The effect of self-employment on health, access to care, and health behavior ()
1. INTRODUCTION
Based on the amount of money that is spent on health services in the US, one might assume that access to health care services and the quality of health services are the primary drivers of health. Although these factors do play a role, federal and local policies, social and physical conditions of the environment, and biology and genetics must also be considered. Moreover, individual behavior or what is sometimes referred to as “lifestyle” has been shown by many researchers to be one of the most important determinants of health [1].
The term “lifestyle” is a catch-all term that typically refers to behaviors such as smoking, diet, drug use, exercise, and even sleep. In this paper, we empirically examine the role of self-employment, conceptualized as a lifestyle factor, on health. The daily rhythm and financial expectations of self-employed individuals is very different from that of wage earners. While wage-earning individuals have the benefit of consistent earnings, being self-employed can give individuals greater work autonomy, flexibility, and the expectation of higher financial rewards [2]. These general features may explain higher job and life satisfaction among the self-employed compared to wage-earners [2-6].
Theoretically, self-employed individuals may experience better health due to the positive association between health and life satisfaction (Binder and Coad, 2010). On the other hand, self-employed individuals face more demands regarding operating their own business (e.g., longer work hours, more decision-making responsibility and stress attributable to market uncertainty). The potential financial, physical and mental stressors among the self-employed can lead to more physical and mental health problems [7].
This study has two primary goals. The first is to investigate health difference (both physical and mental) between the self-employed and wage-earning populations. We analyze a nationally representative sample of US working adults. Instrumental variables approaches are utilized to deal with the fact that employment choice may affect health, and vice versa (i.e., endogeneity of selfemployment). Prior research does not account for this important selection issue [5]. To increase the richness of the study, we use both perceived measures and validated indexes of physical and mental health as well as a set of clinical conditions of physical health.
The second goal of the study is to explore potential explanations for health difference (or no difference in health) between the two populations. We test whether, after accounting for the self-selection issue, self-employment is associated with unequal access to health care or different health-related behavior.
The contemporary US represents an interesting site for a test of the potential pathways through which self-employment may influence health. In the US, self-employment has been linked to a significantly greater risk of being uninsured as compared to wage-earning [8-10]: the self-employed are currently twice as likely as wageearning individuals to be uninsured [9]. In this circumstance, self-employment might relate to worse health outcomes if the lack of health insurance among the selfemployed hampers them from obtaining access to health care at the time of need. Meanwhile, certain job characteristics unique to self-employment such as greater autonomy and flexibility might be attached to health behaviors different from those of wage-earners.
The Affordable Care Act of 2010 and the Supreme Court’s decision in June 2012 in the US will alter the health insurance landscape significantly beginning in January 2014 [11]. Having a clear sense of the health disparities and role of health insurance and health behavior on health production is essential to understand how far the Affordable Care Act can go in terms of reducing health disparities between wage earners and the self-employed.
2. RELATIONSHIP BETWEEN SELF-EMPLOYMENT AND HEALTH
The literature remains inconclusive about a link between self-employment and health, showing substantial within and cross-country variations. Swedish self-employed individuals have more mental health conditions than wage-earners [5]. Israeli self-employed workers experience greater work-related stress than wage-earners [12]. In Germany, the self-employed reportedly have fewer mental health problems [13]. Similarly, analyses of data on workers in the US and European countries find a significant association between self-employment and greater job and life satisfaction [2,4,6,14]. In Canada, no difference in mental health is found between self-employed and wage-earning individuals [15].
There is no clear-cut pattern as well in terms of physical health differences. In Sweden, there is no difference in reported general health status between the self-employed and wage-earners [5]. German self-employed workers are physically healthier, e.g., lower blood pressure and less hypertension cases [13]. Self-employed males in Israel appear to be physically unhealthier than their wageearning counterparts [12].
Little research has examined a relationship between self-employment and health in the US. Dolinsky and Caputo [16] find that among female workers, self-employed persons report worse subjective health than their wage-earning counterparts. Perry and Rosen [17] is particularly noteworthy. They analyze a nationally representative sample of US working adults in 1996 to investigate difference between self-employed and wage-earners in term of health insurance coverage and health status. They report that despite the significant lack of health insurance among the self-employed, no difference in health status is found between the two groups as measured by general health perception and several medical conditions such as cancer, heart disease, and respiratory condition.
Despite the contributions to the literature, several limitations in the literature make it difficult to conclude that self-employment does or does not relate to health disparity in the contemporaneous US.
First, findings from the international data on health differential between self-employed and wage-earning individuals cannot be easily applicable to the US due to cross country differences.
Second, most existing studies are cross-sectional in nature, and therefore their findings are likely to be limited in terms of causal inference. In particular, the potential omitted variable bias and reverse causality from health status to employment choice are not directly addressed. For instance, Perry and Rosen [17] finding might be due to “self-selection” into self-employment by healthy persons, which could occur when healthier persons are more likely to choose self-employment rather than to work for others.
