Isolated Metastatic Barrett’s Adenocarcinoma of the Thoracic Epidural Space Causing Paraplegia ()
1. Introduction
Barrett’s esophagus, which is defined as intestinal metaplasia in the distal esophagus, is considered one of the risk factors of esophageal adenocarcinoma [1]. Most cases of esophageal carcinoma are pathologically squamous cell carcinoma among Japanese, however adenocarcinoma derived from Barrett’s esophagus called Barrett’s adenocarcinoma is increasing in number recently [2]. Although several case reports of the metastatic cancer in the epidural space have been documented, that derived from esophageal carcinoma is rare. To our knowledge, no cases of epidural metastasis without bone involvement from Barrett’s adenocarcinoma have been reported in the literature. We present here a case of metastasis to the thoracic epidural space from adenocarcinoma in Barrett’s esophagus that required surgical intervention due to progressive paraplegia.
2. Case Report
A 50-year-old man presented with a 2-day history of progressive weakness and numbness of lower limbs. Six months previously, he had a resection of the distal esophagus due to adenocarcinoma in Barrett’s esophagus. As metastatic para-aortic lymph nodes were observed during operation, complete lymphadenectomy was performed. No other organ metastasis or distant lymph nodes metastasis was detected by computed tomography of the chest-abdominal region. He was categorized as stage 4 according to the TNM stage classification. He could not walk nor stand from a squatting position. He complained of difficulty urinating in the morning. Neurological examination revealed that muscle motor test of lower limbs was 2/5 in iliopsoas, 2/5 in quadriceps, 3/5 in tibialis anterior, 3/5 in extensor hallucis longus, and 3/5 in gastrocnemius bilaterally. Severe deterioration of sense was manifested under the level of umbilicus. Deep tendon reflexes of both lower extremities were hypereflexia and Babinski response was obtained bilaterally. Plain radiographs and computed tomography of the thoracic spine revealed no signs of bone metastasis includeing bone destruction or erosion. Magnetic resonance imaging (MRI) of the thoracic spine revealed compression of the spinal cord at the T3-4 level by a dorsally located epidural mass with isointensity and enhanced on T1- weighted MR images and increased signal intensity on T2-weighted MRI (Figure 1). No signal changes were detected in vertebrae. Laminectomy of T3 and T4 and tumor resection was performed under general anesthesia since the paraplegia and urinary disturbance were rapidly progressing. The tumor was identified on the dorsal side of dura matter after laminectomy. No adhesion around the tumor was observed and the tumor was easily excised en bloc (Figure 2). Histopathological examinations confirmed a metastasic adenocarcinoma arising from the thoracic epidural space (Figure 3). Postoperatively, motor dysfunction and dysuria improved immediately and adjuvant chemotherapy was started. On follow-up MRI at 3-month postoperatively, the epidural mass disappeared and no other metastasis were detected although intramedullary increased signal on T2-weighted MRI appeared that was considered as a spinal cord injury (Figure 4). At 3 month after the operation, he was ambulatory with a walking aid. But he died 7 month after the operation due to lung metastasis. No recurrence of spinal region was observed on pathological anatomy.

Figure 1. Sagittal image of thoracic spine. Spinal cord was compressed by the dorsally located epidural tumor at the T3-4 level with isointensity and enhanced on T1-weighted MR images ((a) and (c)) and increased signal intensity on T2-weighted MRI (b).
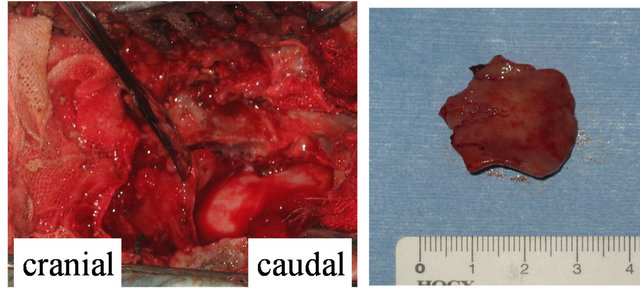
Figure 2. An intraoperative photograph (Left). The epidural tumor existed on dura matter without adhesion and was easily excised en bloc (Right).
