Factors Predictive of Right Internal Jugular Vein Cross-Sectional Area Change in Response to Trendelenburg Positioning ()
1. Introduction
In cardiac surgical patients, the right internal jugular vein (RIJV) is the most commonly central venous access site [1]. Trendelenburg position is commonly used to promote venous distention to facilitate the vascular cannulation [2-8]. Jugular veins are thought to be more responsive to Trendelenburg positioning than subclavian [9]. However, factors predictive of the degree of venous dilation are largely unknown. A systematic search of the National Library of Medicine (PubMed) revealed no studies of factors predictive of, or associated with, the responsiveness of jugular veins to Trendelenburg maneuver. We, therefore, studied the factors likely associated with the jugular venous responsiveness to Trendelenburg position in anesthetized patients.
2. Methods
Institutional Review Board approval was granted for the study, and a signed consent form was obtained from each patient. Thirty-seven patients scheduled to undergo coronary artery bypass or valve surgery (cardiovascular disease (CVD) group), and 20 ASA I and II patients presented for non-cardiothoracic surgery, were enrolled over an 8-month period. Exclusion criteria included conditions that could have interfered with the responsiveness of RIJV or the ability to measure it, such as indwelling catheters, neck pathology, previous neck surgery, renal failure and congestive heart failure.
Imaging and measurement of the RIJV cross-sectional area (CSA) was accomplished using vascular ultrasonography (Sonosite, Inc., Bothwell, WA) in the supine position after induction of general anesthesia and initiation of mechanical ventilation. Measurements were obtained in level position and repeated in the 10-degree Trendelenburg. CSA of RIJV was used in lieu of its diameter due to its irregular complex shape [10]. Planimetric CSA measurements were made from the RIJV sort-axis view in the apex of the anterior triangle formed by the bifurcation of the clavicular and sternal heads of the sternocleidomastoid muscle, a site typically chosen for RIJV cannulation.
RIJV was cannulated as part of anesthetic plan in cardiac surgical patients. The central venous pressure (CVP) was measured and recorded at end-expiration in level supine position with the transducer at the level of midaxillary line. Perioperative transesophageal echocardiography (TEE) was used to estimate the left ventricular contractility, and recorded as ejection fraction (EF). No measurements of EF and CVP were made in the control group, as central venous cannulation and TEE were not indicated.
3. Statistical Methods
Categorical and continuous data are presented in Tables 1 and 2 as frequencies and percentages or means and standard deviations, respectively. Chi-square and Student’s t-test were used to compare the CVD and control groups. A linear mixed model was used to perform a repeated measures analysis of variance for the RIJV CSA
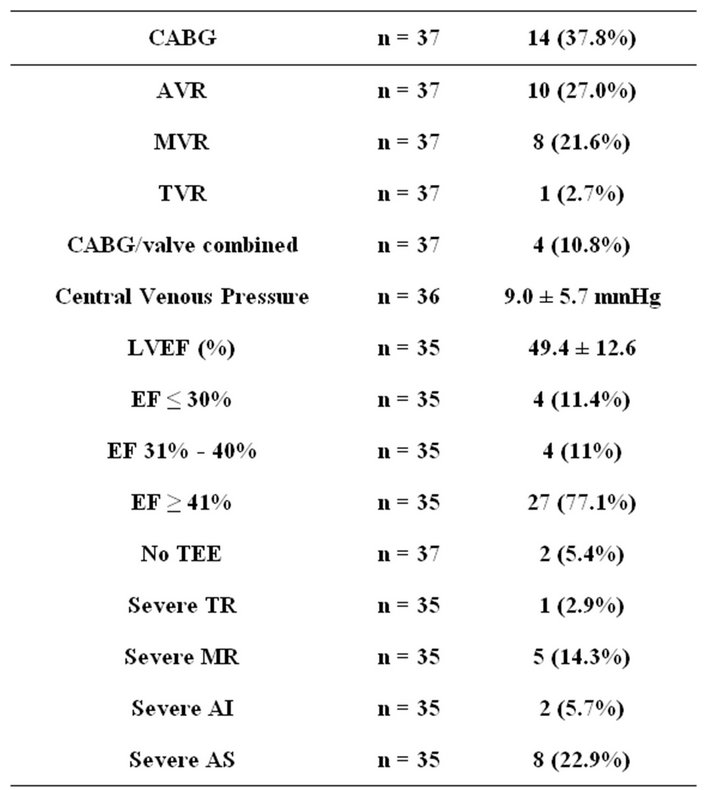
Table 2. CVD group: procedure, CVP, and TEE results.