Third, results from the US-based studies may not be applicable to today’s state of affairs. During the last decades, minorities and women’s participation in the selfemployment workforce have increased significantly [18]. Given that health disparities by race/ethnicity and gender continue to exist, the demographic changes in the selfemployed population might signal a new era of health disparities between the self-employed and wage-earning populations.
Fourth, self-employed persons in the US may obtain equal access to necessary health care services through self-insurance despite their lack of health insurance [19]. In this scenario, an employment status (i.e., self-employment vs. wage-earning) may not lead to any health difference as long as the lack of health insurance does not worsen access to health care among the self-employed. Alternatively, self-employed individuals may be more likely than wage-earning counterparts to engage in health behavior perhaps due to more flexibility and autonomy of self-employment.
This study addresses the limitations in the literature, employing a method that directly corrects for the simultaneity of self-employment and health, and also testing for unmet health care need and health behavior as mechanisms that link self-employment and health.
3. DATA
3.1. Sample
The sample for this study is derived from the household component of the 2007 Medical Expenditure Panel Survey (MEPS). The MEPS is a nationally representative survey of the US civilian non-institutionalized population, and provides rich information on health status, medical conditions, employment, health insurance coverage, and socio-demographic characteristics of respondents. The MEPS uses a complex survey design that features stratified and multi-stage sampling and the oversampling of certain groups such as minorities and lowincome families. Respondents were preliminarily interviewed in the beginning of 2007 (Round 1). Two followup interviews (Rounds 2 and 3 interviews) were conducted during calendar year 2007. All information is derived from the Round 2 interview unless mentioned otherwise.
The original sample contains 30,964 individuals. The elderly aged 65 and over and children under 18 are excluded from the analysis which deletes 13,369 observations. We drop from the sample 4037 unemployed individuals and 123 individuals who provided no information on employment status. The final analytic sample includes 13,435 individuals, either self-employed or wage-earning individuals.
3.2. Measures of Physical and Mental Health
Variables used in this study are reported in Table 1. We discuss their descriptive statistics in the result section.
Measures for physical and mental health include both health perception and validated scores, as well as a set of medical conditions. Health perception measures include perceived physical health status and perceived mental health status. Both variables take the ordinal values from 1 (poor health) to 5 (excellent health). Validated physical health indexes include the Physical Health Composite Scores derived from the Short-Form 12 Version 2 (SF- 12v2). We also examine a set of prevalent life-threatening or chronic medical conditions such as stroke, diabetes, asthma, high blood pressure, high cholesterol, emphysema, joint pain, and arthritis. Validated mental health measures include the Mental Health Composite Scores calculated from the SF-12v2, and the Kessler Index of non-specific psychological distress. Physical Health Composite Scores, Mental Health Composite Scores, and Kessler Index are derived from the Round 2 interview while other health outcomes are obtained from the Round 3 interview.
The SF-12v2 is a short form survey with 12 questions selected from the SF-36 Health Survey [20]. It is a valid shorter alternative to the SF-36. Responses to 12 health questions are combined and weighted to create two scales that provide easily interpretable scores for physical and mental health. Physical Health Composite Score is calculated by weighting the physical items of the SF-12v2 more heavily while Mental Health Composite Score is calculated by weighting the mental responses to the SF-12v2 more heavily. Both Physical Health Composite Scores and Mental Health Composite Scores range from 0 to 100. Although Physical Health Composite Scores and Mental Health Composite Scores may not have very intuitive meaning, higher scores reflect higher levels of health (i.e., better health). The Kessler Index is a summary measure of 6 questions intended to measure the level of non-specific psychological distress. Greater K6 scores reflect lower levels of mental health (i.e., worse mental health). We use the natural logarithms of Physical Health Composite Scores, Mental Health Composite Scores, and Kessler Index to mitigate skewed distribution.
3.3. Access to Care and Health Behavior
Access-to-care outcomes are binary variables indicating whether a person experienced a barrier to obtaining necessary health care services including being unable to get necessary medical care, being delayed in getting necessary medical care, being unable to get necessary dental care, being delayed in getting necessary dental care, being unable to get necessary prescribed medication, and being delayed in getting necessary prescribed medication.
Health behavior outcomes include binary indicators for whether a person currently smoke, whether a person currently engages in moderate or vigorous physical activity for a half hour or more at least three times a week, and whether a person’s body mass index (BMI) falls within the normal weight range (i.e., 18.5 ≤ BMI < 25) as a crude proxy for general health behavior.
3.4. Self-Employment
The binary indicator of self-employment status (SelfEmp) is our main explanatory variable. It takes the value of 1 if a respondent was self-employed and 0 if a respondent was employed as a wage-earning individual.
