Local anaesthesia using Articaine and Lidocaine in oral and dental surgery: A comparative meta-analysis ()
First introduced in 1976, 4% articaine solutions have shown high levels of anaesthetic potency and low systemic toxicity in clinical situations, due to its pharmacological profile and physicochemical characteristics [3]. Regional nerves blocks and local infiltration are the most commonly used anaesthetic administration techniques for mandibular teeth; however, buccal infiltration anaesthesia of the mandibular first molar would be beneficial to both clinicians and patients in terms of the ease and comfort [4].
The preference of a local infiltration over that of regional block has previously been described. For the clinician, the ease and speed of administration would be beneficial to the anxious patient. It has also been suggested that there might be fewer risks in patients taking anticoagulant therapies. If a local infiltration of Articaine could provide more effective analgesia than Lidocaine then it might be a preferable analgesic for use in most routine dental procedures.
The authors undertook this study to explore the possibility of using of Articaine (4AA) as a buccal infiltration alone to anesthetise mandibular first molar teeth, allowing dental, and some minor oral surgery procedures where surgical access is via the buccal cortex.
2. OBJECTIVES
To determine how effective buccal infiltration of 4AA is in producing mandibular permanent first molar pulpal anaesthesia when compared to 2LA.
3. MATERIALS AND METHODS
3.1. Literature Searching
The electronic databases of Ovid MEDLINE®, EMBASE®, PubMed®, Scopus ®, Scirus® and Cochrane Central Register of Controlled Trials were interrogated to identify relevant citations of published trials. In order to identify relevant unpublished or on-going trials further searches of the metaRegister of controlled trials register was also investigated. Table A1 gives the details of the databases searched along with the search strategies used. Attempts were made to contact the leading manufacturer of articaine within the UK (Septodont®) with regard to any information concerning on-going trials.
3.2. Selection of Studies
Randomised controlled trials (RCTs) fulfilling certain specified criteria were selected (Table 1). Cohort studies, case series and case reports are excluded from the review owing to the high potential for bias in these study designs. Case-control studies (except where nested as part of a cohort study) and economic evaluations are also excluded. Trials investigating the efficacy of buccal infiltrations of 4AA and 2LA administered to mandibular first molar teeth were included. A detailed list of the exclusion criteria is located in Table A2. The search process detailing the number of studies excluded at each point of the data collection is shown in Figure 1 and is detailed in Table A1.
3.3. Data Abstracts and Study Characteristics
The titles and abstracts obtained from the search were independently screened as suggested in the PRISMA protocol [5]. All obtained citations were checked to ensure that they fulfilled the inclusion criteria (Table 1). Those satisfying the criteria were then retrieved for analysis.
The data retrieved was extracted to Microsoft Excel® and included the authors, year of publication, study design, sample size, age range, intervention details with regards to the type of anaesthetic used and the measures of effectiveness were recorded (Table 2). The data detailing the time of onset and duration of onset of the anaesthetic were recorded; the data recorded for anaesthetic success was extracted. The data was analysed using StatsDirect®.
The assessment criteria according to COHORT [6] and individual study rating can be located in Table A3. All of the studies stated that appropriate approval and consent of participants was taken.
4. RESULTS
Studies published between 1946 and the present were included within the meta-analysis. The author and a review team screened 177 citations. Data from three randomised controlled trials were included within the statistical analysis (Tables 2 and 3).
The relative efficacy of articaine when compared to lidocaine was calculated for each of studies included (Table 3) and used to obtain the synthesis value (Table 4). This is best illustrated by the forest plot (Figure 2). Therefore, the relative efficacy of 4AA over 2LA in anesthetizing permanent first mandibular molars was calculated at 1.57 (95% CI = 1.27 to 1.95).
Cochrane’s Q and I2 values were calculated from the raw data. Although though no significant heterogeneity was seen in the forest plot a random effects model was employed for the analysis due to the small number of relatively small studies included (as shown in Figure 2).