data. The model included fixed effects for both groups (CVD and control) as the between-subjects factor, conditions (level and Trendelenburg) as the within-subjects factor, and the interaction between groups and conditions. Fixed covariates for age, sex, and interactions of group and condition with gender were also included in the model to control for their possible confounding effects. Subjects nested within groups were included as the random factor. An unstructured covariance matrix was used for the correlated error structure. Contrasts were used to compare conditions within groups and groups within conditions. The data are presented as adjusted means and standard errors in Table 3. SAS 9.2 (SAS Institute, Inc., Cary, NC) was used for all analyses. p = 0.05 probability level was used to determine the statistical significance of test results. Power analysis showed the required sample size of 34 to detect a significant moderate effect size of 0.5 in the change in CSA from supine to Trendelenburg at the two-tailed 0.05 level with 80% power.
4. Results
CVD and control groups were similar with regard to gender, body surface area (BSA) and body mass index (BMI). CVD patients were older than control patients, 69 vs. 62 years (Table 1). Surgical procedures, CVP and TEE findings for the CVD group are displayed in Table 2.
RIJV CSA data are shown in Table 3. In the CVD group, the CSA increased from 1.79 ± 0.14 to 2.01 ± 0.15 cm2 (p = 0.001), and in the control group from 1.82 ± 0.20 to 2.04 ± 0.23 cm2 (p = 0.013). There were no significant differences in CSA between the CVD and control groups in the supine (p = 0.905) or Trendelenburg (p = 0.935) positions, nor was there a significant difference in the CSA positional change between groups (p = 0.995). Central venous pressure had no independent effect on the size of the RIJV or its response to 10-degrees Trendelenburg. There was no correlation between the baseline CSA of the RIJV, or the dilatory response to Trendelenburg, in relation to patient age, BSA, BMI, or cardiac function. Notable was the wide inter-subject variability of the baseline (level) size of the RIJV. The observed values ranged 0.45 - 3.49 cm2 in the cohort of interest, and

Table 3. Supine and Trendelenburg cross-sectional area for CVD and control groups.
0.55 to 3.82 cm2 in control. The response to 10-degree Trendelenburg was unpredictable and variable, ranging from −11.4% to 57.5% in the cardiac patients and from −16.9% to 66.1% in control.
Although both groups showed a statistically significant dilatory response to 10-degree Trendelenburg position, only 24% of cardiac patients and 35% of controls had a dilatory response of greater than 20%, and less than half (49% of cardiac patients and 45% of the controls) exhibited dilatory responses of greater than 10%.
Gender differences in supine CSA and in response to Trendelenburg are summarized in Table 4. Controlled for BSA and age, male patients had significantly larger RIJV, both at level (p = 0.045) and in the 10-degree Trendelenburg position (p = 0.011). In male patients increase in RIJ SCA was significant (2.09 ± 0.16 cm2 to 2.43 ± 0.18 cm2, p < 0.001). In female patients no significant dilatory response to 10-degree Trendelenburg was observed (1.51 ± 0.20 cm2 to 1.62 ± 0.22 cm2, p = 0.167).
5. Discussion
Our data suggest that the change of RIJ CSA in response to Trendelenburg position is variable and largely unpredictable, particularly in female patients. Therefore, the risks of Trendelenburg position [11-14] should be considered in the light of its inconsistent venodilatory effects and unpredictable efficacy. Potentially deleterious hemodynamic and cerebrovascular effects of Trendelenburg maneuver include increased arterial, central venous, intracerebral and intraocular pressures, decreased cerebral perfusion pressure, and the potential for respiratory and cardiac compromise, especially in patients with pulmonary hypertension and abnormal respiratory mechanics [2,13,15,16].
Our findings are consistent with previous studies [1,8, 12]. Marcus et al. [1] studied effects of various levels of PEEP and 20-degree Trendelenburg position in 50 cardiothoracic surgical patients. A 20% increase in the CSA was defined as a clinically significant response—an effect achieved only in 54% of studied patients.
We were not able to demonstrate any correlation between the CVP and RIJV responsiveness. We believe our

Table 4. Gender difference in supine CSA and response to Trendelenburg; CVD and control groups.
observations further support the limited value of singlepoint measured CVP in assessment of intravascular volume [17].
Our data indicate a great variability in the size of the RIJV and the absence of any correlation between the degree of RIJ CSA change with Trendelenburg maneuver and commonly assumed factors such as body habitus, CVP or level size of RIJ. Therefore, our results support the ultrasound guidance as the only evidence-supported means of increasing the success rate of RIJ cannulation and decreasing the risk of complications [9,18,19]. The ultrasound examination allows the determination not only of the baseline level size of the RIJV (commensurate with the intended cannulation), but of the dilatory response to the Trendelenburg maneuver.
NOTES
#Corresponding author.