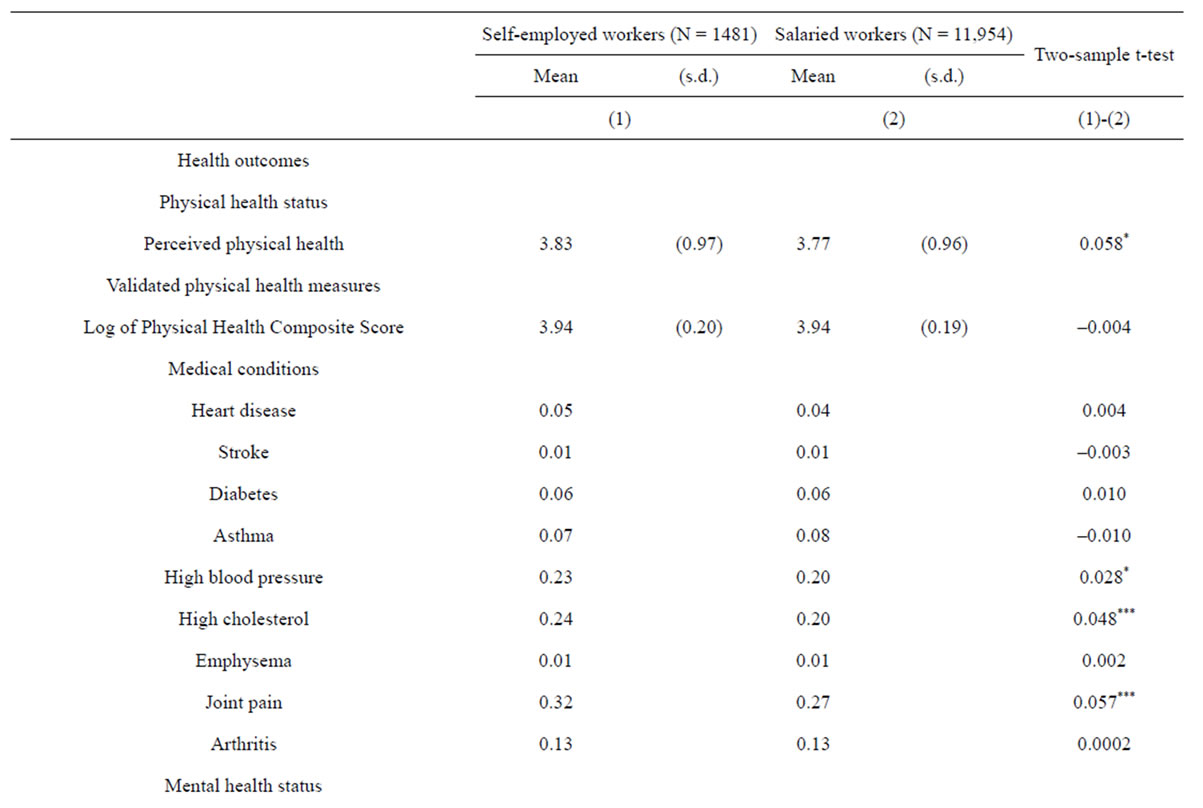
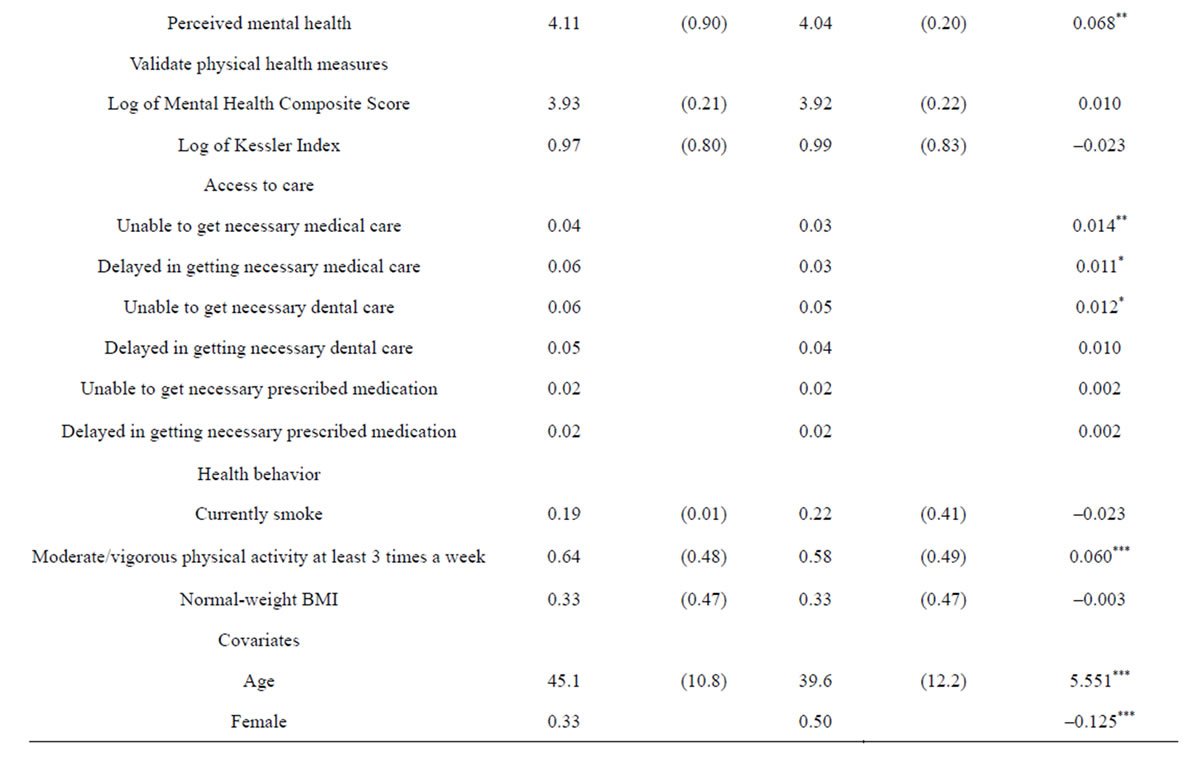
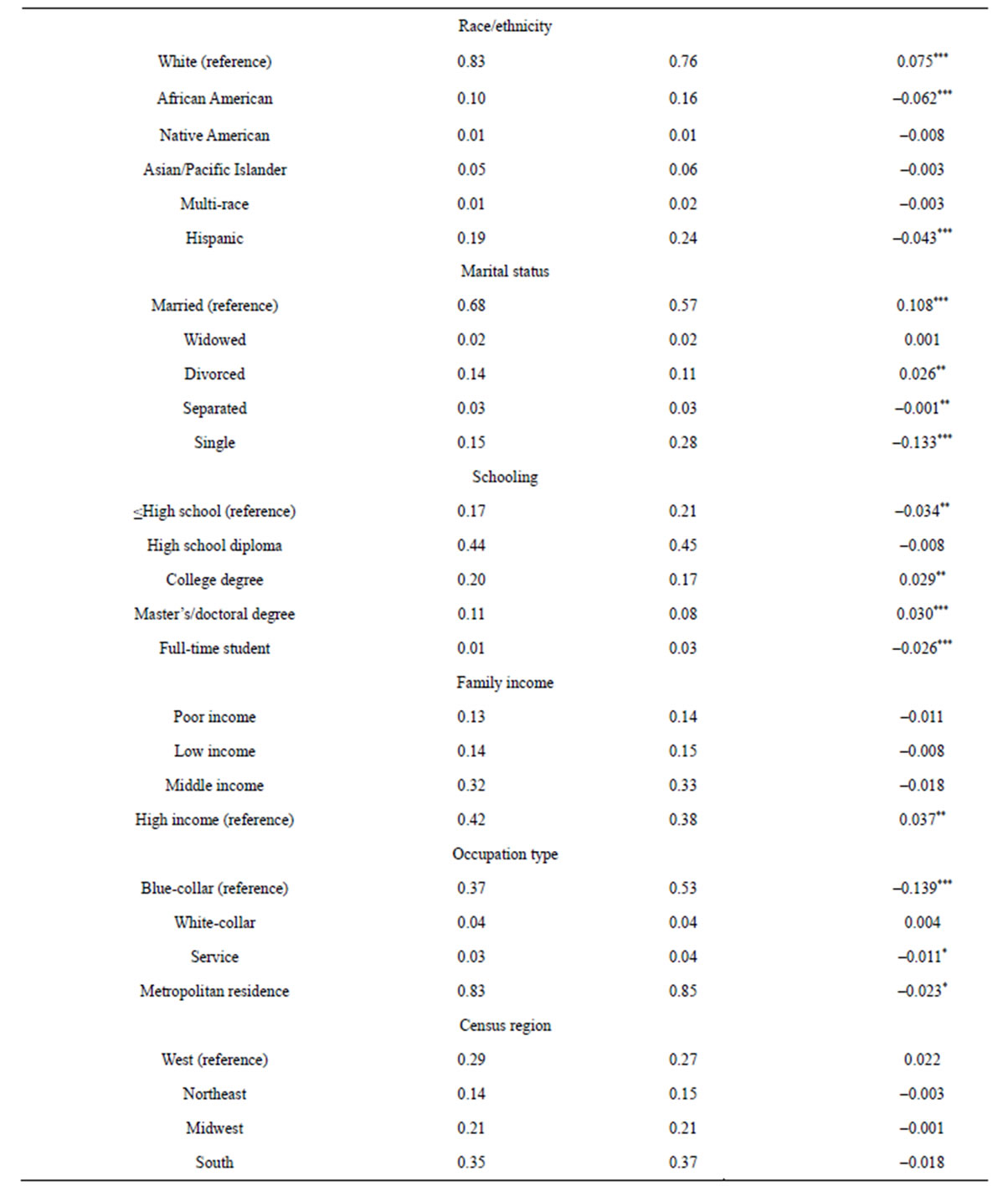
Table 1. Descriptive statistics by self-employment status (N = 13,435).
s.d. = standard deviation. Family income levels are classified into four categories based on 2007 federal poverty level (FPL): poor income (less than 125% FPL), low income (125% to less than 200% FPL), middle income (200% to less than 400% FPL), and high income (greater than or equal to 400% FPL). White-collar occupations include management, business, financial operation, and professional and related occupations. *p < 0.05; **p < 0.01; ***p < 0.001.