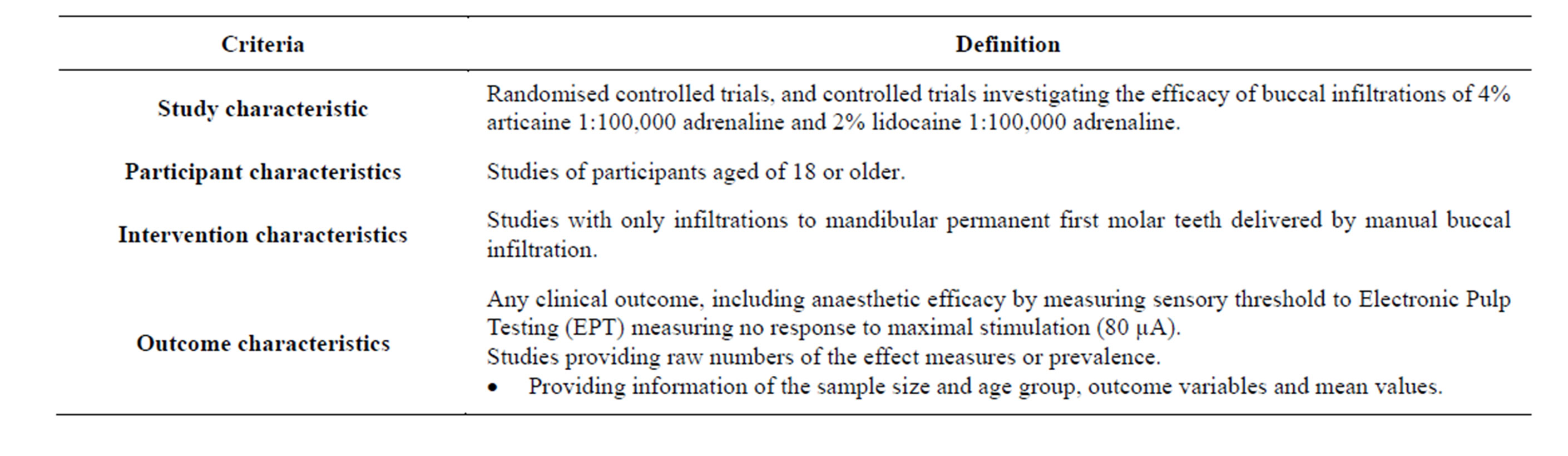
Table 1. Criteria for selection of studies included in meta-analysis.
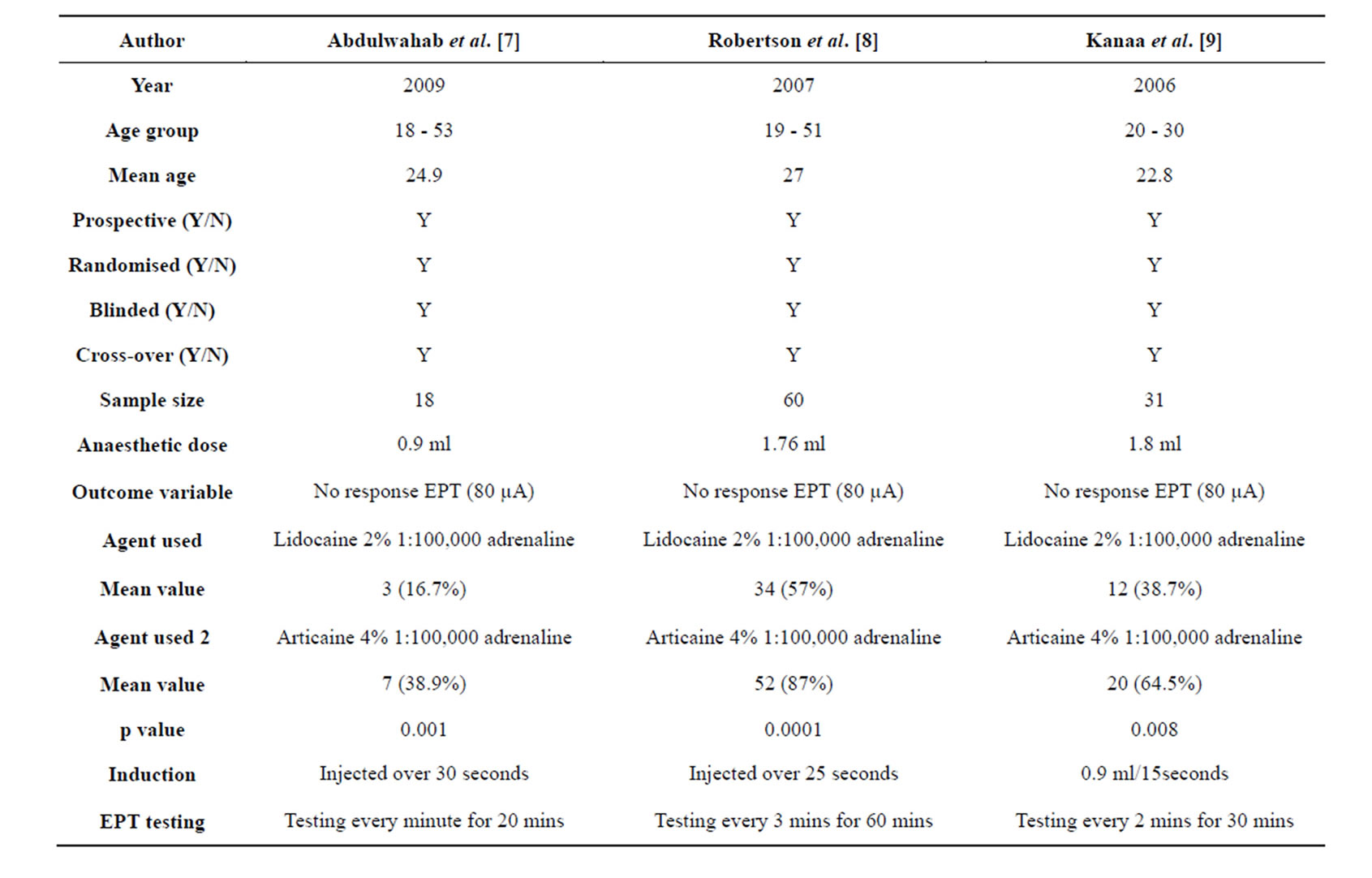
Table 2. Summary of trial characteristics.

Table 3. Extracted data for meta-analysis.
5. DISCUSSION
5.1. Key Findings
This meta-analysis suggests that the anaesthetic efficacy of 4AA when used as a mandibular buccal infiltration is greater than that of 2LA.
5.2. Biological and Clinical Interpretation
Though the mechanism for the increased efficacy of articaine is not fully understood, Skjevik et al. [10] have suggested that Articaine exhibits an exceptional effectiveness in bone tissue penetration along with an additional unique lipophilicity switch in its ability to form an intra-molecular hydrogen bond.
Many studies have investigated articaine buccal infiltration anaesthesia and its application with regards to maxillary and incisor teeth [11,12]. While some have reported no significant difference