Amino acid profiles in relation to chronic periodontitis and rheumatoid arthritis ()
There is evidence to suggest the similarities in the plasma cytokine and gene expression profiles between patients with RA and those with periodontitis [7,8]. The pathogenesis of both diseases is also characterized by increased levels of circulating matrix metalloproteinases, reactive oxygen species, lipid mediators, and neutrophilassociated enzymes [1,2]. Furthermore, it has been proposed that polymorphisms relating to genes encoding inflammatory cytokines might confer susceptibility to RA and periodontitis [9-11]. These findings suggest an importance to predict individuals at a high risk of developing RA and periodontitis with a circulating biomarker.
Recently, a significance of profiling plasma multiple metabolites including amino acids has been demonstrated for diagnosis of RA [12,13]. It has been reported that patients with RA and psoriatic arthritis could be distinguished with high sensitivity and specificity by detection of amino acids [12]. Additionally, plasma levels of metabolites were shown to be associated with disease activity of RA [13]. However, there is no information to date on amino acid profiles in plasma from patients with periodontitis, although there has been a few earlier studies with analysis of saliva and gingival crevicular fluid from the patients with periodontal disease [14,15]. Therefore, the aim of the present study is to compare plasma levels of amino acids among patients with RA and CP, and healthy individuals.
2. MATERIAL AND METHOD
2.1. Participants
Sixty-two Japanese adults with RA (53 females and 9 males; mean ± standard error [SE] age 60.8 ± 1.6 years) (RA group) followed at the Niigata Rheumatic Center, Shibata, Japan, were recruited between July 2010 and August 2011 in the present study. All patients were confirmed to fulfill the 1987 revised classification criteria of American Rheumatism Association [16]: 1) morning stiffness in and around joints lasting at least 1 hour before maximal improvement; 2) soft tissue swelling of 3 or more joint areas; 3) swelling of the proximal interphalangeal, metacarpophalangeal, or wrist joints; 4) symmetric swelling; 5) rheumatoid nodules; 6) the presence of rheumatoid factor; and 7) radiographic erosions and/or periarticular osteopenia in hand or wrist joints. Criteria 1) through 4) must have been present for at least 6 weeks. RA was defined by the presence of four and more criteria. All patients fulfilled the following three exclusion criteria: 1) the presence of diabetes mellitus and pregnancy, 2) having antibiotic treatment within the previous 3 months, 3) a history or the presence of any periodontal therapy and mouth rinse usage within the previous 3 months. The duration of RA and medication of corticosteroids, disease-modifying antirheumatic drugs (DMARDs), nonsteroidal anti-inflammatory drugs (NSAIDs), and tumor necrosis factor-alpha (TNF-α) inhibitors were examined at the time of the examination.
A group of 30 race-, age-, gender-, and smoking status-balanced adults with CP only (25 females and 5 male; mean ± SE age 61.6 ± 1.4 years) (CP group) and 29 race-, age-, gender-, and smoking status-balanced healthy individuals with no signs of systemic diseases and periodontitis (24 females and 5 males; mean ± SE age 54.5 ± 2.6 years) (H group) referred to the Periodontics and General Dentistry Clinic of the Niigata University Medical and Dental Hospital, were included July 2010 and August 2011. The presence of periodontitis was defined as having at least one site with clinical attachment level (CAL) ≥ 4 mm [17]. Individuals who exhibited no signs of periodontitis, as determined by the absence of sites with CAL > 3 mm were assigned to the H group. Signed informed consent was obtained from all participants; the format of the study was reviewed and approved of Ethical Committee for the use of Human subjects in research, Niigata University Faculty of Dentistry (No. 22-R9-10- 06, on June 16, 2010), and Niigata Rheumatic Center (No. 1, on April 26, 2010).
