Ocular Manifestations in HIV Positive and AIDS Patients in Nepal ()
1. Introduction
Human immunodeficiency virus (HIV) is a lentivirus (a member of the retrovirus family) that causes acquired immunodeficiency syndrome (AIDS), [1,2] a condition in humans in which progressive failure of the immune system allows life-threatening opportunistic infections and cancers to thrive. Infection with HIV occurs by the transfer of blood, semen, vaginal fluid, pre-ejaculate, or breast milk. Within these bodily fluids, HIV is present as both free virus particles and virus within infected immune cells. The four major routes of transmission are unsafe sex, contaminated needles, breast milk, and transmission from an infected mother to her baby at birth (vertical transmission). Screening of blood products for HIV has largely eliminated transmission through blood transfusions or infected blood products in the developed world. HIV-infected person is diagnosed with AIDS when his or her immune system is seriously compromised and manifestations of HIV infection are severe. The Centers for Disease Control (CDC) in the USA extended the definition of AIDS to include all those persons who are severely immunosuppressed (CD4+ T cell count < 200/cu mm) irrespective of the presence or the absence of the indicator of disease [3].
The total number of HIV patients in the world was estimated 33.4 million [31.1 - 35.8 million] in 2008. [4] In Nepal, as of November 2007, a total of 10,369 cases of HIV, 1578 AIDS cases and 423 AIDS deaths had been reported to the National Centre for AIDS and STD control (NCASC) [5]. But it is only the tip of the iceberg, the estimated number in Nepal as reported by UNAIDS is 75,000 [6].
HIV has the capability to affect every organ system in the body by direct damage by the virus or by rendering the host susceptible to opportunistic infections. Ocular manifestations have been reported in up to 70% of individuals infected with HIV and it has become apparent that the ocular manifestations almost invariably reflect systemic disease and may be the first sign of disseminated infection in many cases [5]. Several publications have described the ocular manifestations of the HIV/ AIDS [6-19]. Most of the studies on the prevalence of ocular complications in HIV/AIDS have been carried out in industrialized countries [20]. In contrast, more than 90% of all HIV sufferers live in the developing world [6]. Furthermore, there is strong evidence that both ocular complications and their prevalence differ substantially between developing and industrialized countries [20].
Ocular manifestations in HIV positive and AIDS patients range from simple Blepharitis to severe blinding conditions like CMV retinitis. As HIV is an illness that interferes with the immune system making people with AIDS much more likely to get infections, including opportunistic infections and tumors that do not affect people with working immune systems.
Ocular complications if detected at an early stage and managed properly, can be helpful to prevent or minimize potential visual damage.
Ocular complications are common, affecting 50% to 75% of all such patients at some point during the course of their illness. Cytomegalovirus retinitis is by far the most frequent cause of vision loss in patients with AIDS. Although the prevalence of cytomegalovirus retinitis is decreasing in industrialized countries because of the widespread availability of highly active antiretroviral therapy, between 10% and 20% of HIV-infected patients worldwide can be expected to lose vision in one or both eyes as a result of ocular cytomegalovirus infection. Less frequent but important causes of bilateral vision loss in patients with HIV/AIDS include varicella zoster virus and herpes simplex virus retinitis, HIV-related ischaemic microvasculopathy, ocular syphilis, ocular tuberculosis, cryptococcal meningitis, and ocular toxic or allergic drug reactions [21].
Till date, to our best of knowledge, there have been no published documents or studies indicating the ocular manifestation of HIV/AIDS from Nepal. Hence, this study has been undertaken to identify the ocular manifestations in HIV/AIDS in Nepalese population.
2. Material and Methods
A cross sectional study was carried out during the period of January 2008 to July 2009. All diagnosed cases of HIV infected individuals either coming to the Tribhuan University Teaching Hospital (the tertiary center) or collected from three rehabilitation centres in Kathmandu were included in the study. Written and verbal consent were obtained from the patients or their guardians. Detailed demographic profile of the patients including age, gender, ethnic group and duration of HIV infection diagnosed were undertaken. Detailed history was asked including history of receiving antiretroviral therapy, risk factor for the transmission of HIV.
