
1. Introduction
Henri Becquerel’s discovery of radioactivity, and in particular the discovery of the X-rays by Wilhelm Röntgen, sparked a revolution in the modern world. Ionizing radiation is used since then in all areas of life. The scientific research of many scientists and the respective discoveries led to the use of new and modern devices that enable people to improve their life [1] [2].
This ubiquitous use of ionizing radiation brings benefits, but also has a negative impact. Radiation accidents with sources of ionizing radiation [3] [4] [5] greatly increase the natural radiation background [6] [7], which leads to serious negative consequences for a long time. Some of them remain irreversible [8].
Modern medicine would be inconceivable without the use of ionizing radiation, and in particular without x-rays, both for diagnosis and treatment [9] [10] [11] [12]. Improvement and modernization of X-ray equipment is a top priority nowadays [13].
In addition to the benefits, ionizing radiation has a negative side that can be dangerous to the health and lives of those who work with it. This is the main reason to pay special attention to informing and training staff so that they can work safely with ionizing radiation sources. In addition to the training of the future physicians at medical universities [14] [15], special courses are regularly organized for the staff in order to acquire licenses for handling ionizing radiation sources [16] [17] [18].
The widespread use of X-ray equipment in medicine leads to a vital task: the radiation protection of personnel and patients, and the reduction of their dose load obtained from scattered ionizing radiation during a procedure with ionizing radiation. Research in this regard constantly provides new and important information for optimizing the dose load of the staff, when working with the existing X-ray equipment and the new one.
Natasha Ivanova from the Medical University of Varna, Bulgaria is actively working in this field. She published two monographs: a study of the dose load when using a C-arm X-ray system [19] and a study of the dose load when using angiographic X-ray systems [20]. She has also published a series of articles (some of which co-authored with the author of this article) in connection with the dose load of a patient [21] and staff working with C-arm X-ray equipment [22] and angiographic systems [23] [24] [25].
Studies of the doses obtained when working with angiography and C-arm X-ray systems have been carried out by M. Osanai et al.―estimated the impact on eye lens of radiation derived from the 210 Pb in three types of radiation protection glasses [26], Y. Haga et al.―the purpose of this work is to develop a database of 3D scattered radiation dose-rate distributions to estimate the staff dose by location around a C-Arm fluoroscopic system in an interventional procedure room [27], Alnewaini, Z. et al.―in this paper, a novel ray casting approximation of radiation transport is presented and the potential and limitation vs. a full Monte Carlo transport and dose measurements are discussed [28], Sadick V. et al.―they discuss coronary angioplasties can be performed with either single-plane or biplane imaging techniques. The aim of this study was to determine whether biplane imaging, in comparison to single-plane imaging, reduces radiation dose and contrast load and shortens procedural time during 1) primary and elective coronary angioplasty procedures; 2) angioplasty to the main vascular territories; and 3) procedures performed by operators with various levels of experience [29] and Mavrikou I. et al.―they discuss interventional cardiology procedures are usually associated with high patient doses and even deterministic radiation effects may occur. Expensive digital flat panels are preferably used to lower doses, and Athens General Hospital has recently installed one. However, this study shows that it is the cardiologists’ practice that lowers patients’ doses [30].
1.1. Motivation
This study continues the work of our research team dealing with assessment of the dose load from angiographic X-ray equipment. The initial data for the calculations for the article are taken from our dose measurements during angiographic LCx-stenting by using an angiographic system Philips Allura Xper FD10 in the Specialized Hospital for Active Treatment in Cardiology in Varna, Bulgaria.
1.2. Purpose
The purpose of this article is to make calculations of the dose load received by the medical staff during the angiographic procedure LCx stenting (left circumflex coronary artery) for the duration of the two modes of operation and the three projections used as basic. Further, on the basis of these calculations, the dose load of the two modes of operation (radiography and fluoroscopy) of the equipment are to be compared for the three projections (RAO-caudal, LAO-caudal and pure Cranial), used as basic projections, in three different patient table positions (lowest, highest and zero), at three measurement points (“Head”, “Gonads” and “Feet”). Based on this comparison, measures to reduce the dose load of the medical staff during the implementation of an LCx procedure are to be recommended.
2. Methods
The main method in this study is to perform mathematical calculations based on previously measured dose values [19] and to compare the results obtained in order to optimize the dose exposure of the medical staff to the scattered radiation during the angiographic procedure LCx-stenting.
Following projections are used during the angiographic procedure LCx stenting (Table 1):
Total duration of the whole procedure: 45 - 90 minutes
・ The procedure starts with initial 3-4 seconds in the AP projection.
