Examining the Benefits and Challenges Associated with the Use of the Mobile Renewal Service in Ghana ()
1. Introduction
Ghana’s public sector is rapidly changing in terms of ICT. Government agencies with a solid offline reputation are increasingly using their brand value to provide online services. Ghana’s government is committed to modernizing public service delivery through electronic government technologies. The Ghanaian Ministry of Health has developed a list of goals for the country’s Universal Health Coverage (UHC) plan. Authorities have been tasked to use ICTs and other E-government solutions as part of the E-Ghana plan modules.
National Health Insurance Authority (NHIA) has introduced the Mobile Renewal Service, which allows NHIS subscribers to renew their expired NHIS cards using their mobile phones. Compared to the traditional service renewal process, the service is available 24/7, eliminating queues and reducing branch operating hours. Despite its many advantages, adopting new technology has drawbacks.
1.1. Background to the Study
Ghana’s government has unveiled a new digital plan to build on the country’s recent progress in digitizing government services. The reforms have already begun to bear fruit for the economy, with import revenue increasing by 3.9 percent to GHS13.2 billion ($2.6 billion) in 2018, indicating that the reforms are having an impact. It was hosted in May 2019 that an international conference on “Moving Beyond Aid: Expanding the Local Digital Economy” was held on the theme “Moving Beyond Aid: Expanding the Local Digital Economy”. An extensive range of issues were covered at the conference, including e-government, industrial automation and cybersecurity, as well as the promotion of public-private partnerships (PPPs). In line with the digitalization plane of the Government of Ghana (GoG), the National Health Insurance Scheme (NHIS) launched the Mobile Renewal Service on December 17, 2018, to make renewing coverage easier for members. This novel method of renewing membership and paying premiums aims to increase NHIS enrollment and retention rates (NHIS). To use the service, dial *929# from any mobile network.
Given the efficiency and effectiveness of the Mobile Renewal Service, which includes reducing congestion at the many NHIS District offices across the country, saving time, and decreasing operational expenses, it is worthwhile to examine the benefits and challenges associated with using this service, as well as ways that NHIA could improve the service in order to attract a larger audience.
1.2. Literature Review
This chapter summarizes the study’s review literature. It includes both a conceptual review and a review of ideas pertinent to this study’s course.
The concept of e-service is one practical application of ICT. E-services are actions or sequences of actions performed by a provider or a consumer via an electronic network. E-services include web, mobile, and information kiosks. Traditional services are replaced by e-services to satisfy digital technology. It is a service platform that uses ICTs, such as electronic networking services (information, interaction, transaction, etc.). Provider, receiver, and technology are three platforms for electronic services. Telephony, call centers, public kiosks, mobile phones, and television are also evaluated. Lu (2001) claims that e-service increases customer base, transparency, and consumer awareness. E-service is becoming increasingly important in assessing e-commerce success (Yang & Jun, 2001). It improves the customer’s knowledge flow. With e-service came higher labor costs and technological advancements, customers can now generate and consume services without direct contact with suppliers. E-service can help you succeed and save time. E-service will automate and nurture customer relationships (Taherdoost, Sahibuddin, & Jalaliyoon 2014).
Clients use e-services with caution because they change competitive, business, and consumer relationships. According to Taherdoost, Sahibuddin and Jalaliyoon (2014), electronic services that only replace human contact are not widely used. Now, everyone uses e-services. The utilization and relevance of e-Services are more vital than ever. More services are now being offered online/electronically (e-Services) than ever before due to the usage of technology in all services and the COVID-19 pandemic forcing us into a digital transformation of our work and lives.
Electronic Health Definition
E-health has no agreed-upon definition. But only in a medical setting. E-health is a general term for medico-technological coupling (Khalil & Jones, 2007). Services, information, and research in e-health include healthcare (Denardis, 2011). “The use of technologies and data to support clinical services provided by health care teams or patients”, say Curtis, Cunningham et al. Scholars cannot agree on eHealth. Aspects of trade and healthcare were studied by some researchers. The World Health Assembly approved it in 2005 as a way to develop affordable and reliable ICTs for health and related fields. The WHO has advised member countries to adopt long-term plans and strategies for e-health service delivery and infrastructure development (Healy, 2008).
