Survival Analysis of Victims of Sulfur Oxide Air Pollution Suffering from COPD or Asthma in Yokkaichi, Japan, in Relation to Predisposing Exposure ()
1. Introduction
Yokkaichi, Mie Prefecture, is an industrial city that faces Ise Bay on the Pacific Ocean side of the Japanese archipelago. A petroleum complex was built and began operating in 1957, using crude oil with a high sulfur content (more than 3%). The annual sulfur dioxide (SO2) emission level exceeded 100,000 tons, which caused air pollution with an increased concentration of sulfur oxides, as high as 1 ppm in polluted areas. By the early 1960s, the incidence of respiratory diseases, such as bronchial asthma, chronic bronchitis, and pulmonary emphysema, increased among people living in the vicinity of the complex. This resulted in increased mortality from these diseases. The adverse health effects of air pollution subsequently became a major health problem in Japan that was known as “Yokkaichi Asthma” (Yokkaichi Zensoku, in Japanese). A series of counter measures based on an area-wide total emission control system were put in place in 1972, which were resulted from a lawsuit in the Yokkaichi Court brought by inhabitants of Yokkaichi against six companies for reparation for health damage caused by air pollution. Following this, sulfur oxide air pollution in the region was markedly reduced, and reached the same level as that in un-polluted areas by the end of the 1970s. The atmospheric SO2 level is now below 0.01 ppm in the Yokkaichi area [1]. Mortality due to bronchial asthma decreased immediately after improvement of pollution, whereas mortality from chronic bronchitis decreased to the levels of control areas 4 to 5 years after the SO2 concentration was reduced to the ambient air standard [2-12].
Recently, we published a report regarding the mortality and life expectancy of patients with Yokkaichi Asthma [13]. This revealed that the 1975-2000 mortality rates for chronic obstructive pulmonary disease (COPD, chronic bronchitis and pulmonary emphysema) and asthma in Yokkaichi patients were significantly higher than those in the whole Mie Prefecture population. Yokkaichi patients showed a shorter life expectancy than the whole Mie Prefecture population, reflecting high mortality rates in patients from Yokkaichi. The potential gains in life expectancy were greater in patients from Yokkaichi than in the Mie Prefecture general population when death from respiratory diseases was excluded. The excess gains of Yokkaichi patients reached approximately half of the difference in life expectancy between Yokkaichi patients and the Mie Prefecture population, suggesting that the decreased life expectancy was largely due to respiratory mortality. Thus, delayed adverse health effects persisted among victims despite reductions in air pollution, although no new cases of COPD or asthma due to air pollution have been reported since 1988.
COPD is a leading cause of death worldwide. Factors that predict outcomes in patients with COPD are reported to be age [14,15], smoking status [15,16], body mass index (BMI) [17-19], vital capacity percent predicted (%VC) [20], forced expiratory volume 1.0 (sec) % (expressed as FEV1% predicted, FEV1/FVC%, or volume) [15,18,21], clinical symptoms such as shortness of breath (dyspnea) [22], cough and sputum [14,21,23,24], and asthma attack [25]. Recently, Celli et al. [18] constructed the BODE index using BMI, airflow obstruction, dyspnea and exercise capacity index (measured by the sixminute-walk test) to predict the risk of death in patients with COPD. Asthma is another condition characterized by decreased lung function that is associated with increased mortality [26]. The risk of subsequent death from asthma has been reported to increase with the presence of reduced FEV1, advanced age, and lifetime tobacco consumption [27]. However, Nishimura et al. [28] reported that the level of dyspnea has a more significant effect on survival than disease severity based on FEV1 in patients with COPD. Regarding long-term outcomes in relation to initial clinical parameters, however, few epidemiological studies have been conducted. A study by Vandentorren et al. [16], a 25-year follow-up of a large sample of the French adult population, suggested an excess mortality in asthmatic individuals that was particularly due to COPD. Hospers et al. [25] reported asthma attacks with predicted mortality from COPD the general population.