Staging of disease was done according to revised WHO clinical staging of HIV as given in Table 1 [22].
Number of recent CD4 count was also noted. The severity of ocular manifestations was correlated with the number of CD4 count. Detailed ocular examination was carried out. Ocular examination included visual acuity assessment, ocular motility assessment, eyelid and adnexal examination, conjunctival and scleral examination, examination of cornea, anterior and posterior segment evaluation.
Visual acuity was noted by Snellen chart and was recorded in snellen fraction. Ocular motility was tested with torch light in cardinal gazes. Detailed orthoptics examination including Hess charting and diplopia charting were also carried out in suspected case of muscle
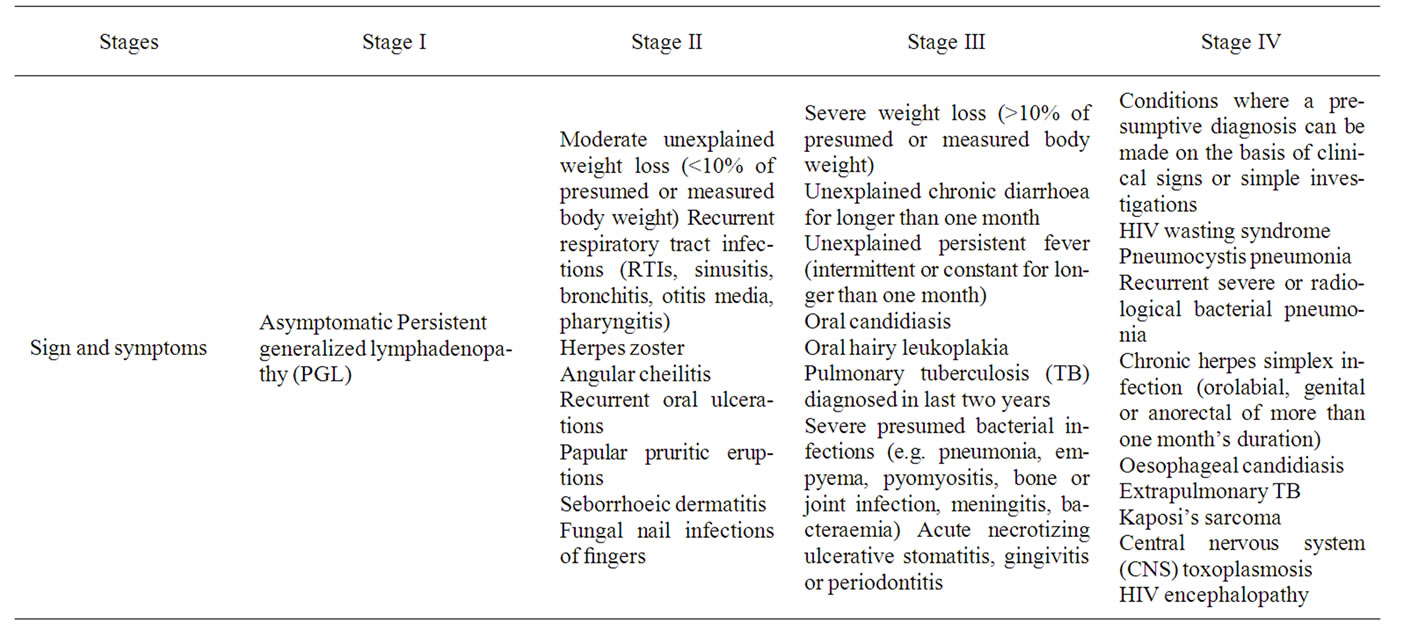
Table 1. Revised who clinical staging of HIV/AIDS for adults and adolescents.