Eysenbach (2001) define e-Health as “health services and information delivered or enhanced via the internet or related technologies”. The term refers to “a networked, global review of health care using information and communication technology to improve health care locally, regionally, and globally”.
eHealth can be implemented at the micro/individual, meso/institutional, and macro/societal levels. Many jurisdictions, especially in developing countries, have embraced eHealth (Royal College of Nursing, 2012).
Affecting eHealth adoption, success and effort expectations are minor factors (Kesse-Tachi et al., 2019). Also, according to Mendiola et al. (2015), healthcare professionals are resistant to change (Mendiola et al., 2015). The inability of healthcare information systems to communicate and the many competing and overlapping eHealth standards are major deterrents. These information systems occasionally collide (DeNardis, 2011).
Electronic Services in the Ghana Health Sector
Like other developing countries, Ghana’s healthcare system is poorly accessible to rural areas (Afarikumah, 2014). It was Ghana that pioneered Community-based Health Planning and Services (CHPS), National-scale Community Health Workers (NCHW), and Telemedicine, according to Afarikumah (2014). E-health is new in Ghana. A robust, state-of-the-art health ICT platform with unique ID numbers for all patients in Ghana can help Ghana achieve the Sustainable Development Goals (SDGs) faster than any other country. ICT has become a leading solution for achieving health and development goals since the SDGs were adopted. It was launched in July 2010 by the Ghanaian government. In addition to distribution and data collection, many international organizations have implemented telemedicine pilot projects. Other initiatives include the launch of web-based health advisory services and the support of numerous companies and government agencies. According to research, Ghana has around twenty-two (22) active eHealth projects (Afarikumah, 2014), most of which are funded by donors. Onetouch Medicareline, Mobile Teledermatology, SMS for Life Logistic Management, and others are among the programs. At the moment, Afarikumah (2014) claims there is growing interest in the potential benefits of eHealth, especially for remote areas.
Studies show that healthcare administrators’ administrative traits and characteristics influence the adoption of eHealth (Kesse-Tachi et al., 2019). Health care organizations have increasingly used electronic systems and ICT to improve patient care. The world is currently developing many applications based on computerized medical information, electronic patient records, and communications, improved data processing, remote education, telemedicine, and public services. Many e-solutions in the health sector are becoming increasingly popular, according to Al Basheer and Al Morshid (2010).
Mobile Phone Utilization in the Health Sector
Smart devices and wearable technology are becoming more common. No wonder millions of people use these devices to track and preserve their health. This phenomenon has spawned a new health delivery model: mobile health. Cell phones are widely used in the medical field, but little research has been done on their effectiveness. Mobile devices have become increasingly accessible and affordable, and mobile technologies and communication systems have grown exponentially in the last decade (Tian, Zhang, & Zhang, 2020). It was named after Robert Istepanian, who coined the term mHealth in 2005 (Istepanian et al., 2006).
Cell phones, patient monitoring devices, PDAs, and other wireless devices are examples of mHealth, according to the WHO. Earlier research has shown the importance of mobile phones in health care.
Ling (2004) asserts that the advent of cell phones in disadvantaged communities has spawned a new social networking model centered on health seeking rather than friendship and social relationships. The unique structure of disadvantaged audiences’ cell phone use often resonates strongly in health crises. It has been argued that cell phone use is better related to activity coordination. It has been argued that cell phone use correlates better with emergency transport planning (Horst & Miller, 2006; Ito, 2005).
