Prevalence of Dysmenorrhea among Female Adolescents in Dubai: A Cross-Sectional Study ()
1. Introduction
Dysmenorrhea in adolescents is a real dilemma, due to the existence of diagnostic challenges encountered during the investigation pathway, to identify any underlying cause.
In the majority of these cases, no underlying cause could be identified except primary dysmenorrhea. In 10%, dysmenorrhea will be secondary to another underlying pathology, mostly endometriosis or uterine anomalies [1] . Dysmenorrhea which involves pain during menstruation is a perturbing symptom that impairs the quality of life. The highest rate of dysmenorrhea is reported among adolescents. Therefore, it is considered the major reason for school absenteeism and limitation in activities that will ultimately result in poor academic performance and long-term burden on the national economic budget [2] .
Over a century has passed since endometriosis was first described by von Rokitansky in 1860. However, endometriosis is still not less of an enigmatic disease, where little progress has been done to identify the pathogenesis, or to find a cure for this disease [3] .
Owing to its chronic nature, endometriosis mostly can worsen over years, causing permanent damage to the female reproductive system. In addition, the perception of sever menstrual pain during adolescence has been historically “normalized” as a normal association with the menstrual cycle. Hence, it does not come as a surprise the recent publications showing advanced Endometriotic disease among young females during investigations for delayed conception [1] .
Stella et al. conducted an extensive literature review in Sweden and found that dysmenorrhea leads to a total loss of 230,000 working days, which causes a huge financial loss [4] .
Majority of adolescents suffer from primary dysmenorrhea, where no underlying cause could be identified. However, researchers suggest that abnormally high prostaglandin levels could be the underlying cause [5] . Persistence and/or severity of dysmenorrhea should prompt investigations to identify any underlying cause that could reveal secondary dysmenorrhea [6] .
Endometriosis was found in 62% of adolescents with secondary dysmenorrhea. In endometriosis, active endometrial glands and stroma are distributed in the pelvic cavity [4] , and can respond to hormonal influences. There is an intraperitoneal bleeding that mimics menstruation, which results in an intense and progressive inflammatory process [7] , constituting the cornerstone of the dense adhesions. This leads to a permanent destruction of the anatomical and functional potential of the reproductive capacity in adolescents [8] .
Regardless of the type of dysmenorrhea, its severity produces a debilitating effect that persists for a few days and recurs every month [4] . Adolescents with moderate to severe dysmenorrhea fail to enjoy activities of daily livings and may absent themselves from school [9] . Repeated absenteeism will ultimately result in poor school performance that will subsequently have a negative effect on the productivity of society [10] . Increasing evidence confirms that severe dysmenorrhea is a grave symptom that will have an unfavourable outcome on academic and athletic progress [11] .
The prevalence of dysmenorrhea varies worldwide. The reported incidence in 2017 was 72.2%, 89.1%, and 65%, among adolescents in Turkey, Iran, and India, respectively [12] , with similar incidence in gulf countries; however, data for the United Arab Emirates (UAE) are sparse. Reviewed literature revealed that the diagnosis of endometriosis was confirmed laparoscopically in 47% - 73% of adolescents with chronic pelvic pain, who did not respond to medical treatment [13] . This shows that diagnosing endometriosis is not easy, and requires about 12 years for the diagnosis. This difficulty is due to lack of screening tools. In addition, many adolescents perceive severe dysmenorrhea as a normal variant [14] . Therefore, every effort should be made to differentiate between primary and secondary dysmenorrhea to prevent severe outcomes [15] .
Adenomyosis, is another possible reason for secondary dysmenorrhea in adolescence, where the endometrium invades the myometrium. Advances in imaging have led to the diagnosis of the disease among adolescents [16] . These findings may reveal that primary dysmenorrhea can be an early stage of adenomyosis [17] .
In adolescents presenting with dysmenorrhea, symptomatic treatment should be initiated. Such treatments could involve non-steroidal Anti-inflammatory drugs (NSAIDS) and/or hormonal treatment [18] . Unresolved symptoms after 3 - 6 months necessitate further investigations for possible secondary causes [ACOG Committee Opinion 760] (Figure 1) [6] .
This study aimed at investigating the prevalence of dysmenorrhea in Dubai and its effect on academic and athletic performance among participants.
![]()
Figure 1. Dysmenorrhea management algorithm.