palsy. Findings in eyelid, orbital and peri-orbital region was recorded and documented schematically. Conjunctiva, sclera and episclera were examined for any abnormalities and were documented. Cornea was examined for any defect, infiltrates and sensitivity. Anterior chamber finding was recorded. Cells, flare grading was done [13]. Posterior segment examination included vitreous and retinal examination. Vitreous cells and flares were also graded according to their severity [14]. Detail Fundus examinations under mydriasis were performed with Heine Beta 200 direct ophthalmoscope, binocular indirect ophthalmoscope with +20 D lens and Haag Streit 900 slit Lamp with +90 D Lens. Intra ocular pressure (IOP) was measured by non contact air Puff tonometer.
Data were collected in a proforma prepared for the study and the data were tabulated and analyzed in spss13. Mean, standard deviation, Pearson’s correlation coefficient were used as descriptive statistical tool and chisquare, ANOVA and paired t-tests were used as inferential statistical tool.
3. Results
A total of 103 patients were included in the study. 54.4% of patients were from hospital and 45.6% were from rehabilitation Centre. The mean age of the presentation was 29.6 ± 9.8 years. 81.5% of the total patients were in the age group 21 to 40 years (73.84% - 89.15%, CI-95%). 71 (68.9%) were male and 32 (31.1%) were female, with a ratio of 2.2:1.
Table 2 shows the patient distribution according to the visual acuity at presentation. 94.2% of the patients had visual acuity of 6/6 to 6/18 in each eye.
40 patients (38.8%) had ocular involvement. 35.2% of total male patients and 46.8% of the total female patients had ocular involvement. Out of 103 patients, 79 (76.7%) patients were asymptomatic. 87.5% the symptomatic group of patients had ocular involvement. Even in the asymptomatic group, 24% had ocular morbidity.
60 cases (58.3%) of the total patients had undergone the CD4 count investigation. 27 (45%) had count in the range 51 to 199. There were 13 patients (21.7%) with range 200 to 500 and 10 patients each in ≥500 and ≤50. There was a statistically significant, strong negative correlation between ocular involvement and CD4 count (r = –0.51, p = 0.00003).
Figure 1 shows that the ocular involvement in heterosexual mode was more than in intravenous drug users (IDU). There was no ocular involvement seen vertically transmitted cases. The association between mode of transmission and ocular involvement was statistically signifycant (p = 0.023).
Ocular involvement was correlated with the WHO clinical stage of the disease. 50% ocular involvement was observed in Stage IV followed by 12.5% in Stage III and 11.5% in Stage I. No ocular involvement was seen in Stage II. There was not statistically significant correlation between the clinical staging of the disease and the ocular involvement (p = 0.1, chi square test).
Table 2 shows the form of ocular disorder in symptomatic and asymptomatic patients. The table shows that even in those asymptomatic patients in 19 out of 79 patients accounting 22.7%, ocular lesions were seen. The most common finding was HIV retinopathy seen in 33 eyes (20.8%) of 17 patients. In the symptomatic group also, the most common lesion was HIV retinopathy seen in 10 eyes (20.8%) of 7 patients, followed by conjunctivitis seen in 8 eyes (16.6%) of 4 patients and CMV retinitis seen in 5 eyes (10.4%) of 4 patients.
7.76% of the cases had Neuro-ophthalmic Lesions. 2 cases (1.9%) had papilloedema, 1 case of retrobulbar optic neuritis, 2 cases of optic atrophy associated with retinal degeneration. 3 cases (2.9%) had cranial nerve palsy; one cases each of CN III with papillary sparing, CN VI and CN VII palsy.
Figure 2 shows among the total 48 ocular findings seen in 103 patients; HIV retinopathy was the most common accounting for 50% of the total ocular findings followed by CMV retinitis and Conjunctivitis each accounting for 8.3%.