It has been observed that chronic exposure to outdoor SO2 air pollution is associated with decreased pulmonary function in asthmatic and adult populations [29,30]. Significant positive associations were observed between chronic volcanic SO2 exposure and increased prevalence of cough and phlegm, wheezing and bronchitis [31].
Bronchitis-like symptoms such as cough and phlegm were correlated with 3-year proximity SO2 pollution levels in individuals aged 65 years or older [32]. Asthma severity in adults is reported to be associated with concurrent SO2 air pollution [33]. In the present study, therefore, we investigated the relationships of survival of patients with Yokkaichi Asthma to initial clinical findings and symptoms (at the medical check-up just prior to registration) and predisposing exposure to ambient SO2, based on 35 years of follow-up.
2. Subjects and Methods
2.1. Subjects
Records of 1836 patients registered in Yokkaichi during 1973-1988 by “Pollution-Related Health Damage Compensation Law (1973)” were used in this study with the authorization of the Yokkaichi Public Office. Disease diagnosis was made based on clinical signs and symptoms and laboratory findings such as chest X-ray, arterial blood oxygen tension and lung function in each hospital/ clinic that the patients attended (registration for compensation by the City Office was performed approximately one month later, based on the patient application). In total, 467 subjects younger than 20 years were excluded from the study because they lacked pulmonary function data. Among the remaining subjects, data until December 31, 2007, were available for 1045 subjects. Complete records were obtained from 735 patients (352 males and 383 females) and were used for the analysis.
2.2. Symptoms and Pulmonary Function Data
The day when the diagnosis was made was regarded as the start of observation for the present study. Data obtained were sex, age (months), BMI, %VC, FEV1%, smoking status, clinical symptoms (dyspnea, asthma attack, cough and sputum) and clinical diagnosis at the start of observation, and observation period (months). Smoking status at the end of observation was also included. Smoking status was scored as 0 (never smoked), 1 (ex-smoker) or 2 (smoker). Each clinical symptom had been scored from 1 (slight) to 5 (most severe) by attending physicians.
2.3. Estimation of Predisposing Exposure to Ambient SO2
Monthly average ambient air SO2 concentration for the Yokkaichi area since 1970 was obtained from the Environmental Numeric Database of the National Institute for Environmental Science, Japan [35]. Data for the polluted area (Isozu, Shiohama and Kusu districts) during the period between April 1970 and the start of observation (see above) were then averaged for each subject and used as his/her predisposing exposure to ambient SO2.
2.4. Statistical Analysis
Correlation analysis was performed to assess the relationship between predisposing exposure to SO2 and all baseline variables, i.e. sex, age (months), BMI, %VC, FEV1%, smoking status and clinical symptoms (dyspnea, asthma attack, cough and sputum).
The survival of all patients was analyzed using the Kaplan-Meier method. Survival between primary diagnoses (COPD vs. asthma) was compared by the log-rank test. A Cox proportional hazards analysis was performed to assess the relationship between survival and all baseline variables, smoking status at the end of observation and predisposing exposure to SO2.
3. Results
Figure 1 shows monthly average ambient air SO2 concentration during 1970-1988. The clinical diagnosis of 735 patients is presented in Table 1. Their demographic variables by primary diagnosis are presented in Tables 2 and 3, for male and female subjects, respectively.
Table 4 presents correlation coefficients between predisposing SO2 exposure, pulmonary function and clinical symptoms. Severity of clinical symptoms was correlated with predisposing exposure in both males and females. Pulmonary function data were inversely correlated with predisposing exposure in females. Figure 2 illustrates Kaplan-Meier survival curves for 735 subjects; in addition, results for all 1045 patients are shown. For both groups, survival rates were significantly higher in asthma classes for both males and females. Table 5 presents the results of the Cox proportional hazards analysis. The model revealed that in males, mortality was significantly associated with age, %VC, FEV1%, and smoking status at the end of observation, cough and sputum. In females, mortality was significantly associated with age, FEV1% and smoking status at the end of observation.