between the use of articaine or lidocaine [13] many maintain that 4AA is more effective than 2LA in achieving pulpal anaesthesia. Additionally, the onset of pulpal anaesthesia with articaine has been shown to be significantly faster than Lidocaine via buccal infiltration (P = 0.03), with a significantly longer duration of soft tissue anaesthesia (3.8 h vs. 2.5 h; P < 0.0001) [14,15].
5.3. Limitations
The included studies are based upon the use of 2% lidocaine with 1:100,000, adrenaline (epinephrine) whereas the most commonly used formulation for dental and oral surgical procedures in the UK employs adrenaline at the slightly higher concentration of 1:80,000. The concentration difference in vasoconstrictor may well account for a difference in clinical soft-tissue anaesthesia time mean-

Figure 2. Relative risk meta-analysis forest plot (random effects).
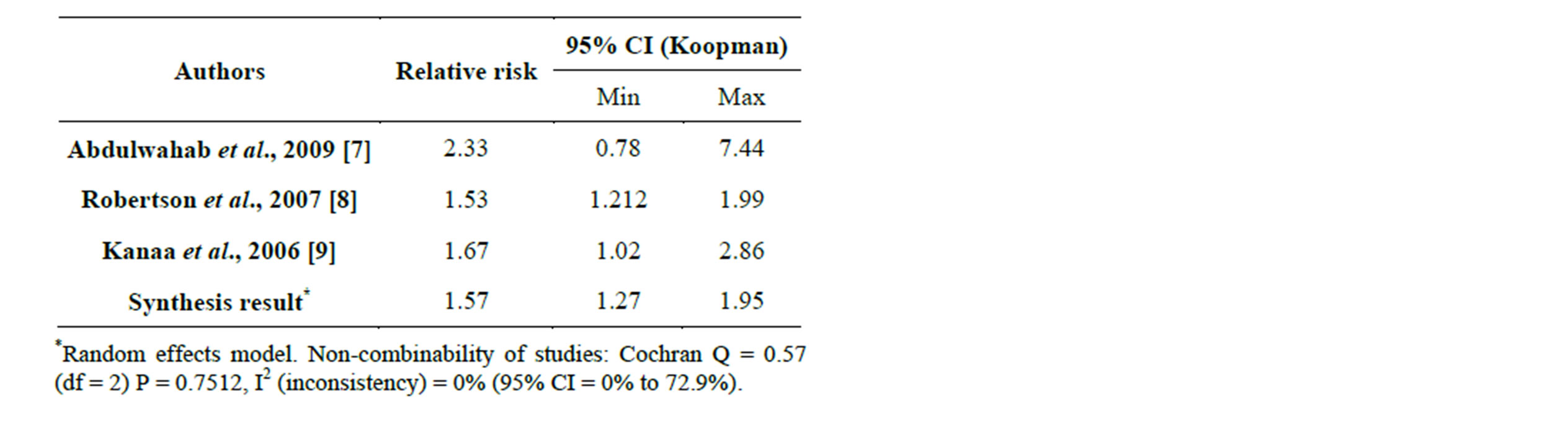
Table 4. Comparison of relative efficacy between studies.