2.2. Clinical Assessments
Clinical periodontal assessments were performed by two calibrated examiners (T.K. and M.O.) who were masked from the group assignments and the rheumatologic data. The calibration was performed before the study with 5 volunteer subjects in Niigata University Faculty of Dentistry. Reproducibility of the clinical measurements was calculated by means of the κ index, and a value of 0.857 was obtained for CAL with a difference of ±1 mm. All participants were evaluated clinically in the following measurements: number of teeth present, probing depth (PD), CAL, supragingival plaque accumulation, and bleeding on probing (BOP). The presence or absence of supragingival plaque and BOP were recorded at four and six sites around each tooth, respectively. Measurements of PD and CAL were conducted with a Williams probe at six sites around each tooth, recorded to the nearest millimeter, and every observation close to 0.5 mm was rounded to the lower whole number. The averaged score for whole-mouth PD, CAL, and the number of sites with plaque and BOP divided by the total number of sites per mouth and multiplied by 100 were calculated for each subject.
The disease activity of RA was determined with Disease Activity Score including 28 joints using C-reactive protein (DAS28-CRP), constituting four categories: remission (DAS28-CRP < 2.3), low (2.3 ≤ DAS28-CRP < 2.7), moderate (2.7 ≤ DAS28-CRP < 4.1), and high disease activity (4.1 ≤ DAS28-CRP), which underestimates disease activity compared with DAS28 using erythrocyte sedimentation rate (DAS28-ESR) in Japan [18]. Smoking status of the participants was classified as currentsmokers, former-smokers, or never-smokers, according to information provided on a standard questionnaire.
2.3. Measurements of Inflammatory Markers
Peripheral venous blood samples were obtained from all participants and placed on ice within 5 minutes. Plasma was isolated within 4 hours from the blood samples by centrifugation at 1500 g for 20 minutes, and stored at −70˚C until use. Concentrations of rheumatoid factor (RF) and high-sensitive CRP were determined with a latex particle-enhanced and a simple nephelometric method (SRL, Tokyo, Japan). Levels of interleukin-6 (IL-6), TNF-α, and anti-cyclic citrullinated peptide (CCP) antibodies were determined by sensitive enzyme-linked immunosorbent assay (ELISA) (IL-6 and TNF-α: R&D Systems, Minneapolis, MN, USA; anti-CCP: Medical & Biological Laboratories, Aichi, Japan), according to the manufacturer’s instructions. The microtiter plates were read at a wavelength of 450 nm with an automated microplate reader (Bio-Rad Japan Laboratories, Tokyo, Japan). The lower limits of detection for these measurements were as follows: RF, 1.25 IU/ml; CRP, 0.004 mg/ dl; IL-6, 0.016 pg/ml; TNF-α, 0.038 pg/ml; anti-CCP antibodies, 0.4 U/ml. Positivity of RF and anti-CCP antibodies was defined as showing more than15 IU/ml and 4.5 U/ml, respectively. Levels of measurements below the lower limit of detection were recorded as being not determined.
2.4. Measurements of Amino Acids
Plasma levels of amino acids were determined with precolumn derivatization high performance liquid chromatography/electrospray mass spectrometry [19]. The following 21 amino acids and related molecules were measured: Glycine (Gly), Alanine (Ala), Serine (Ser), Proline (Pro), Valine (Val), Threonine (Thr), Isoleucine (Ile), Leucine (Leu), Aspragine (Asn), Glutamine (Gln), Glutamic Acid (Glu), Methionine (Met), Histidine (His), Phenylalanine (Phe), Arginine (Arg), Citrulline (Cit), Tyrosine (Tyr), Tryptophan (Trp), Ornithine (Orn), Lysine (Lys), alpha-aminobutyric acid (α-ABA).
2.5. Statistical Analyses
The required sample size was more than 15 subjects in each group, which was based on power calculation test with repeated-measures analysis of variance with 5% of alpha level, 0.14 of obtained effect size, 0.8 of statistical power level. After evaluating the normality of distribution by Kolmogorov-Smirnov test, differences in clinical and laboratory parameter values were assessed among the three groups by Kruskal-Wallis test, and when significant differences were detected, further assessment of differences between the two groups were done by Scheffe’s test. The Spearman’s rank correlation coefficient analysis was used to determine the relationship between levels of amino acids and periodontal conditions. Statistical significance was accepted at 1% (p < 0.01).