・ The basic projection is used for about 30 to 60 minutes. Each one of the three used projections can be basic depending of the performed procedure. The
![]()
Table 1. Projections used in the procedure LCx stenting.
duration of the procedure in pulse fluoroscopy of the basic projection is about 10 minutes. The duration of radiography in the basic projection is about 2 - 3 minutes.
・ The total duration of the non-basic projections is about 15 to 30 minutes. The total duration of pulse fluoroscopy in the non-basic projections is about 5 minutes. In the non-basic projections no radiography mode is used.
Due to the very low dose load from the PA projection, it is not included in the general calculations, because it will practically not affect the results.
3. Results
Dose calculations for the different projections are shown in Tables 2-4. The results of the tables are illustrated with Diagrams 1-3 for Table 2; Diagrams 4-6 for Table 3; Diagrams 7-9 for Table 4; and 10, 11 and 12 for the whole procedure at the three positions of the table―respectively Diagram 10―lowest, Diagram 11―highest and Diagram 12―zero. For each of the comparative diagrams, the dose was calculated for both modes of operation: radiography and fluoroscopy and for the basic projection the calculations were made for 2 and then for 3 minutes radiography.
Therefore, the graphs show sectors “2 minutes” (summation of fluoroscopy doses for the three projections used and 2 minutes radiography in the main projection) and “3 minutes” (summation of fluoroscopy doses for the three projections used and 3 minutes radiography in the main projection).
In the studied LCx stenting procedure, most of the diagrams show the highest dose load in radiographic mode, both at 2 and at 3 minutes. The dose values obtained in the non-basic projections are very low and therefore the comparison will be made only for the values obtained for work in the basic projections.
When comparing Diagrams 1-3 for the lowest position of the patient table it is seen that the high values prevail at the measured point “gonads”, for the projections LAO-Caudal and Pure Cranial as basic projections; in the projection RAO-Caudal as basic projection high values are observed at the measured point “feet”.
The smallest differences between the values of the different measured points in the radiographic mode, are observed in the projection RAO-Caudal as basic projection, and the largest differences―in the projection Pure Cranial as basic projection. In fluoroscopic mode, the situation is reversed: The smallest differences are in Pure Cranial, and the largest differences―in RAO-Caudal. The lowest values prevail at the measured point “Head” for all basic and non-basic projections in both operating modes.
When comparing Diagrams 4-6 for the highest position of the patient table, lower values than the values in the 2 minutes radiography in relation to the fluoroscopic mode are observed in RAO-Caudal as basic projection. This kind of result is observed only in Diagram 4 (basic projection RAO-Caudal), namely higher dose values for fluoroscopy compared to radiography. In this basic projection a lower value is obtained at the point “Gonads”.
In the other two basic projections LAO-Caudal and Pure Cranial, the observed highest values are for the point “Gonads”, similar to the values obtained at the lowest position of the table. The lowest dose value at this table position is again measured at the point “Head” but there is one exception for RAO-Caudal as basic position, where the value at the point “Head” is higher than the value t the point “Gonads”.
The following three Diagrams 7-9 of the dose load at zero position of the patient table show higher values for all radiographic modes compared to the fluoroscopic ones for all three basic projections. Comparing the radiographic modes, maximum values for the different measurement points are observed for different main projections. When RAO-Caudal is the basic projection, the highest values are measured at “Head”; for LAO-Caudal maximum value is measured at “Feet”, and for the third basic projection Pure Cranial the highest values are at “Gonads”. The lowest values for the radiographic modes are following: for RAO-Caudal at the point “Feet” and for the other two projections―at the point “Head”. Comparing the fluoroscopic modes, the higher values are at the points “Feet”, while for the basic projection Pure Cranial, the values for “Feet” and “Gonads” are equal; for all basic projections the lower values are for the point “Head”.
When comparing Diagrams 10-12 for the doses obtained for the whole procedure in the three different positions of the patient table, the lowest values at the point “Head” for all table positions are clearly indicated. Clearly distinguished maximum values, however, are not observed for any measurement point in all basic projections. For the basic projection RAO-Caudal, the maximum value for all three positions of the patient table is obtained at the point “Steps” and the minimum value―at the point “Head”.
For LAO-Caudal as basic projection, for the lowest and highest position of the patient table, the maximum dose is observed at the point “Gonads”. When the table is in the zero position, the maximum dose value is observed at the point “Steps”. The minimum dose value for all three table positions is obtained at the point “Head”, similar to RAO-Caudal as basic projection.