There were 1481 self-employed persons (11 percent of the unweighted sample) in 2007.
3.5. Control Variables
We control for demographic and socio-economic variables that may be correlated with our main independent and outcome variables. Covariates include age, female, race/ethnicity (African-American, Native American, Asian/ Pacific Islander, Multi-race, and Hispanic; white as a reference), marital status (widowed, divorced, separated, and single; married as a reference), level of schooling (high school graduate, college diploma, and master’s or doctoral degree; less than high school as a reference), full-time student status, family income levels (poor, low, and middle income; high income as a reference), occupation type (white-collar and service job; blue-collar as a reference), metropolitan statistical area of residence, and geographic census regions (Northeast, Midwest, and South; West as a reference).
4. METHODS
4.1. Empirical Model
We estimate an empirical model of the following form:
 (1)
(1)
where i indexes an individual and  refers to the error term. Y includes the various health measures as well as the measures of access to care and health behavior. SE is the binary self-employment variable of main interest. X is a vector of covariates, discussed above.
refers to the error term. Y includes the various health measures as well as the measures of access to care and health behavior. SE is the binary self-employment variable of main interest. X is a vector of covariates, discussed above.
Since our dependent variables include both continuous and discrete measures, we take into account different function forms of the dependent variables when estimating Equation (1). For the continuous dependent variables such as ln (Physical Health Composite Scores), ln (Mental Health Composite Scores), and ln (Kessler Index), we obtain ordinary least squares (OLS) estimates. For the ordinal response variables such as perceived physical and mental health status, we estimate ordered logit models. Probit models are estimated for the binary medical condition variables as well as for the access-to-care and health behavior outcomes. All estimates are surveyweighted and adjusted for the complex design of the MEPS survey.
In a linear model such as an OLS model, the coefficient on the self-employment variable captures the marginal effect of self-employment on the outcomes. For non-linear models such as ordered logit and probit, we calculate the marginal effect of self-employment as a mean difference in predicted probabilities of the outcome between self-employed and wage-earning individuals [21,22]. We defer detailed discussion to the result section.
4.2. Endogenous Selection into Self-Employment
One complication in our empirical models is that selfemployment may be endogenous. This situation would arise if healthier individuals choose to be self-employed, rather than to become wage-earning individuals, or if there are unobserved individual profiles associated with both self-employment and health measures. This situation causes the self-employment variable to be correlated with the error term ( ), leading to biased and inconsistent estimates.
), leading to biased and inconsistent estimates.
To test and address the potential sources of bias, we carry out instrumental variables analyses. We obtain efficient two-step generalized method of moments (GMM) estimators for the continuous health variables. We obtain consistent two-stage residual inclusion (2SRI) estimators for the ordinal and binary health measures because the standard instrumental variables method may lead to inconsistent estimates in nonlinear models [23-25].
Instruments must meet two fundamental requirements. First, there must be a non-zero correlation between selfemployment and instruments. Second, instruments should not be correlated with the error terms in the above Equation (1). We reviewed the literature to find theoretically plausible instruments that meet the first condition. Our prospective instruments include the number of self-employed family members, a dichotomous immigrant status variable, years of labor market experience, the number of children, and having uninsured children. Having selfemployed family members increases the probability of entering self-employment possibly due to intra-household transfers of human capital [26,27]. Borjas [28] and Yuengert [29] report that the rate of self-employment is higher among immigrants than among US-born workers. Many older workers appear to transition from salaried work into self-employment before they complete retirement [26]. There appears a positive correlation between self-employment status and the number of children [30]. The high uninsurance rate of the self-employed may lead to a greater uninsurance for their children. Therefore, a dichotomous indicator for having uninsured children is included as a potential instrument.
We rigorously test whether the prospective instruments meet the above two criteria to become valid. We test the explanatory power of the instruments in the first stage equation using individual t-test and joint F-test. Staiger and Stock [31] recommend 10 or greater F statistic as evidence of strong instruments. The validity of the prospective instruments is further evaluated for the exclusion restrictions through the Hansen J statistic [32]. The J test evaluates the joint null hypothesis that instruments are uncorrelated with the error and thus are validly excluded from Equation (1). The J statistic from two-step GMM is used for the nonlinear models.
Table 2 presents a sample result of a first-stage regression. Having uninsured child and the number of selfemployed family members are used as valid instruments based on results of the diagnostic tests for the strength and validity of instruments. As shown, the instruments are highly, individually significant. Table 3 shows that in all models our instruments are jointly significant and validly excluded from the main equations.