2. Methods
2.1. Subjects and Setting
Using a cross-sectional study design, students were randomly recruited from different high schools in Dubai, from both the government and private sectors, to participate in the study during the period between May 2018 to May 2019 academic year. A total of 10 schools participated, of which six were government schools and four were private schools. A total of 470 students were approached. Fourteen were excluded since they did not attain menarche. Therefore, 456 girl students in grades 7 - 12, aged 11 - 19 who met the inclusion criteria, i.e. those who started menstruating and those who agreed to participate in the study, were requested to complete a self-administered questionnaire written in both English and Arabic to match students’ preferences. The questionnaires were filled in their schools to allow further clarification where needed.
Written informed consent was obtained from parents and school authorities prior to the commencement of the study.
2.2. Questionnaire and Other Materials
A questionnaire was prepared in English and Arabic version, based on questions obtained from the World Endometriosis Research Foundation using the Women’s Health Symptom Survey Questionnaire [19] .
The questionnaire was filled by 30 high school students and assessed prior to the study. Based on the feedback, modifications were made for difficult statements. Content validity was reviewed by two experts in this field.
Irrelevant questions for the study age group were excluded, considering the cultural and ethnic background of the country. Those questions were related to the use of contraception, occurrence of pregnancy, and information regarding sexual activity. The final questionnaire composed of 29 questions divided into three sections. The questionnaire included sociodemographic data and questions linked to menstrual cycle. These involved: age at menarche, regularity and duration of the cycle, the associated pain during menstruation and its severity, the use of analgesic, and the degree of relief in menstrual pain. School absenteeism and physical activity during the menstrual cycle were assessed. Further assessment included pain associated with defecation and urination during the menstrual cycle (Appendix 1).
Participants were asked to select between the options yes/no and to use a 1 - 10 Likert scale to grade the intensity of the menstrual pain. The scores were classified into mild (1 - 3), moderate (4 - 7), and severe (8 - 10) dysmenorrhea, using the Multi-dimensional Scoring system (MSS) grading of pain (Appendix 2).
The questionnaire took about 20 minutes or less to complete, followed by an endometriosis awareness lecture.
2.3. Data Analysis
Data were analysed using IBM-SPSS for windows, version 23.0 (SPSS Inc., Chicago, IL). Descriptive statistics are presented as frequencies with percentages, bar chart, pie graphs, measure of central tendency and dispersion.
2.4. Ethical Approval
The study was approved by Dubai Research Scientific Ethical committee in Dubai Health Authority (Approval number: DSREC-03/2018_17). The study protocol was approved by the Ministry of Education (MOE) and Knowledge and Human Authority (KHDA). Informed consent was obtained from all participants.
3. Results
456 girl students in grades 7 - 12, aged 11 - 19 had completed a self-administered questionnaire. The answers to the questions were analysed, as follow.
3.1. Participants Characteristics
Participant characteristics with their menstrual cycle characteristics were assessed using the responses given on the questionnaire (Table 1).
![]()
Table 1. Socio-demographic and menstrual characteristics of participants.
Majority of our participants (79.8%) were natives. There was almost an equal percentage of participants’ mothers with primary/high school degree and university degree, while majority of them were housewives (68.7%). Interestingly, nearly half the population (47.9%) had a family history of dysmenorrhea. A large percentage of the participants (60.5%) had clinically normal menstrual duration that ranged from 5 to 7 days. Dysmenorrhea was found in 94.7% of the total study population. A total of 208 participants (45%) reported severe pain during menstruation (Figure 2).
More than half of the participants (57.1%) did not use pain relieving medications such as paracetamol or NSAIDs for their menstrual cramps. Among the participants who used analgesia, surprisingly more than half (56.6%) reported no relief from pain, while a few (8.6%) with severe pain reported that they needed to go to the clinic or hospital for medical advice. None of the participants reported receiving hormonal treatment (Figure 3(a) & Figure 3(b)).
3.2. Effect of Dysmenorrhea on School Absenteeism and Hindrance to Physical activity
One fourth of the participants reported school absence with each menstrual cycle due to the severe pain associated with it; for the same reason, one third reported cessation of sport activities and missing training, which was frequent among those who were in the national team (Figure 4).
3.3. Exploring Possible Symptoms That Strongly Suggesting Deep Infiltrating Endometriosis (DIE)
Among the participants, 74 (16.3%) and 57 (12.5%) reported pain during defecation and while passing urine, respectively, during each menstrual cycle. Further, 64 (14.1%) students reported persistence of pain after the menstrual cycle (Figure 5).
A total of 124 (28.1%) respondents have shown concern about their menstrual associated pain and were willing to follow up on future clinical assessments for their cases.
![]()
Figure 2. Menstrual Cycle Pain Grading on 1 - 10 Likert scale. This figure illustrates the severity of dysmenorrhea among participants.