In the basic projection Pure Cranial for all three table positions the dose maximum value is observed for “Gonads” and the minimum value―for “Head”.
When comparing the number of maximum values for the different projections and the three table positions, the points “Gonads” and “Feet” show a small difference. There is a small advantage to the point “Gonads”.
![]()
Table 2. Dose received during the angiographic procedure LCx stenting by an interventional cardiologist for the lowest position of the patient table, at three points of his body.

Diagram 1. Basic projection RAO caudal―lowest table position.
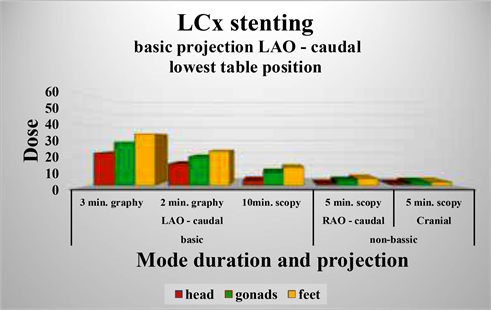
Diagram 2. Basic projection LAO caudal―lowest table position.

Diagram 3. Basic projection Сranial―lowest table position.
![]()
![]()
Table 3. Dose received during the angiographic procedure LCx stenting by an interventional cardiologist for the highest position of the patient table, at three points of his body.
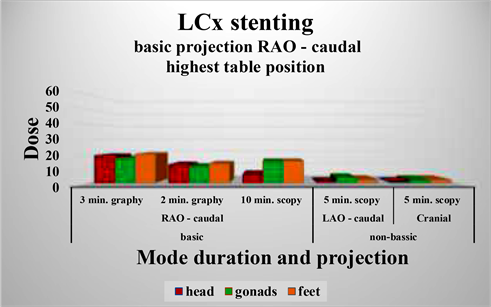
Diagram 4. Basic projection RAO-caudal―highest table position.
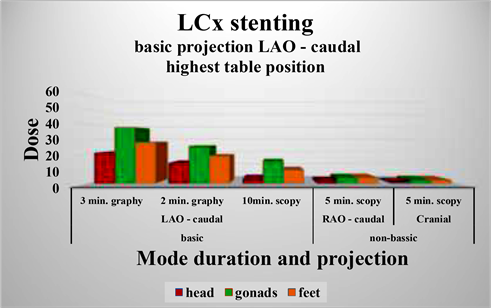
Diagram 5. Basic projection LAO caudal―highest table position.
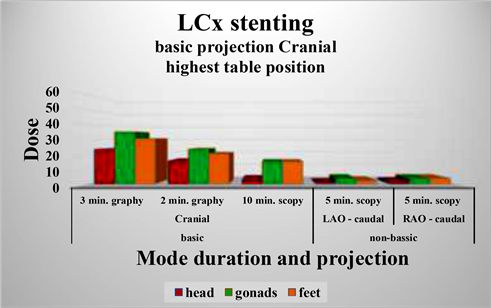
Diagram 6. Basic projection Cranial―highest table position.
![]()
Table 4. Dose received during the angiographic procedure LCx stenting by an interventional cardiologist for the zero position of the patient table, at three points of his body.

Diagram 7. Basic projection RAO-caudal―zero table position.

Diagram 8. Basic projection LAO-caudal―zero table position.

Diagram 9. Basic projection Cranial―zero table position.
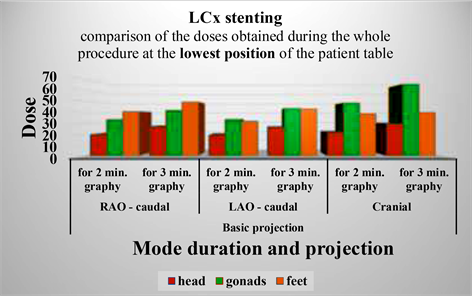
Diagram 10. Comparison of the doses obtained during the whole procedure for different basic projections at the lowest position of the patient table.

Diagram 11. Comparison of the doses obtained during the whole procedure for different basic projections at the highest position of the patient table.
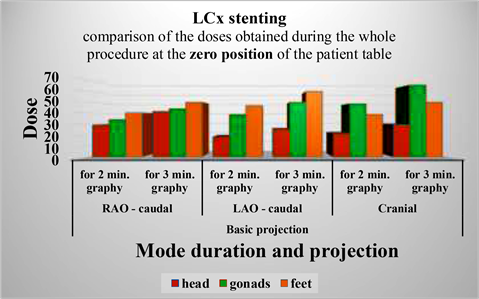
Diagram 12. Comparison of the doses obtained during the whole procedure for different basic projections at the zero position of the patient table.