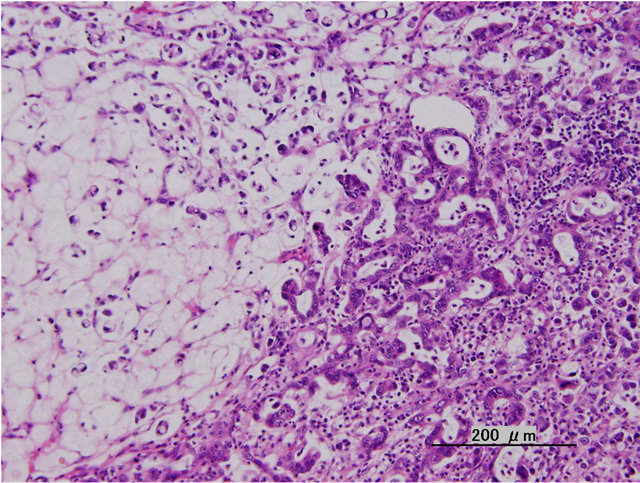
Figure 3. Histological appearance of epidural mass. Atypical epithelioglandular cells spread and formed an irregular glandular structure compatible with metastatic adenocarcinoma.

Figure 4. Axial T2-weighted image of the thoracic spine examined at 3 months after operation. The epidural tumor was excised entirely without any local reoccurrences.
3. Discussion
Barrett’s adenocarcinoma was defined as a tumor located in the tubular part of the esophagus and arising within the zone of Barrett’s metaplasia [3]. Barrett’s esophagus is considered to be strongly associated with esophageal adenocarcinoma [4]. The relative risk of adenocarcinoma among patients with Barrett’s esophagus was 10 - 40 times that of the general population, and the incidence rate was 1.2 to 5.0 per 1000 person-year from previous studies [5-7]. Adenocarcinoma accounts for almost half of esophageal cancers among Europeans and Americans, however the majority of esophageal cancers among Japanese are squamous cell carcinoma [2,8]. Although the incidence rate for adenocarcinoma out of esophageal carcinomas among Japanese was only 1% - 2%, it is now increasing [2]. Spinal epidural metastasis occurs in 5% - 10% of all cancer patients. In particular, lung, breast, prostate, kidney, and lymphs are common as the primary site [9]. Spinal epidural metastasis of esophageal carcinoma is rare and the incident rate is about 1% [10-12]. Among metastatic tumors in the epidural space, approximately 60% are located in the thoracic spine and 30% are located in the lumbosacral spine [9]. To our knowledge, no cases of isolated epidural metastatic tumor without bone involvement from Barrett’s adenocarcinoma have been reported in the literature. Most metastatic epidural tumors arise in vertebral bodies or pedicles first, followed by invasion of the epidural space. An isolated epidural tumor without bone involvement might be caused by a direct hematogenous dissemination via radicular arteries or vertebral venous plexus from a primary site that was not apparent during the primary operation [4,13,14]. Good neurological recovery resulted after the tumor was resected en bloc and the patient was ambulatory again postoperatively. The prognosis of advanced Barrett’s adenocarcinoma is generally poor although a good prognosis is expected in early stage cases. The five-year survival rate for a patient without lymph node metastasis is 85.3%, whereas that with distant lymph node metastasis (stage 4) is 0% [1]. In this case, though the patient was died 13 months after the initial operation, there was no recurrence of spinal region. Therefore, epidural tumor resection was effective for maintaining his daily living
4. Conclusion
An isolated epidural metastatic tumor without bone involvement is rare and thought to be caused by a direct hematogenous dissemination via radicular arteries or vertebral venous plexus from a primary site; indeed, metastatic para-aortic lymph nodes were observed during the first operation, and the patient was categorized as stage 4 according to the TNM stage classification. In this case of isolated metastatic epidural tumor from Barrett’s adenocarcinoma, no adhesion around the tumor was observed and it was easily excised en bloc, therefore good neurological recovery should be obtained postoperatively.