4. Discussion
The present study indicated that among all patients (COPD and asthma), age, FEV1% and smoking affected mortality for both males and females. Cough and sputum, as well as %VC also affected the survival of male subjects. Severity of clinical symptoms and decreased pulmonary function were significantly correlated with predisposing SO2 exposure, suggesting that changes in respiratory system function caused by air pollution affected the survival of patients. These significant correlations
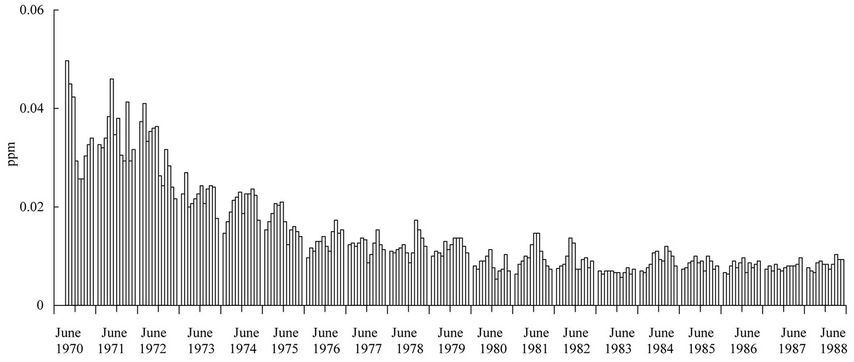
Figure 1. Monthly average ambient air SO2 concentration during 1970-1988 in the Yokkaichi area (Isozu, Shiohama and Kusu districts).
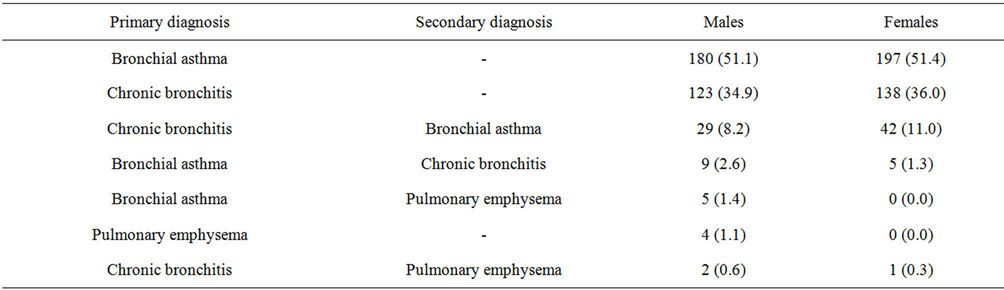
Table 1. Clinical diagnosis of 735 patients (352 males and 383 females), n (%).
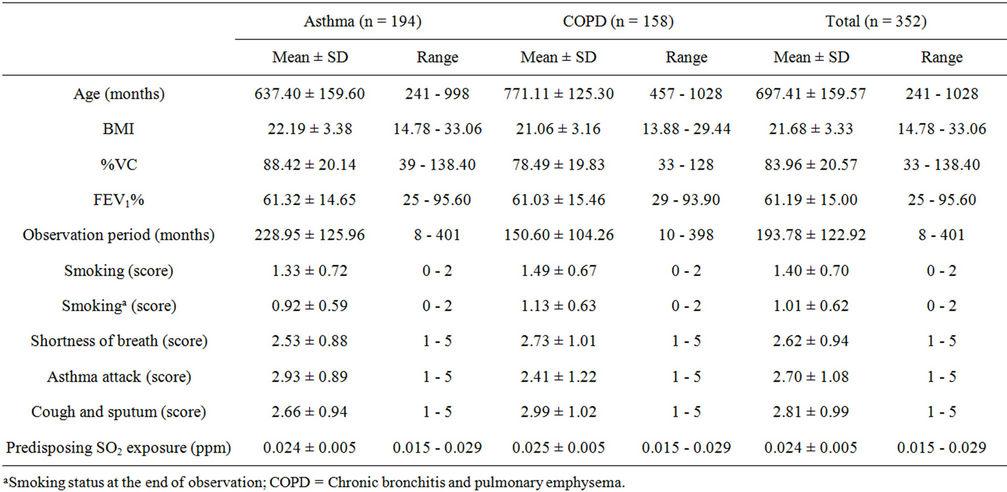
Table 2. Characteristics of 352 male subjects, by primary diagnosis.