Comparing the dose values obtained for the three positions of the patient table, the highest values are observed for the zero position of the table, while the values for the other two positions are comparable.
Comparison of the doses obtained by the principal interventional cardiologist, at three points of his body, for the whole LCx stenting procedure for the different basic projections and for different positions of the patient table.
4. Conclusions
The results of the study show that the dose load in the LCx stenting procedure is mainly accumulated due to the use of the radiographic mode of operation of the X-ray equipment.
This high value, which is observed in almost all positions of the patient table and in all the basic projections, is observed, although the time of the X-ray irradiation in the radiographic mode lasts 2 - 3 minutes while the duration of the fluoroscopy is 10 minutes in the basic projection and 5 minutes for the non-basic projections, i.e. total 15 minutes. When comparing these durations, it is found that the operating time in fluoroscopic mode is 5 - 6 times longer than in radiographic mode. Therefore the angiographic equipment, which is C-arm type equipment, creates a larger dose load in radiography than in fluoroscopy. In this sense, in order to reduce the dose load of the medical staff performing the procedure, it is necessary to reduce the duration of work in radiographic mode as much as possible. The desired reduction in the duration of the radiographic mode can be achieved through continuous and effective preparation training without use of X-rays. The results show that the maximum dose load is obtained at zero position of the patient table in this procedure. To reduce the dose load, it is useful to avoid working in this position when performing the LCx stenting.
When working in the projection RAO-caudal as basic projection, in all three positions of the patient table, the most irradiated point is “Feet”. The limbs are the least sensitive parts of the human body and therefore no additional protection is required for them.
The highest dose values at the measured point “Gonads” are observed when working in the projections LAO-Caudal and Pure Cranial. The gonads are very radiation sensitive organs in the human body. Therefore, to reduce the dose load at this point, the body of the person performing the procedure must be protected with radiation protection clothing―a lead rubber apron with a lead equivalent of not less than 0.5 mm. Radiation protection clothing is also recommended when working in RAO-caudal projection. Although the highest dose load for this projection is obtained for the feet, the next higher dose value is obtained for the point “Gonads”.
The values of the dose load for the point “Head” are not very high but due to the large number of performed procedures would lead to increased dose load of the head. Therefore, it is advisable to use radiation protection for the head and the neck. The eyes are also highly sensitive to x-rays, so wearing goggles with lead protection is helpful to reduce the dose load here.
Regarding the position of the patient table while working with the angiographic equipment, the results show, that especially for the RAO-caudal basic projection, the lowest dose is received at the lowest position of the patient table (due to the largest number of high values measured). Therefore, the dose load for the interventional cardiologist would be the lowest in this position.
For LAO-caudal, the lowest values are observed at the lowest table position, which will give the lowest dose load.
When working in the Pure Cranial projection, the values for the lowest and highest table positions are comparable. Therefore the dose load will be almost the same at these two table positions.
5. Recommendations
From the conclusions made so far, we could summarize the following recommendations to reduce the dose load of medical staff performing LCx stenting under X-ray guidance:
1) A minimum duration must be achieved to perform a quality procedure, especially when working under x-ray guidance in radiographic mode;
2) A patient table position should be used that is as comfortable as possible for the principal interventional cardiologist. For LAO-caudal as basic projection a position of the patient table should be used which is as close as possible to the lowest position; for RAO-caudal―the table position should be near the highest position. For Pure Сranial the lowest or the highest position of the patient table can be used;
3) In this LCx stenting procedure, it is recommended not to use a position of the patient table close to zero (factory set position), because in this position the dose load is the highest;
4) Individual protective equipment must be used during work―apron, collar, goggles and hat of lead equivalent not less than 0.5 mm.
Compliance with these recommendations would result in a reduction in the x-ray dose obtained from scattered radiation during the angiographic LCx stenting procedure.
Acknowledgements
Special thanks to the three physicians, members of our research team, from the Cardiology Hospital, Varna, Bulgaria: Dr. Ismet Tahsinov, Ph.D. Hrisimir Todorov, Ph.D. Nikolai Aleksandrov, without whose invaluable help our team would not have done so well.
Special thanks also to Eng. Yavor Ivanov from S&T Bulgaria, Bulgaria (official representative of Philips for Bulgaria), technical equipment engineer, who created optimal conditions for the x-ray examination.
Special thanks to Natasha Ivanova from the Medical University, Varna for the provided data, on the basis of which we prepared this article.
And last but not least, special thanks to the editors of the magazine for their help in printing the article.