
1. Introduction
Angiographic procedures were first used in 1927 by the Portuguese physician Egas Moniz from the University of Lisbon [1]. In 1929 Werner Forssmann, then assistant physician at the Auguste Victoria Hospital in Eberswalde near Berlin, was the first physician to insert a catheter into a human heart. Fosman performed this procedure on himself and used his own heart as an experimental object. He placed the catheter in a vein in his own hand and from there inserted it into the right atrium of his own heart. Then he went to the x-ray department to prove the success of the procedure. Although he was fired for conducting this experiment, this success earned him the 1954 Nobel Prize in Medicine [2].
To the devotion of many scientists [3] [4] and engineers [5], we owe today the use of modern technical equipment that has become indispensable in our lives. This is especially true for medicine, in which modern examinations would not be possible without the use of x-rays [6] [7] and ionizing radiation in general [8]. The renewal and modernization of the equipment using ionizing radiation are constantly on the agenda [9].
But just as there are benefits from use of ionizing radiation, there are downsides as well. The ubiquitous use of the ionizing radiation sometimes leads to unforeseen consequences―accidents and incidents involving radiation [10] [11] [12]. In this case, the ecological balance is disturbed and the radiation background is exceeded [13]. The radiation background is one of the most important factors for the maintenance of life on the planet Earth. For this reason, it is very important to test for the presence of radionuclides in the air, food and water [14].
In order to reduce the harmful effects of ionizing radiation on our lives and especially in medicine, it is of great importance to keep staff informed and trained so that they can work safely with the respective equipment [15]. Training in this field begins in the student years [16] [17] and continues throughout the career of personnel working with ionizing radiation [18] [19]. But training alone is not enough, it is necessary to constantly study and control the dose load of people working with ionizing radiation. In medicine, this is the medical staff working with x-rays in imaging; with open sources of radiation, in nuclear medicine and metabolic therapy; and with linear accelerators in radiotherapy clinics. Modern x-ray systems of the C-arm type and their variants are indispensable equipments in the work of surgeons, orthopedists, nephrologists, cardiologists and others. They all use X-rays on a daily basis in their work to visualize the part of the human body that they are interested in. Therefore, studying and controlling the dose load received from the medical staff from the scattered radiation during the procedure is critical.
In the monograph “Dose load of staff and patients when working with a C-arm system”, N. Ivanova discusses the dose load of a principal surgeon and his assistant during orthopedic interventions [20]. This topic is further developed by this author in collaboration with the entire research team in several other articles: on the dose exposure of the patient [21] and the staff [22] [23]. The subject of dose load when working with the C-arm equipment in orthopedics and surgery is also discussed in the articles of Wang M.L. et al. [24] and Chapman T. et al. [25].
The modern x-ray angiographic systems are a modified version of the C-arm systems. They are used almost continuously in the invasive cardiology departments. Due to the large number of angiographic procedures per day, whith several projections (different positions of the movable C-arm) there is a danger of receiving a high dose radiation, especially from the principal cardiologist. This is the reason for the special interest in the dose load when using this device. The dose load of the principal cardiologist when using an x-ray angiograph is considered by N. Ivanova in her monograph [26], and in a series of articles, together with a research team [27] [28] [29]. The purpose of the article of D’Alessio D. et al. is to evaluate the radiation dose in patients undergoing liver angiographic procedure and verify the usefulness of different dose measurements to prevent deterministic effects [30]. Diagnostic coronary angiography (CA) uses ionising radiation with relatively high doses, which impacts on both patients and staff. The study of James A Crowhurst et al. sought to identify which patient and procedural factors impact patient and operator dose the most during CA [31].
1.1. Motivation
The calculation and comparison of the dose received by the principal cardiologist in an angiographic procedure is a continuation of the overall study of dose during work with x-ray systems at the Specialized Hospital for Active Treatment in Cardiology in Varna, Bulgaria. This study continues.
1.2. Purpose of the Study
The purpose of this article is to calculate the dose received by the principal cardiologist during the angiographic procedure RCA stenting (Right Coronary Artery). In this procedure, two modes of operation are used: radiography and pulse fluoroscopy. Three projections of the moving arm of the angiographic systems (LAO-cranial, RAO-cranial and Pure Cranial) are examined.
A comparison is made for the dose load in the two modes of operation in the three used projections, for three different positions of the patient table (lowest, highest and zero―the factory preset position), at three points of interest (“Head”, “Gonads” and “Feet”). Based on this comparison, recommendations are made to minimize the dose load of the principal interventional cardiologist during the RCA stenting.
2. Methods
Mathematical calculations are performed on the basis of previously published practical dosimetric measurements [26]. The results are compared using diagrams. Based on the obtained results, the aim is to optimize the dose load obtained
![]()
Table 1. Projections used in the RCA stenting procedure.
from the scattered X-ray radiation during RCA stenting.