5. RESULTS
5.1. Descriptive Results on the Relationship between Self-Employment and Health
Table 1 reports unweighted descriptive statistics for the outcomes and the covariates by self-employment status. Self-employment is significantly associated with a greater level of perceived physical health status. The two-sample t-test shows that the difference is statistically significant. The self-employed have a lower average Physical Health Composite Score than wage-earning individuals, but this difference was statistically insignificant. Although differences in various medical conditions are somewhat mixed, the descriptive statistics suggest that the self-employed have a greater probability of having high blood pressure, high cholesterol, and joint pain. In terms of mental health, self-employed individuals appear to have better perceived mental health. However, there is no statistically significant difference in clinically validated scores such as the Mental Health Composite Score and the Kessler Index of non-specific psychological distress.
Self-employed and wage-earning individuals also appear to be statistically different in other ways. The selfemployed on average is older than wage-earning individuals. The self-employed are more likely to be male, white, non-Hispanic, married workers, or have higher education levels. They are more likely to report high family income, and live outside a metropolitan statistical area.
5.2. Effect of Self-Employment on Health
Table 4 reports results of the multivariate models. In order to preserve space, only marginal effects of selfemployment are presented. Full model results can be requested from the authors. The coefficients are interpreted as marginal probabilities for the continuous health measures such as Physical Health Composite Score, Mental Health Composite Score, and the Kessler Index.
In the regression models for discrete outcomes, the coefficients cannot be interpreted directly, and thus have been transformed to marginal probabilities [21,22]. For the ordered logit model, where the level of health is a latent variable, we standardize the marginal change in
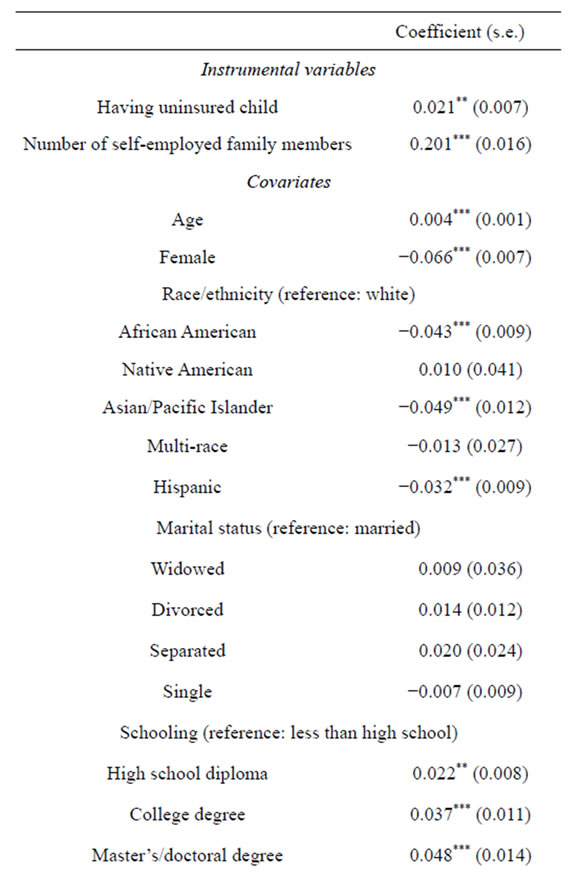
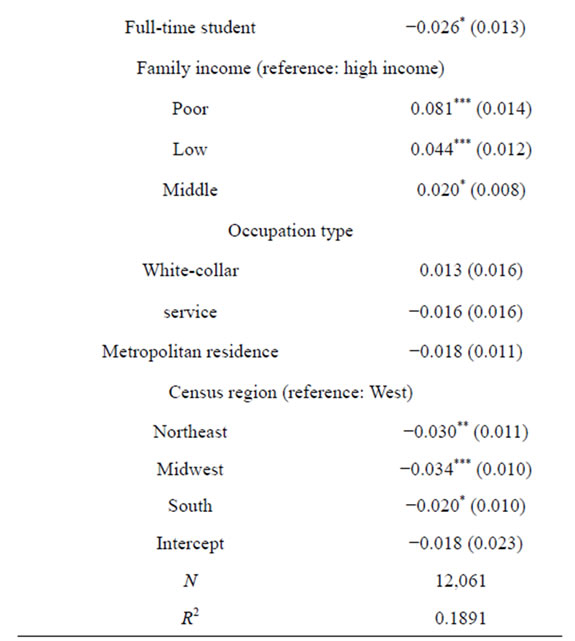
Table 2. First-stage regression on self-employment.
s.e. = standard error. *p < 0.05; **p < 0.01; ***p < 0.001.