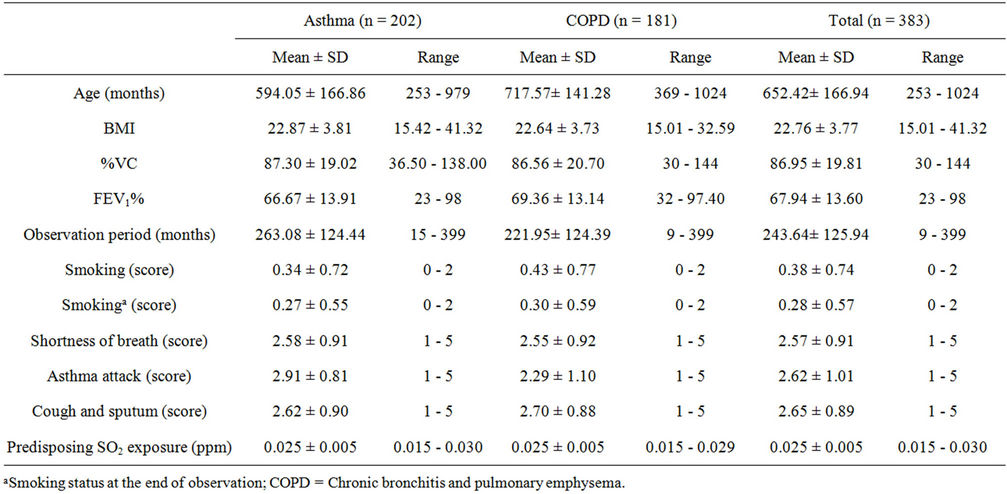
Table 3. Characteristics of 383 female subjects, by primary diagnosis.
essentially agree with previous observations of a significant association between SO2 exposure and changes in pulmonary function and/or clinical respiratory symptoms [29-33].
In the present study, a significant association between pulmonary function data and predisposing SO2 exposure was observed for both males and females, whereas the severity of clinical symptoms was significantly associated with exposure only in females. This agrees with a previous report [32], where a more pronounced effect of SO2 on cough and phlegm was observed in females than in males. It has been reported that chronic cough and sputum production were associated with premature death in patients with COPD [14,21,23,24]. In the present study, there was a significant association between cough and sputum and mortality in males, but not in females. Because Lange et al. [14] reported that chronic mucus hypersecretion (cough and sputum lasting at least three
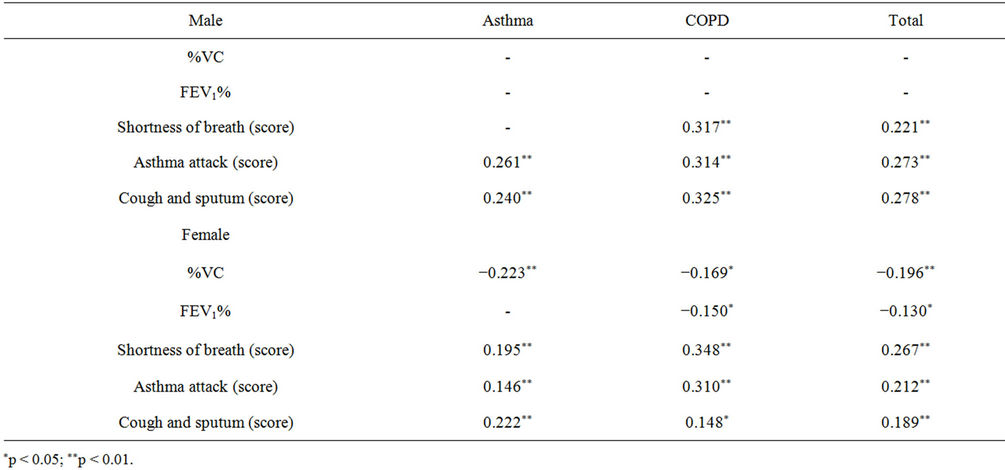
Table 4. Significant correlation coefficients between predisposing SO2 exposure, pulmonary function and clinical symptoms, by primary diagnosis.