![]() (a)
(a) ![]() (b)
(b)
Figure 3. (a) Modalities of treatment used by participants. This figure illustrates modalities of pain relief adopted by participants. (b) Degree of Pain Relief. Illustrates the response of pain relief among participants used analgesia.
![]()
Figure 4. Impact of dysmenorrhea on school absenteeism and hindrance to physical activity. Illustrates the effect of dysmenorrhea on school attendance and physical activities.
![]()
Figure 5. Co-exitance of symptoms suggestive of deep infiltrating endometriosis. Illustrates the presence of symptoms suggestive of deep infiltrating endometriosis among participants.
4. Discussion
The menstrual cycle is a physiological process that declares the potential capability of reproduction. Mild dysmenorrhea is common and expected, however moderate to severe dysmenorrhea is disabling. The problem of persistent dysmenorrhea is more pronounced in adolescents where the negative impact associated with pain can reflect on their academic and physical performance [4] .
The aim of our study was to detect the prevalence of dysmenorrhea among adolescents in Dubai. Therefore, this cross-sectional study was conducted with appreciably high response rate.
Interestingly 218 students mentioned a family history of dysmenorrhea.
Among the 456 students who submitted their responses, we have demonstrated a prevalence of dysmenorrhea in 430 participants, (94.7%), with variable severity (mild = 23.1%, moderate = 33%, and severe = 45%).
This was the highest rate among other studies conducted in the gulf and other Arab countries.
In Saudi Arabia, two studies revealed a prevalence of 70.6% (n = 197); severe (35.2%) and 74.4% (n = 256; mild = 21.1%, moderate = 41.4%, and severe = 37.5%) [20] [21] . In Kuwait, a study conducted by AL Matouq et al. [22] demonstrated a prevalence of 85.6% (n = 763). Another study in Egypt by Kamel et al. [12] reported a prevalence of 84% (269) among university students.
The severity of menstrual pain reported in our study (45%), was higher than that reported in Saudi Arabia at the King Abdul-Aziz University, which was 29% [23] , and that in Lebanon, which was 20% [24] .
Several studies revealed a positive correlation between the severity of menstrual pain and school absenteeism; we found that 24.8% of participants missed their academic classes during the menstruation since they could not cope with the severity of the menstrual pain. Higher rates of 59.4% and 58.2% was reported by Abd El Mawgood et al. [21] and Al Matouq et al., [22] respectively.
A lower rate was however reported by Kamel et al., [12] where 16.8% of the students missed their classes.
Al Asadi and Abdul Qadir [25] revealed that dysmenorrhea affects concentration and distracts student’s attention, leading subsequently to poor academic performance.
In the current study 152 participants (33%) declared complete cessation of their regular training and physical activities during the menstrual period due to painful cramps. This matches approximately to Kamel et al., findings (39.5%) [12] .
Our study was unique in exploring symptoms that are strongly linked with endometriosis, which were painful micturition and defecation during the menstrual cycle. Painful micturition was reported by 43.1% of participants, which was really alarming since it could be a symptom for an underlying deep infiltrating endometriosis [26] .
The other symptom that strongly related to endometriosis was painful defecation during the menstrual cycle and was reported by 46.7% of the participants with varying degrees. Recently Chapron et al. [27] identified this as an independent predictor for DIE, with 74.5% sensitivity and 68.8% specificity [28] .
NSAIDS is the first option for managing menstrual pain. To maximize its effectiveness, it should be taken 1 - 2 days before the onset of menses, to block prostaglandin synthesis by interrupting the action of cyclooxygenase enzyme [28] .
Failure to respond to NSAIDS may be due to the delay in starting dosage, or insufficient dose. This could be the reason for the high failure rate among the participants in the study. Adolescents with persistent dysmenorrhea should have an extensive evaluation to establish an underlying pathological element [29] .
A study by Kamel et al. [12] demonstrated high pain relief rate among the participants (87.2%) after using NSAIDS. This could be related to the age of the participants, since they were college students with a mean age of 20.4 ± 1.7 years.
Although hormonal therapy is recognized as an effective tool in treating dysmenorrhea worldwide, it is not widely accepted as a modality of treatment for adolescents in our community.
The American College of Obstetricians and Gynaecologists, in its committee opinion no. 760 reported that a positive family history of endometriosis in first-degree relative poses a 7 to 10-fold increase in the risk of developing endometriosis. The percentage reported in our study (47.9%) requires further evaluation [6] .
Irrespective of the high rate of dysmenorrhea among participants, majority considered this pain to be a normal part of the menstrual cycle (Figure 6) [23] . This could be related to the cultural beliefs and rituals, which influence the interpretation of menstrual pain.