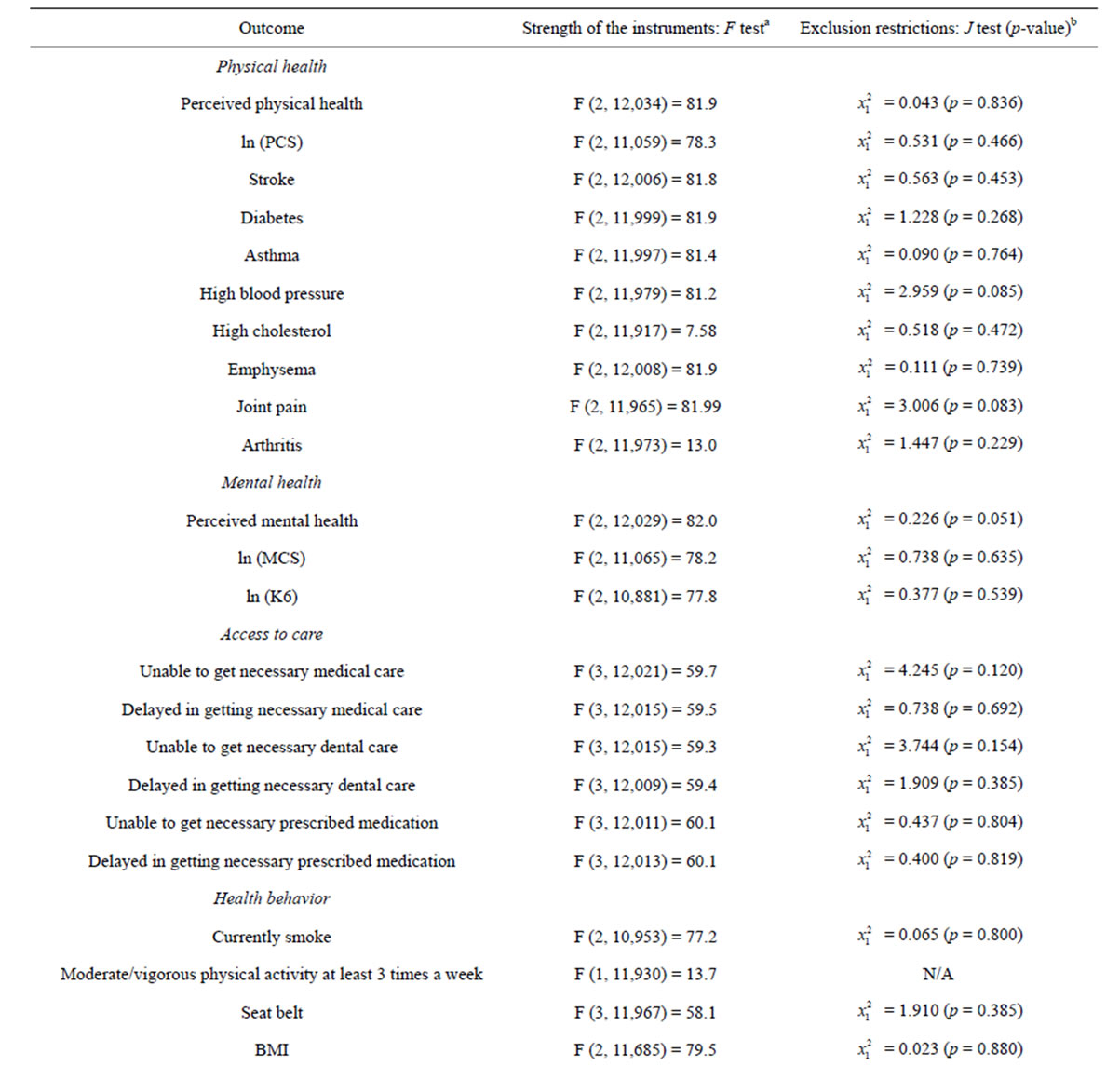
Table 3. Diagnostic tests for the validity of instruments.
aInstruments with a F statistic greater than 10 in general are considered as being strong; bJ statistic must be insignificant for instruments to be valid.
the latent health variable by the estimated standard deviation of the latent variable [33]. Therefore, the marginal effects from the ordered logit models for perceivedphysical and mental health are interpreted as changes in standard deviations of the latent health level for self-employed individuals in comparison to wageearning individuals. For example, the marginal effect on perceived physical health indicates that the health of the self-employed is 0.069 standard deviations higher than that of wage-earning individuals (see Column 1).
Marginal effects in the probit model for binary outcomes are computed as differences in average predicted probabilities between the self-employed and wage-earning individuals, e.g., the self-employed have the approximately 11.6 percentage-point lower risk of diabetes relative to wage-earning individuals (see Column 1). Standard errors are based on 1000 bootstrap repetitions.