3. RESULTS
Table 1 shows the demographic, clinical, and laboratory parameter values of RA, CP, and H groups. Both the RA and CP groups exhibited significantly less number of teeth and higher scores of periodontal parameters (% of sites with plaque and BOP, PD, CAL, and % sites with PD and CAL ≥ 4 mm) than the H group (P < 0.01). However, these dental parameter values proved comparable between the RA and CP groups (P > 0.01). Levels of CRP, IL-6, and TNF-α were significantly higher in the RA group than those in the CP and H groups (P < 0.01).
As shown Table 2, levels of four amino acids (Gly, His, Orn, and α-ABA) were significantly different among the three groups (P < 0.01). The RA group displayed significantly lower levels of Gly and His and significantly higher Orn level than the CP and H groups (P < 0.01). On the other hand, the CP group showed significantly higher α-ABA level than the RA and H groups (P < 0.01).
Of these four amino acids, a significantly positive correlation was found between Orn level and % of sites with BOP (P = 0.006) in the RA group (Table 3). No associations were obtained between amino acid levels and periodontal conditions in the CP group (P > 0.01) (Table 3).
4. DISCUSSION
The percentage of females was 85.5%, the mean age was 60.8 years, and the mean RA duration was 11.6 years in the RA group in the present study. These observations are almost in accordance with the results of race-matched large-cohort (7512 patients) IORRA and (3073 patients) Ninja studies [20,21]. The frequencies of patients with remission, low-, moderate-, and high-activity, as measured with DAS28-CRP, as well as RA medication were almost comparable between the present and other studies [20,21]. Furthermore, patients with RA exhibited higher levels of CRP, IL-6, and TNF-α than the age-, gender-, smoking status-, and periodontal condition-balanced individuals with CP, which is consistent with the results of previous study [8]. These findings imply that patients with RA who participated in the current study were representative of the general Japanese RA population.
Determination of the plasma concentrations of amino acids is important for understanding the pathophysiology of inflammatory diseases such as RA and periodontitis. However, it is necessary to pay an attention for management of blood samples. It has been demonstrated that delays in processing of blood samples caused a rapid change in amino acid concentrations [22]. Therefore, in the present study, blood samples were placed on ice within 5 minutes after collection, and plasma was isolated within 4 hours to avoid degradation of amino acids.
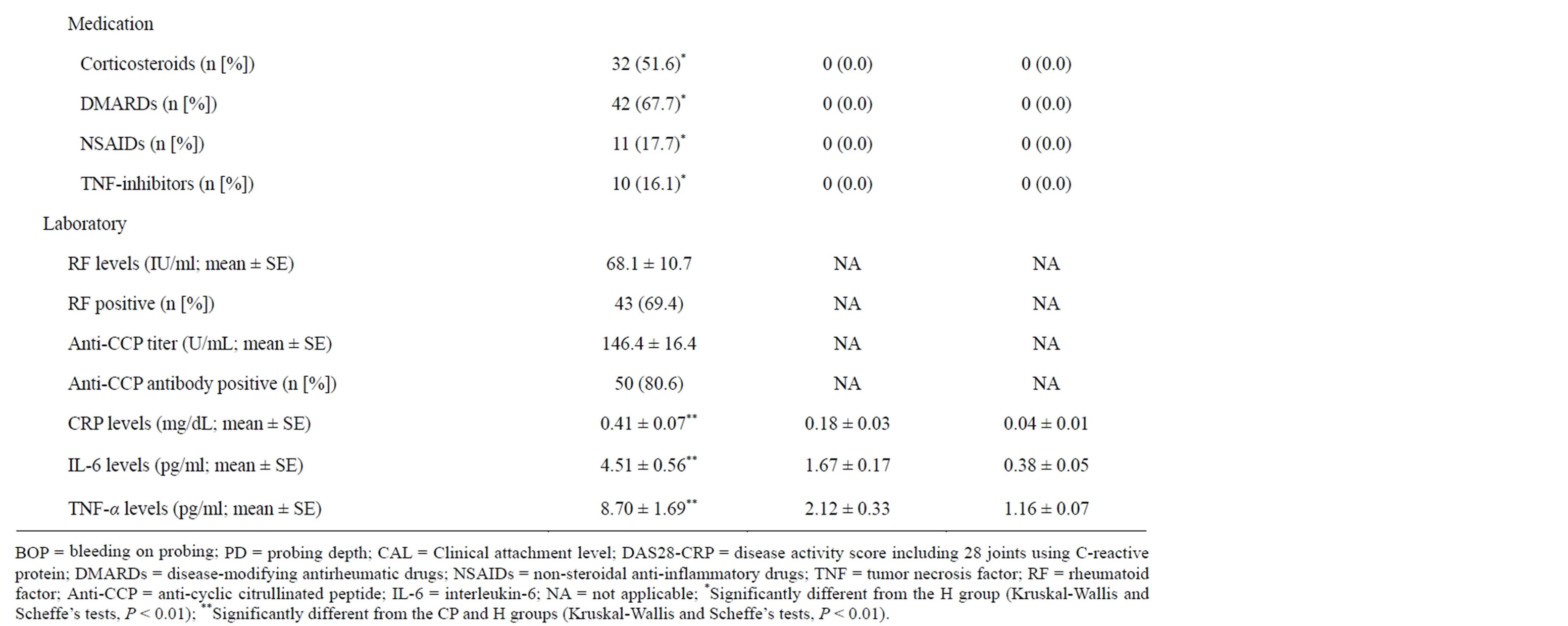
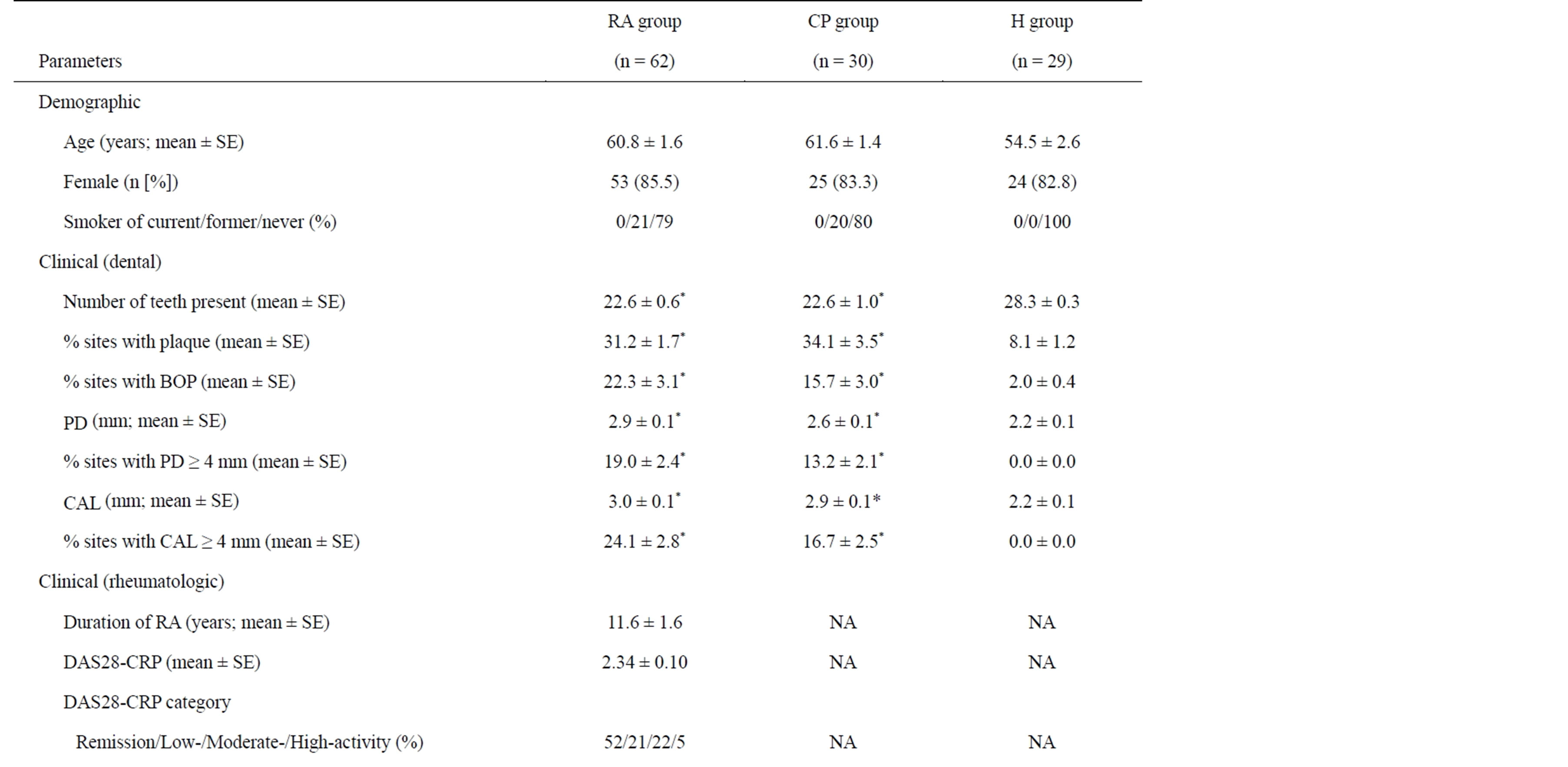
Table 1. Demographic, clinical, and laboratory characteristics of patients with rheumatoid arthritis (RA) and chronic periodontitis (CP), and healthy controls (H).