ing that the use of 4AA may make little difference in this aspect.
The trials included in the meta-analysis all considered pulpal anaesthesia to have been achieved following the absence of response to the maximal stimulation (80 µA) with the electronic pulp tester on two or more episodes of testing. These results may not be directly transferable to oral surgical procedures such as the extraction of teeth which require anaesthesia of the structures surrounding the tooth.
As only a limited number of trails were available for inclusion within this meta-analysis it is premature to suggest that buccal infiltrations of 4AA in the mandibular region should be the anaesthetic agent and technique of choice.
5.4. Comparison to Previous Work
A meta-analysis conducted by Katyal, [16] investigating the efficacy and safety of articaine versus lidocaine in dental treatments supports the argument that articaine is more effective then lidocaine in providing anaesthetic success in the first molar region. Although higher pain scores for delivery were recorded, articaine has still been suggested as superior for use as an anaesthetic agent in dental treatment.
6. CONCLUSION
In this study 4AA has been shown to have greater efficacy in achieving pulpal anaesthesia in mandibular permanent first molar teeth than 2LA when administered via buccal infiltration on analysis of three studies. The increase in efficacy may be as high as 1.57. The small numbers of available studies in this analysis indicate that more work is required before the results can be directly translated into clinical practice.
ACKNOWLEDGEMENTS
I would like to thank Mr S. Parmar (Consultant in Oral and Maxillofacial Surgery) for his contribution to this work.
APPENDIX
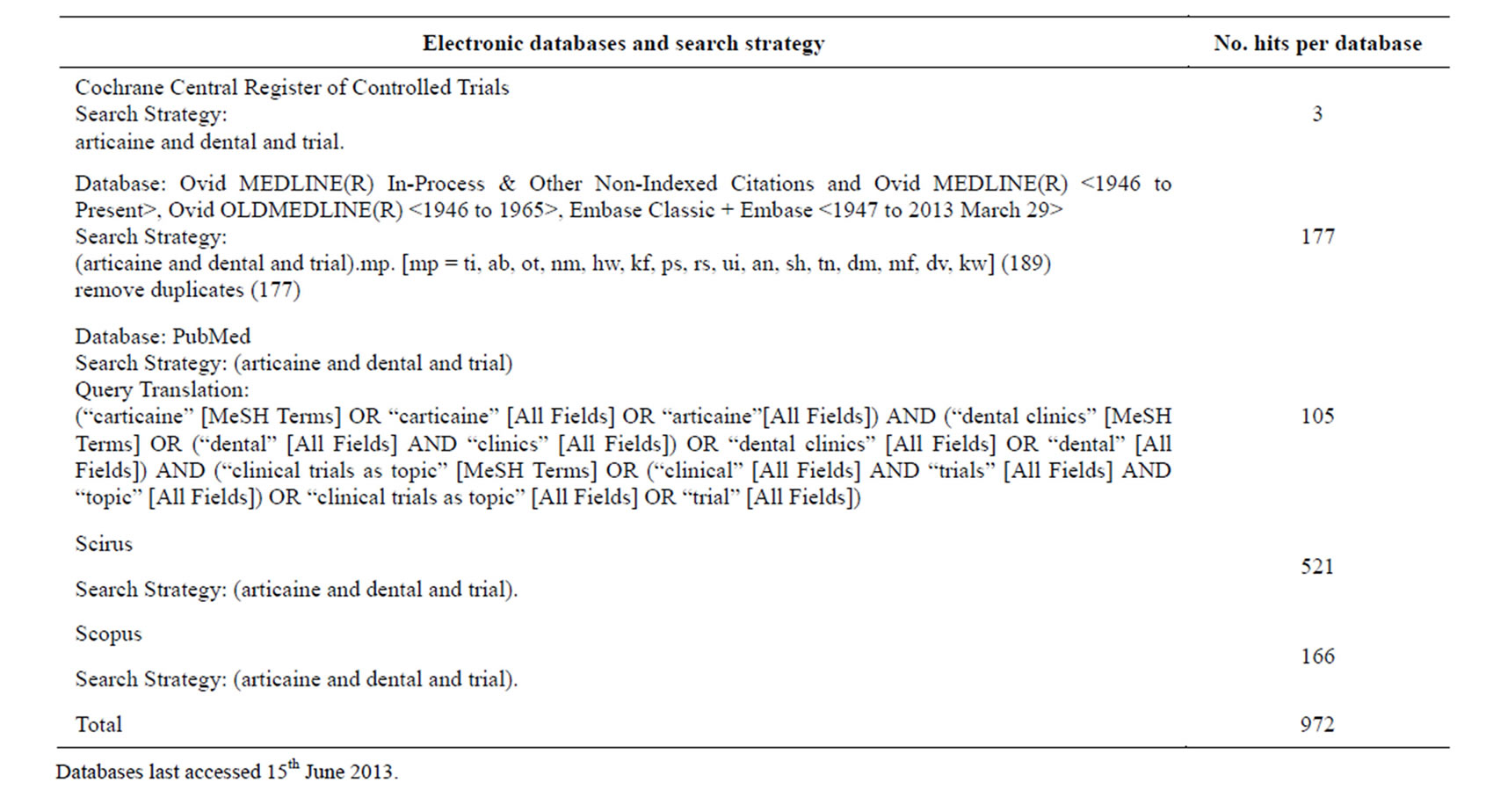
Table A1. A table outlining search strategies and number of hits per database.

Table A2. Data search exclusion criteria.
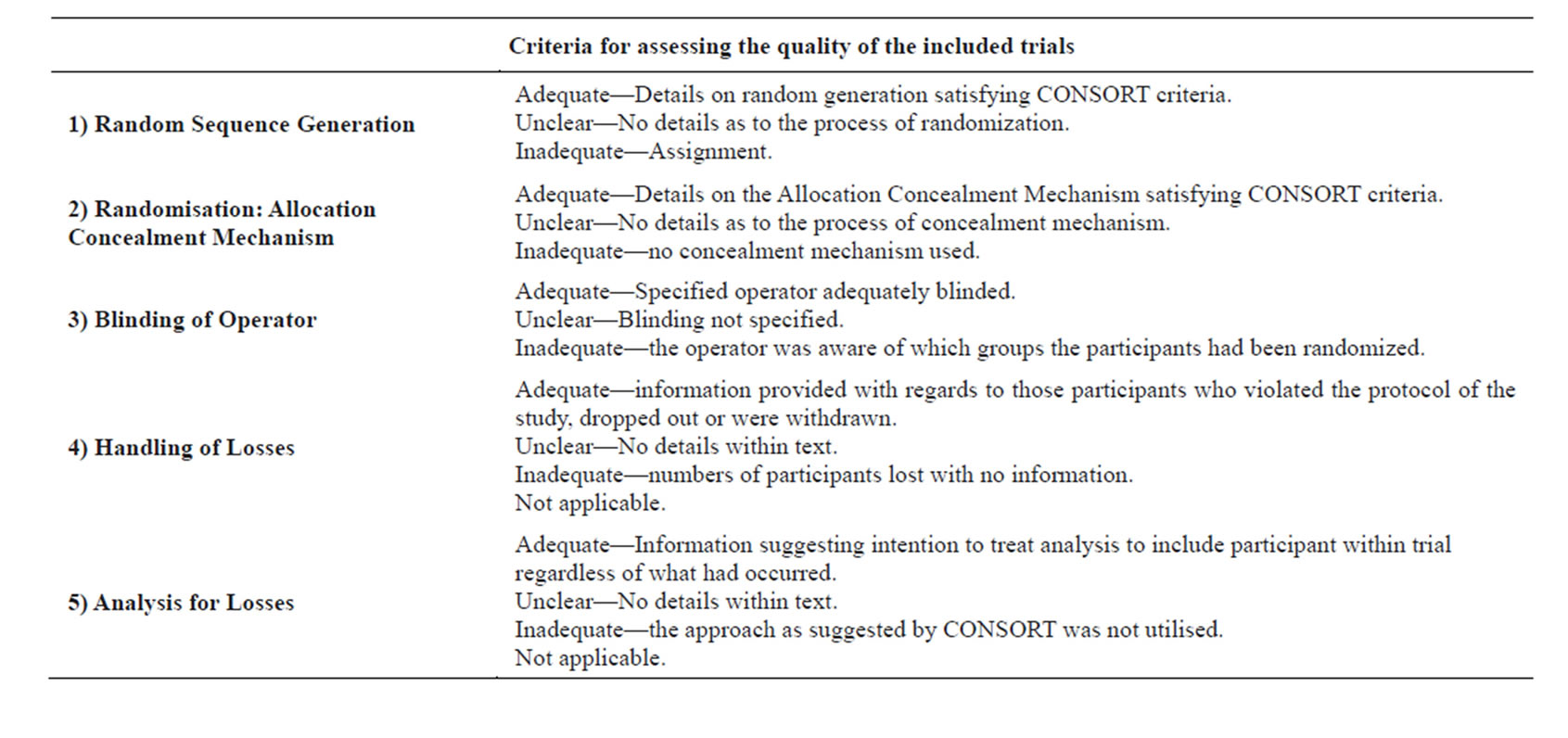
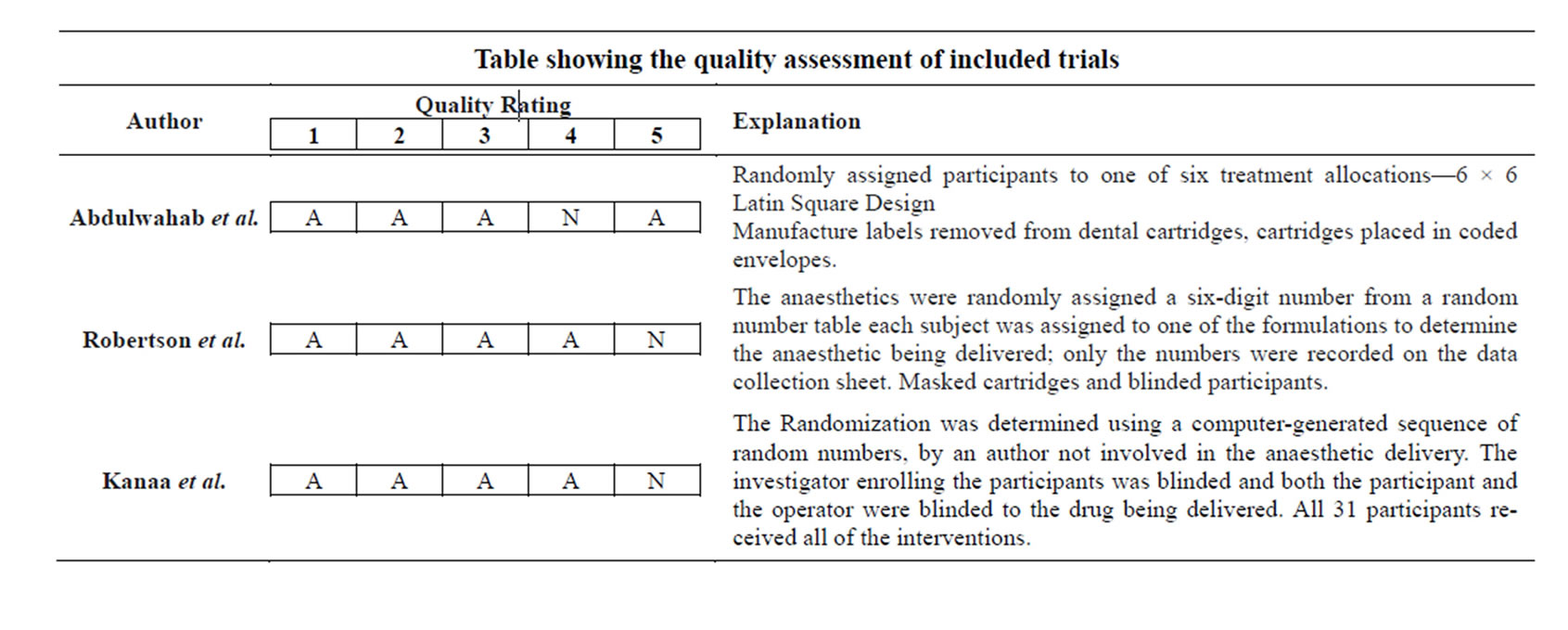
Table A3. Criteria for quality and the quality assessment of the included trials.