Results from the “usual” estimation methods without correction for selection bias, i.e., multivariate linear regression, probit, and ordered logit models-are reported in Column 1. Self-employment is strongly and positively associated with both perception measures and clinical
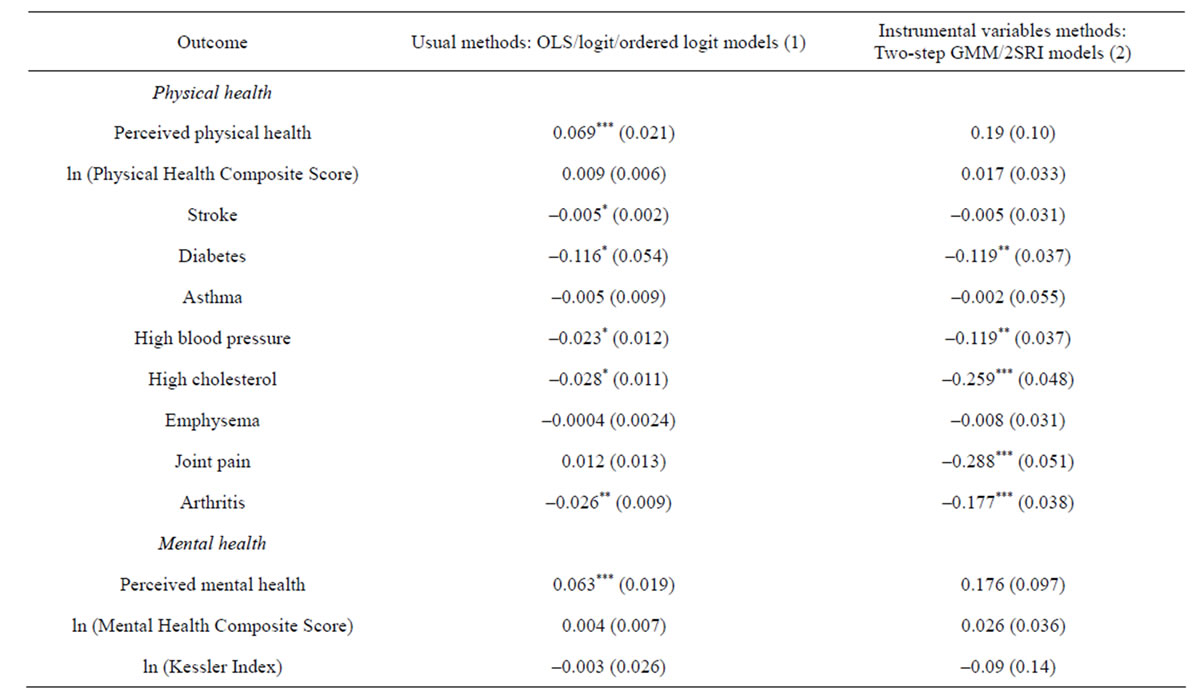
Table 4. Marginal effects of self-employment on health outcomes.
All estimates are survey-weighted. Standard errors are in parentheses and are adjusted for complex survey design. Bootstrapped standard errors (based on 1000 repetitions) are reported for discrete health-outcome models. *p < 0.05; **p < 0.01; ***p < 0.001.
indexes of physical health. The effect of self-employment on perceived physical health status is positive and significant, meaning that the self-employed are more likely than wage-earning individuals to feel they are physically healthy. The marginal effect on self-employment is also positive for ln (Physical Health Composite Score), but is not statistically significant at the 95 percent level. Marginal effects on the medical conditions are and negative and statistically significant for stroke, diabetes, high blood pressure, high cholesterol, and arthritis. The marginal effects appear to be large in magnitude. For example, self-employment is associated with the 2.3 and 2.8 percentage-point lower risk of having high blood pressure and high cholesterol, respectively.
The usual estimation methods in Column 1 find a positive and significant relationship between self-employment and perceived mental health status. However, the marginal effect of self-employment in the clinically validated mental health measures, i.e., ln (Mental Health Composite Score) and ln (Kessler Index)-do not support this association.
Instrumental variables results that address the issue of self-selection into self-employment are reported in Column 2, and are in alignment with those from the usual estimation methods in Column 1, with some exceptions. As discussed above, in the usual models, selfemployment significantly increases perceived physical health and reduces the likelihood of stroke. In the instrumental variables models, the direction of the effect stays the same, but significance is lost. For the joint pain outcome, the instrumental variables result suggests that the self-employment significantly reduces the likelihood of joint pain by approximately 29 percentage points. Overall, the results of the usual model and the instrumental variables model suggest that self-employment is a significant variable in terms of reducing the likelihood of specific physical health conditions.
Regarding mental health, the instrumental variables results reported in Column 2 suggest that self-employment is not significantly associated with any measure of mental health.
5.3. Effect of Self-Employment on Access to Health Care and Health Behavior
Table 5 presents effects of self-employment on the likelihood of experiencing a barrier to health care and the likelihood of engaging in health-related behavior. As shown in Column 1, marginal effects from the usual models show that self-employment is positively significantly associated with the likelihood of being unable to obtain necessary medical care, delay in obtaining necessary medical care, and being unable to obtaining necessary dental care. However, instrumental variables