The present results indicated decreased levels of Gly and His in patients with RA compared with individuals with CP and healthy controls, which is supported by the results of other studies [12,23,24]. It has been docu-

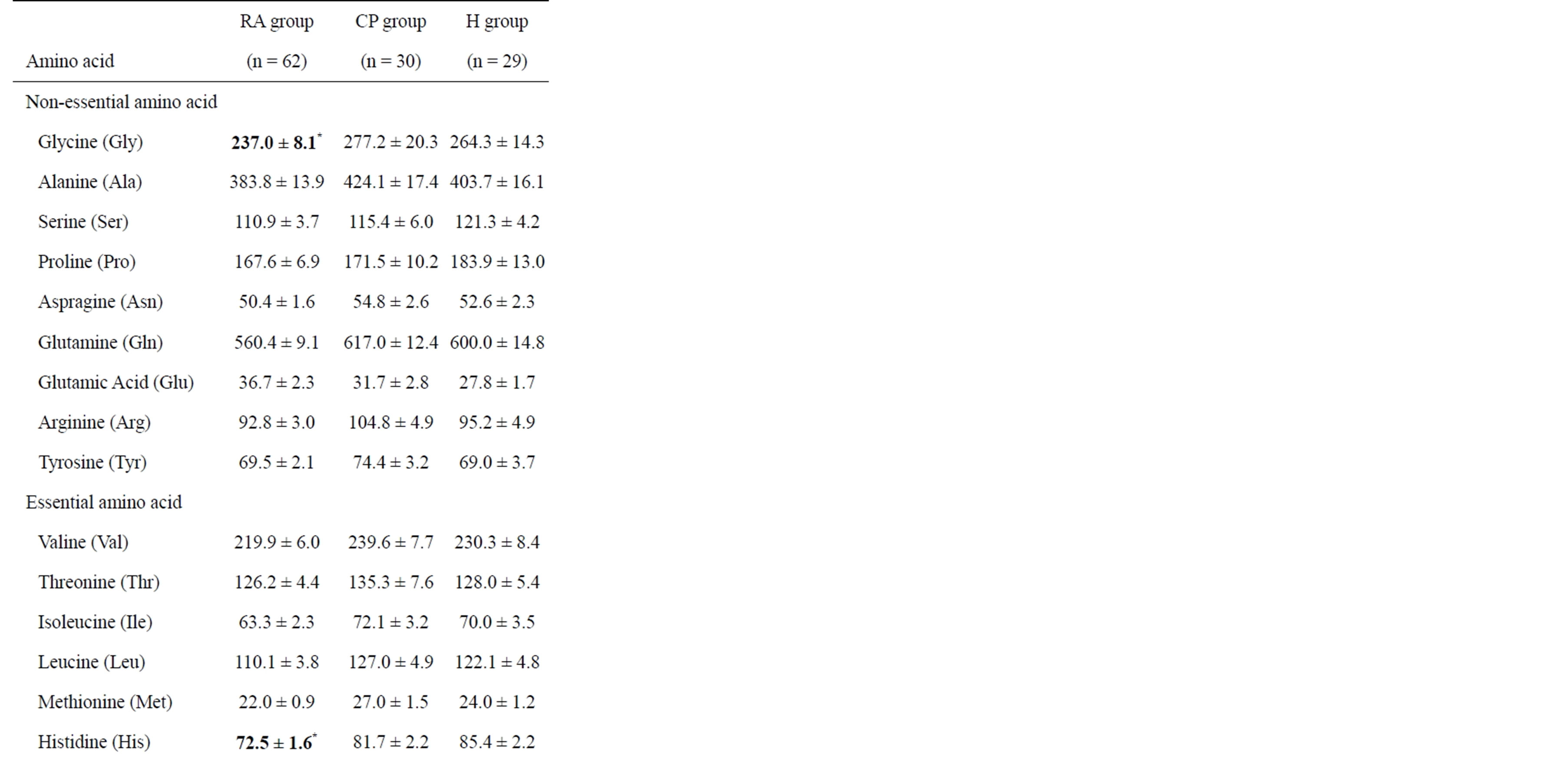
Table 2. Amino acid levels in patients with rheumatoid arthritis (RA) and chronic periodontitis (CP), and healthy controls (H).
mented that patients with RA exhibited lower levels of His than healthy individuals [12]. The decreased His level in RA has been partially explained by increased degradation of His through the His decarboxylase [23]. It has also been reported that the decrease in plasma Gly levels was observed in patients with RA, whose significance in the pathogenesis of RA has not been discussed

Table 3. Correlations between amino acid levels and periodontal conditions in patients with rheumatoid arthritis (RA) and chronic periodontitis (CP).
[24].
Notably, the present data showed that Orn level was increased in patients with RA compared with healthy individuals, which is different from the results of other study [24]. Additionally, Orn level was positively correlated with periodontal inflammation as determined with BOP in patients with RA, but not in individuals with CP and healthy controls. To best of our knowledge, this is the first study demonstrating an association of Orn profile with CP and RA. However, it cannot be concluded from these findings alone whether Orn plays a role in the pathogenesis of RA and periodontitis. Further studies would be required to evaluate longitudinally the effects of Orn and its metabolism on periodontal condition in patients with RA.
Interestingly, similar amino acid profiles were obtained in the present study between individuals with CP and healthy controls, except for α-ABA. These observations are different from earlier studies showing that patients with periodontal disease exhibited considerable amino acid variations in saliva and gingival crevicular fluid [14,15]. These inconsistent results might be partly explained by clinical periodontal condition or blood sample management between the present and other studies [14,15]. It has been reported that α-ABA did not take part in protein synthesis and was only associated with sepsis [25]. Therefore, it would be necessary to perform the clinical and in vitro studies to confirm and extend the observations obtained in the present study.
5. CONCLUSION
The results of the present study suggest a possibility that profiles of four amino acids (Gly, His, Orn, and α-ABA) may play a role in the pathogenesis of CP and RA.
ACKNOWLEDGEMENTS
The authors declare no conflict of interest related to this study. This work was supported by Grant-in Aid for Scientific Research A (No. 25253104) and C (No. 22592309) and Grant-in Aid for Challenging Exploratory Research (No. 24659922) from the Japan Society for the Promotion of Science, Tokyo, Japan.