasma cell gingivitis which he considered a hypersensitivity reaction following regular use of herbal dentifrices among herbal toothpaste users. He described plasma cell gingivitis (PCG) as a rare benign condition of the gingiva characterized by sharply demarcated erythematous and edematous gingivitis often extending to the mucogingival junction [28]. Gingival lesions observed in this study presented as erythematous areas devoid of edema (Figure 4). All the lesions seen in this study following the use of herbal toothpaste were described clinically, no histopathological diagnosis was carried out.
The role of herbal dentifrices in maintaining optimum oral health is not very clear. Issues that need clarification also include the frequency of use and whether such dentifrices are for daily, prophylactic or therapeutic use. Other unresolved issues include whether the herbal dentifrices are to be used interchangeably or synergistically with the conventional fluoride toothpaste. Areas that could be explored include the incorporation of the herbal dentifrices into prophylactic pastes used for patients with active periodontal conditions.
Claims made by manufacturers and marketers of these products need to be scientifically verified over a sufficient period of time. The residual effects observed in some of the patients following withdrawal of the herbal dentifrices also pose a source of concern.
The role of regulating bodies such as National Association for Food, Drugs and Administrative Control (NAFDAC) and the Nigerian Dental Association (NDA) in approving these products for use is not clearly defined and this needs to be addressed.
5. CONCLUSIONS
The regular use of the herbal dentifrices identified in this study can result in adverse oral signs and symptoms affecting taste, nutrition, aesthetics and general oral physiology in some consumers. These findings would suggest that further long term clinical trials need to be conducted on herbal dentifrices available to consumers to identify the noxious agents causing these adverse reactions. There is a need to standardize and regulate the use of herbal dentifrices.
Dental practitioners should be aware that the oral and peri-oral effects of daily use of some herbal dentifrices could contribute to patient clinic attendance and may lead to increase morbidity in these patients.
NOTES