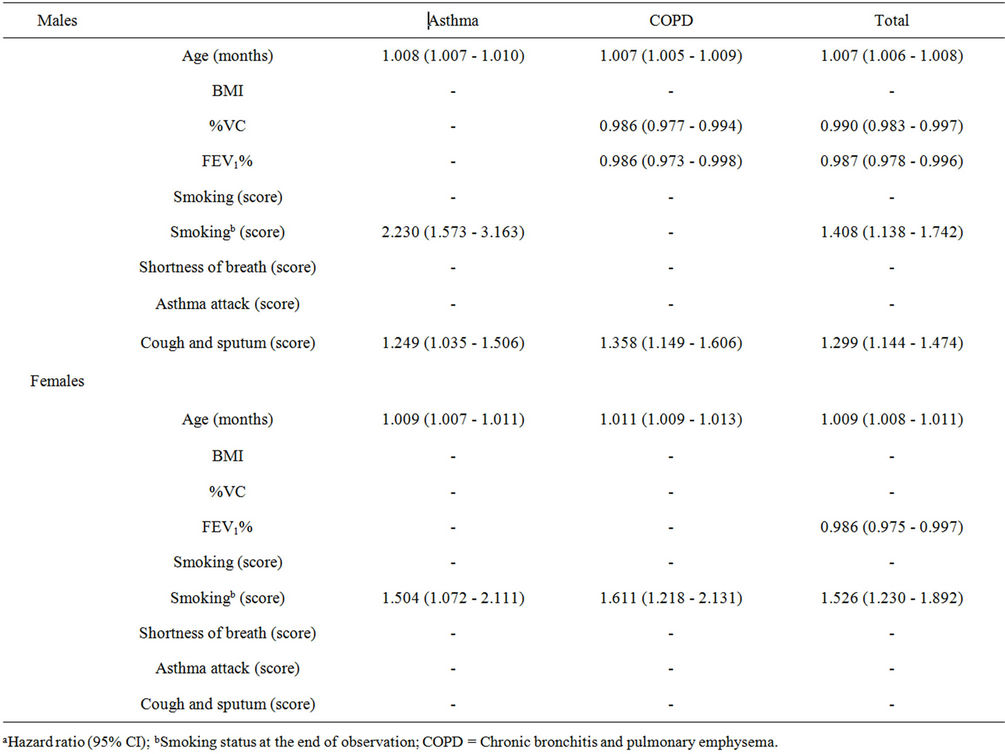
Table 5. Multivariate Cox proportional hazards analysis of parameters associated with mortality, by primary diagnosisa.
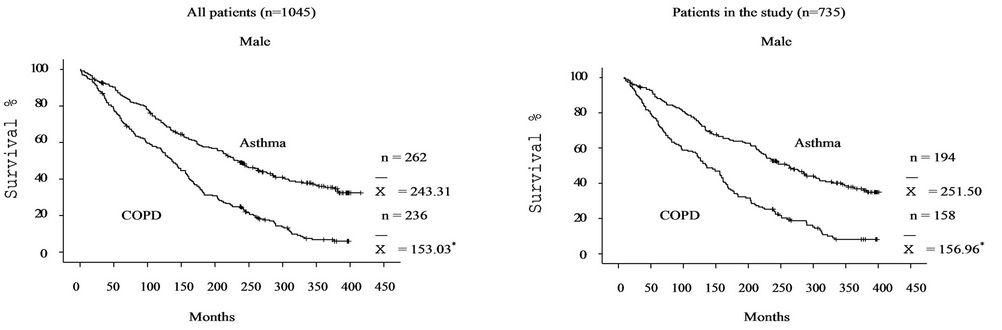
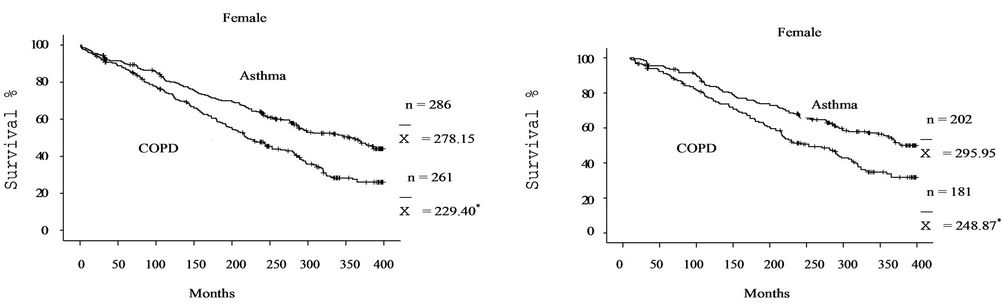
Figure 2. Survival rates by primary diagnosis (asthma or COPD) for all 1045 patients and 735 subjects analyzed in the present study.  = mean survival (months). *p < 0.05 compared with asthma by log-rank test.