Following projections are used in the RCA stenting procedure (Table 1).
Here, the three projections are used as basic projections, but they are performed for different duration.
The total duration of work is about 120 minutes of which:
・ 3 - 4 s beginning with AP projection.
・ Work in the first basic projection (LAO―30˚) for about 60 minutes. The work under x-ray guidance is about 10 minutes pulse fluoroscopy. The duration of the radiography is about 2 - 3 minutes.
・ Work in the second basic projection (RAO-cranial 30˚/30˚) for about 30 minutes, where the duration of pulse fluoroscopy is about 5 minutes. Radiographic mode is used for about 1 minute.
・ Work in the third basic projection (Сranial 30˚) for about 30 minutes, where the duration of pulse fluoroscopy is about 5 minutes. Radiographic mode is used for about 1 minute.
Due to the very low dose load from the initial AP projection, it is not included in the general calculations, because it is practically insignificant.
3. Results
Dose calculations for the different projections are given in Tables 2-4 and the results are illustrated with Diagrams 1-4.
For each of the comparative diagrams, the dose obtained during work with the given mode of operation was calculated: radiography and pulse fluoroscopy. For the first basic projection the calculations are performed for 2 minutes and respective 3 minutes radiography. Therefore, the diagrams show sectors “2 minutes” (summation of fluoroscopy doses for the three projections used and 2 minutes radiography in the basic projection) and “3 minutes” (summation of fluoroscopy doses for the three projections used and 3 minutes radiography in the basic projection).
Comparing Diagrams 1-3 in all three positions of the patient table during the studied procedure RCA stenting, it is seen that all diagrams show the highest dose load for radiographic mode of operation.
For the lowest position of the patient table, Diagram 1 shows that the lowest dose load is obtained for the measurement point “Head” for all three basic projections and for both operating modes used. For this table position we cannot observe a single point with the maximum dose load. For the first basic projection, the highest dose is observed for “Gonads” in both radiography and pulse fluoroscopy.
For the second basic projection, a higher dose is observed for “Feet” in radiographic mode, exceeding, albeit with a very small difference the dose at the point “Gonads”, but in pulse fluoroscopy these two points show equal values.
In the third basic projection, the point “Feet” shows a slightly higher value in radiography, compared to the point “Gonads”, but in the fluoroscopy the opposite is observed―“Gonads” show a higher value.
Comparing the values of Diagram 2 for the highest position of the patient table, the point with the lowest dose load is again the “Head” in both operating modes used in all three projections.
In the first basic projection, the greatest dose load for both modes of operation is again at the point “Gonads”; in the second basic projection, the highest dose load is at the point “Feet” for both modes of operation. In the third basic projection, the higher dose is observed in radiography at the point “Gonads” and in fluoroscopy―at the point “Feet”―although the difference is small.
Diagram 3 illustrates the dose load received in the zero position of the patient table and shows similar ratios of the measurement points, such as Diagram 2. Here, too, the lowest dose value is observed in the point “Head” for both modes of operation and for the three used projections. The highest dose measured in the first basic projection is at the point “Gonads”. In the second basic projection, “Gonads” and “Feet” show almost equal values―at the point “Gonads” the radiography shows some higher values and for the pulse fluoroscopy the values are equal. In the third like in the first basic projection, the maximal dose value is observed at the point “Gonads”.
Comparing the dose values from Diagram 4 showing the dose load for the whole procedure in all three positions of the patient table, the most and the least irradiated points are very clearly outlined. These are “Gonads” and “Head”
![]()
Table 2. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the lowest position of the patient table, at three points of his body.
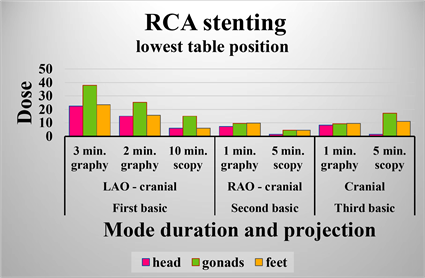
Diagram 1. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the lowest position of the patient table, at three points of his body.
![]()
Table 3. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the highest position of the patient table, at three points of his body.
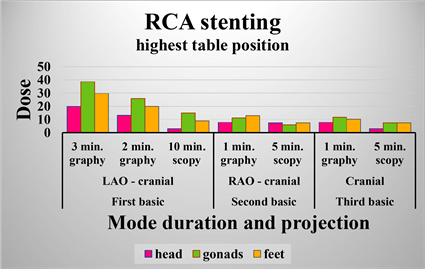
Diagram 2. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the highest position of the patient table, at three points of his body.
![]()
Table 4. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the zero position of the patient table, at three points of his body.
