Methamphetamine and male suicide in the US-Mexico border region ()
1. INTRODUCTION
Toxicology plays a crucial role in studying suicide, since psychoactive substances are essential in the suicidegenerating stimuli [1]. Published studies on toxicology identify alcohol as the most frequent substance in nonoverdose and mixed method suicides followed by methadone and cocaine. Less frequent drugs include phencyclidine, cannabis, methamphetamine (MA), other opioids, antidepressants, methylendioximethamphetamine, gamma-hydroxybutiric acid, and petroleum [2-18]. Even though MA is not frequently identified in completed suicide, it is connected with impulsive behaviors (i.e. reckless driving, unprotected sex, gambling, suicide attempts), and important comorbidities (i.e. HIV/HCV infection, mood and psychotic disorders) [19-22].
MA is readily available in the United States-Mexico border region (USMBR) within a complex environment of consumption, production, and across the border smuggling [23,24]. Although drug abuse and dependence is less frequent, use of illegal substances is higher in young males (18 - 29 years) in this region than the rest of Mexico [25].
The USMBR refers to the 62.5 miles north/south of the international boundary. It stretches 2000 miles and encompasses 4 US states and 6 Mexican states [26]. The suicide rate has declined in the USMBR, but remains relatively high in certain States [27].
In the US side the suicide rate is highest in Arizona and New Mexico and lowest in Texas; and is slightly higher (11.0) than the national rate (10.4). The border suicide rate in 2000 consistently exceeded the national rate for groups over 45 years old. In the Mexico side, the suicide rate increased from 2.7 in 1990 to 5.5 in 2000, higher than the national rate of 3.6. More than half of all suicides are among people aged 25 - 44 years, while this age group accounts for one-third of all suicides at the national level [27,28]. We studied suicides in Mexicali, the third largest Mexican municipality in the USMBR.
2. METHOD
The Autonomous University of Baja California IRB approved this retrospective review of the autopsy database of all suicide victims from 1999-2005 in collaboration with the Forensic Medical Service (SEMEFO). Data collected included, sociodemographic variables (i.e. gender, age, marital status, educational level, occupation, home address, place of residence, place of birth, health coverage) and clinical variables (i.e. date and place of the
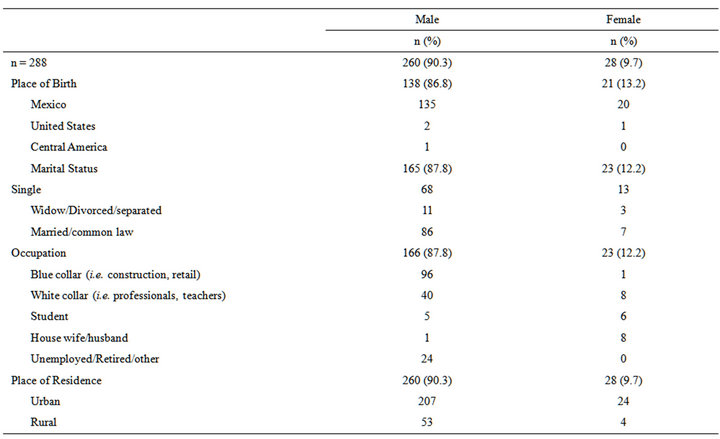
Table 1. Sociodemographic features.
event, method employed, and toxicological screen results). At this facility the toxicological screens tested for alcohol, cannabis, cocaine, heroin, and methamphetamine [29]. Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS 16.0), including chi square, t test, and ANOVA.
3. RESULTS
A total of 288 suicides were identified, mostly men (n = 260, 90.3%) across all age groups (p < 0.05). The sociodemographic findings are summarized in Table 1. The methods most commonly used were hanging (n = 188, 65%) and gunshot (n = 89, 31%).
Further analysis was focused on the 260 male victims, 164 were between 20 - 39 years old (63%), 96 were employed in blue collar jobs (i.e. retail, hard labor) (36%), 207 lived in an urban area (79%), and 122 were found in their homes (47%).
Toxicology screen was obtained in 211 victims and was positive in 118 (p < 0.001) (Table 2). MA was the most common and was present in 74 cases (61.8%, p < 0.001). It was alone in 38 (36%) cases, 16 (22%) combined with cocaine, 12 (16%) with alcohol, 7 (9%) with heroin, and 1 (1.3%) case with alcohol and heroin (p < 0.001, 0.327).
4. DISCUSSION
We studied 260 male suicide victims in Mexicali from 1999-2005. The modal male victim was a young urban blue-collar worker. Toxicological results were available in 211, with 64% positive, and the most common MA (p < 0.001) alone or combined with other substances.
Limitations imposed by the retrospective nature of this study prevent us from establishing any causal relationship. As well, prevents us from establishing if victims were occasional users or met criteria for MA abuse/dependence. Furthermore, we cannot ascertain if users had a preexisting disorder or developed psychiatric symptoms after using MA. Finally, one cannot conclude if victims died while intoxicated, as concentration levels were not recorded. Although no causal effect can be drawn, our study results suggest that methamphetamine use may be a risk factor for suicide in this sample. Nevertheless, prospective studies, are required to better understand these findings.
It is remarkable that previous studies report MA not nearly as prevalent as in our study [1, 6,10,25]. It is understandable that use of substances varies for reasons that go beyond the scope of this paper but in spite of limitations, our findings provide novel and unique data in a clinical, research and geographical area with insufficient information.
5. ACKNOWLEDGEMENTS
The authors thank the invaluable contribution of Dr. David FuentesRomero who was instrumental in the completion of this project, and due to his premature death is not in the authors list.
NOTES