= mean survival (months). *p < 0.05 compared with asthma by log-rank test.
months a year) was significantly associated with death from all causes in males with COPD, mucosal changes in the lung seem a potent risk for death in males. The underlying mechanisms behind these sex differences should be further studied.
Pulmonary function is believed to be the most important predictor of mortality [35]. For example, a decrease in FEV1% increased the risk of death in patients with COPD [21]. In the present study, a significant association between mortality and FEV1% was observed in both males and females (Table 5), suggesting that spared pulmonary function extended their survival. Similarly, a significant association between mortality and FEV1% was observed in males with COPD. However, the severity of cough and sputum showed more potent effects on mortality than FEV1%. This may agree with a report by Guerra et al. [36] that chronic bronchitis (cough and sputum production) unaccompanied by airflow limitation (FEV1% < 70%) [37,38] was an early marker of allcause mortality.
Gunen et al. [19] reported that the duration of disease was strongly related to mortality. Kawakami et al. [39] reported comparisons between %VC of COPD survivors and nonsurvivors; survivors had high %VC values. In the present study, a significant association between mortality and %VC was observed in all male patients (COPD and asthma) (Table 4), suggesting that spared pulmonary function extended their survival. In contrast, no significant association between mortality and %VC was observed in females. This is probably because %VC in males (mean 83.96) was lower than that in females (mean 86.95). Similarly, a significant association between mortality and %VC was observed male patients with COPD, who showed the lowest %VC values (mean 78.49).
In the present study, smoking was significantly associated with mortality in both males and females, in agreement with other studies [21,25]. Mortality for males in the present study was simultaneously affected by FEV1% and smoking. According to previous prevalence studies [40], airflow obstruction will eventually develop in 10% to 20% of all smokers. Smoking may induce the process that accelerates airflow obstruction, and thus increase mortality [41].
Mortality increases with age in patients with obstructive pulmonary disease [14]. Gunen et al. [19] reported that the duration of disease was strongly related to mortality. These observations may explain the finding of a significant association between mortality and age in the middle and high age classes for males and females. In the present study, only data on symptoms and pulmonary function among Yokkaichi patients were available. Therefore, the Kaplan-Meier analysis could not compare survival curves between Yokkaichi patients and cases of COPD or asthma which were not due to air pollution during the same period. The risk factors for COPD in the developed world are occupational or environmental exposure to dust, gas, vapor or fumes [42], malnutrition [43], socioeconomic status and lifestyle [35] and increased airway responsiveness [44]. The effects of these risk factors on the patients should be evaluated in further studies.
5. Conclusion
The survival of patients with Yokkaichi Asthma was affected by severity of clinical symptoms and decreased pulmonary function, which were related to predisposing SO2 exposure. It appeared that the effects of clinical changes were greater in males than in females.
6. Acknowledgements
The study was supported by the Conference on Medical Care and Research for Environmental Pollution, Mie Prefecture, Japan.
NOTES