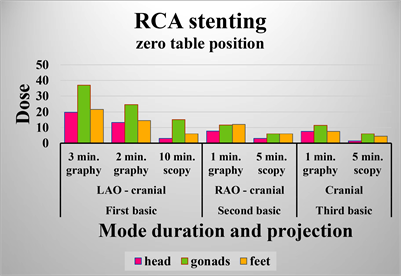
Diagram 3. Dose received during the angiographic procedure RCA stenting by an interventional cardiologist for the zero position of the patient table, at three points of his body.
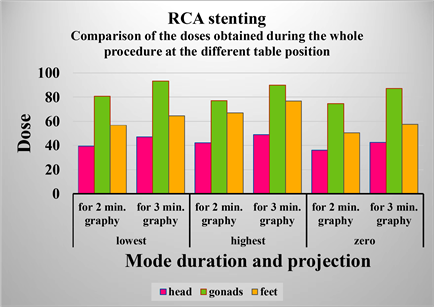
Diagram 4. Comparison of the doses obtained during the whole procedure at the different position of the patient table.
respectively for both modes of operation―radiography and pulse fluoroscopy, for all three table positions―lowest, highest and zero position.
4. Conclusions
Based on the results of the dose load study during the RCA stenting procedure, it becomes clear that radiography generates most of the dose load received, although the duration of work with radiography is significantly shorter than the duration of work with fluoroscopy. While the work in radiography is about 4 - 5 minutes for the whole procedure, the work in pulse fluoroscopy is about 20 minutes for the whole procedure, i.e. about 4 - 5 times longer than in radiography.
If we look at the dose values obtained in the various projections, it can be seen that the dose load is maximal in the first basic projection, since the durations of radiography and fluoroscopy are the longest―around 14 to 15 minutes total time. For the other two projections the total time is approx. 6 minutes.
In the first main projection, the highest number of high dose values (average value 21 μSv) is observed at the highest position of the patient table. In the zero position of the table the average value is the lowest―17.16 μSv. Therefore, the most suitable position to obtain lowest possible dose load in the first basic projection (where the dose load is the largest), is the zero position of the patient table.
In the second basic projection, the largest number of high values (average value 8.8 μSv) is observed again in the highest position of the patient table and the lowest values (average value 6.63 μSv) are observed in the lowest position. Therefore, during work in the second projection the most suitable position is the lowest position of the patient table.
In the third basic projection, the highest number of high values is obtained in the lowest patient table position (average value 9.5 μSv) and the lowest values (average value 6.4 μSv) in the zero position of the table. Thus in the third basic projection, it is advisable to work in the zero position of the table. However, as it is practically inconvenient to constantly change the position of the patient table during the procedure, it is necessary to work only in one position, as convenient as possible for the cardiologist.
Taking into account the above conclusions, we can recommend to the principal cardiologist to work in the most convenient position of the patient table, but closest to the zero position, because this position shows the lowest dose load in two of the projections―the first basic projection (giving the largest part of the dose load) and third basic projection.
The comparative Diagram 4 for the whole procedure and the three table positions confirms the conclusion already made about the table position giving lowest dose load in the RCA stenting procedure.
The comparative Diagram 4 shows that the most irradiated point is the gonads. This leads to the conclusion that the radiation protection of this point is of particular importance. At the same time, this part of the body is one of the most sensitive to radiation, which leads to the conclusion that the cardiologist and other medical staff working in this procedure must use a lead-rubber apron with a lead equivalent of at least 0.5 mm.
The lowest dose load is obtained for the point “Head”. However, prolonged exposure to scattered x-rays of the cardiologist would lead to a high dose load on the head and all the organs in it and the neck.
In this regard, radiation protection of the head and the neck with a lead-protected hat, lead-protected goggles and a lead-rubber collar is highly recommended.
The feet also receive a considerable dose load, but the limbs are the least sensitive parts in the human body, so no additional protection is required for them.
5. Recommendations
As result of all told above, following recommendations can be made:
1) To look for and use ways to reduce the time to work under radiography mode. For example this could be achieved with appropriate training and prior accumulation of experience.
2) The patient table should be placed in the most comfortable position for the principal cardiologist, but as close as possible to the zero position and
3) Individual radiation protection equipment must be used.
Acknowledgements
Special thanks to the three physicians, members of our research team, from the Cardiology Hospital, Varna, Bulgaria: Dr. Ismet Tahsinov, Ph.D. Hrisimir Todorov, Ph.D. Nikolai Aleksandrov, without whose invaluable help our team would not have done so well.
Special thanks also to the medical physicist Bistra Manusheva, Head of the Radiation Control Department at the Regional Health Inspectorate, Varna, for the provided equipment for the dosimetric measurements.
Special thanks to Natasha Ivanova from the Medical University, Varna for the provided data, on the basis of which we prepared this article.
And last but not least, special thanks to the editors of the magazine for their help in printing the article.