![]()
Figure 6. Own perception of severe dysmenorrhea. Illustrates the perception of severe dysmenorrhea by participants.
Knowing this fact, we conducted an awareness presentation for all participants from different schools, with the aim of rectifying their knowledge on menstrual pain [14] .
Therefore, further surveys among female adolescents using approved screening tools should be encouraged with the aim of early recognition and treatment of endometriosis in adolescence.
Such implementation will have a tangible impact on the pathological progress of the disease and help avoid its negative effect on female fertility, hence improving the quality of life of these adolescents. It will also help in increasing awareness among those young population [14] .
The study is the first to provide information about the actual existence of dysmenorrhea in Dubai, UAE; thus, we believe it will help physicians to plan and develop strategies for improving reproductive health among this group.
In addition, it was unique in exploring symptoms that suggest endometriosis, therefore it supports moving the diagnosis of endometriosis from surgical to clinical to enhance early diagnosis and prevent grave sequalae [30] .
Our study had few limitations related to the use of a self-reported questionnaire. Moreover, it is a single-centre study, conducted in Dubai, which doesn’t represent the whole UAE.
5. Recommendations
We believe that our study can pave the way for future investigations on a nation-wide scale to investigate the impact of the disease on the quality of life in adolescents. Future nation-wide surveys are needed to accumulate more data on the prevalence of primary dysmenorrhea among schoolgirls and its impact on their social life and physical wellbeing. This data will help formulate baseline information for future researches in endometriosis among adolescent girls in Dubai and other parts of emirates. The cohort of adolescents that presented with symptoms suggestive of endometriosis will require further follow up and clinical evaluations to prevent potential long-term morbidities. It is imperative that appropriate action be taken to educate and provide health services to avoid future impediment to fertility and/or surgical intervention and to prevent central sensitization on those patients.
Based on the results of this survey, awareness on endometriosis and lifestyle modifications were recommended for the study group through educational presentations and follow up meetings.
Further, educating mothers will have a positive impact on disease progression through early recognition and prompt medical consultation with specialists where needed.
Moving the diagnosis of endometriosis from surgical to clinical will undoubtedly shorten the long journey of diagnosing such debilitating disease among adolescents.
Conclusion
Severe dysmenorrhea in Dubai is a crucial problem, and data obtained could reveal endometriosis as a secondary cause.
Advances in Knowledge
This study found a surprisingly high prevalence of dysmenorrhea among female adolescents in Dubai.
Application to Patient Care
This study calls for screening to identify young women who are strongly suspected to have endometriosis in order to alleviate their severe menstrual pain and improve their quality of life, thus reducing school absenteeism, which will have a positive impact on their academic achievement.
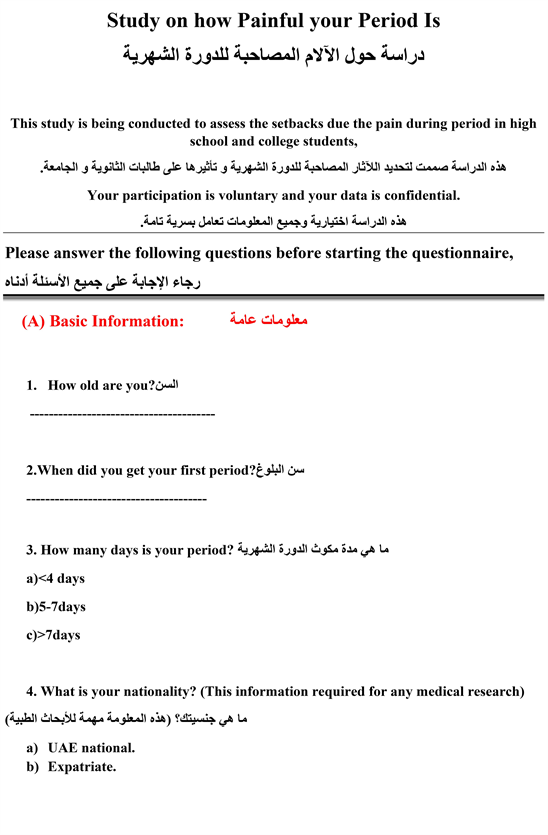
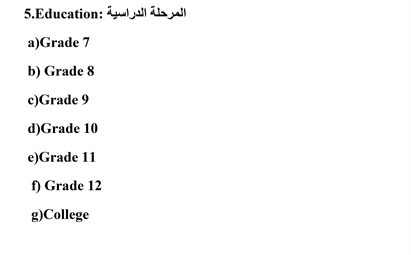
Appendix
1) The study questionnaire.

![]()
![]()
2) Multi-dimensional Scoring system (MSS) grading of pain.