Heart disease, diabetes, autism, insomnia, and asthma are now tracked using mobile phones. Researchers are also looking into mHealth’s potential, such as mobile HIV interventions. Some healthcare providers use text messaging to improve medication adherence and clinical appointment attendance. A simple text message helps HIV patients stay on their ART medication. The Australian ACT government has created a website promoting mHealth for diabetes management. In Sierra Leone, for example, cell phones are used to coordinate a wide range of social relations. In most cases involving vulnerable and disadvantaged individuals, well-organized networks of relatives, friends, and neighbors make the treatment decision. However, the examples of people using their phones for health care show that users can create social media contexts that include digital media. Many mHealth systems provide large-scale health care in the developing world. A cost-effective, equitable and high-quality health care system is promoted by the state in Bangladesh (Ahmed et al., 2014).
Measure up/press down, an American Medical Group Foundation mHealth initiative, has already improved hypertension diagnosis and management for over 400,000 people. During the campaign, patients use an automated blood pressure monitor connected to a smartphone to record their readings. This information is automatically sent to the patient’s doctor, who will check and monitor their blood pressure. Studies on the effectiveness of cell phone research in promoting and strengthening preventive healthcare have shown that only certain measures are effective. Consumer satisfaction is an important determinant of an intervention’s effectiveness.
According to Cresswell (2003), mobile technology can help the most vulnerable Ghanaians. Positive patients can now call in and schedule their next counseling session with hospital counselors. Only a third of the patients Cresswell (2003) spoke to own a phone. In addition, patients and healthcare workers face high calling costs.
Also, none of the above mobile phone interventions involve using the phone to pay for healthcare. But Ghana is not the first country to use mobile phones to renew health insurance. Kenya launched M-Pesa in March 2007. M-Pesa is a platform that allows health insurance subscribers to renew monthly. Despite its popularity among Kenyan National Health Insurance members, no research has been done on its use. The use of mobile money to pay for health care bills is new in Ghana, where “some health facilities, especially private health care providers” accept it (Boaheng et al., 2019). According to Boaheng et al. (2019), one benefit of cell phone premium payments is allowing those who cannot afford to pay their premium in advance to pay in installments for NHIS membership. According to some research, “urban living, senior high education, tertiary education, and informal employment are determinants of paying the NHIS premium with a mobile phone” (Boaheng et al., 2019).
Surprisingly, given the rapid growth of mobile technology, research on mobile service adoption is still in its infancy. According to Hosbond & Nielson (2005), previous research on mobile system development has a significant focus on the technological viewpoint, which examines how associated technologies contribute to mobile system development. Few researchers have studied mobile service adoption. As stated previously, no research has been done to examine the benefits and challenges associated with using the Mobile Renewal Service. As a result, examining the benefits and challenges of the Mobile Renewal Service is critical.
Mobile Money
A mobile wallet service allows users to send and receive money using their mobile phones. Money is received, stored, and spent using a mobile phone or other mobile device, which is called mobile money. mPesa, EcoCash, GCash, Tigo Pesa, and many others are examples of mobile wallets. Mobile money services are widely available in Africa, Asia and Latin America. Due to its ease of use, security, and availability anywhere a mobile phone signal exists, mobile money is quickly becoming a cash and bank substitute.
For its convenience and safety, mobile money has surpassed bank accounts in popularity. It works on smartphones as well as basic phones.
An equivalent amount of Bank notes and coins is stored in a mobile phone’s Subscriber Identification Module (SIM). In order to use Mobile Money, you need to have a SIM card in your phone.
Financial services cannot be delivered profitably through traditional branch-based channels, according to the Global System for Mobile Communications (GSMA). These services include electronic wallets used to send and receive money between people (G2P). A global average daily value of P2P transactions on MM platforms is estimated at USD35.00 (GH150.00) by the Global System for Mobile Communications (GSMA).
In Ghana, mobile money wallets are used to pay for goods and services such as airtime, utility bills, gold and DSTV, some workers’ salaries, taxi fares, micro-credit, savings, and micro-insurance, among other things. A quarter-end interest payment on mobile money float balances results from the store of value function of mobile money (MM). It was GHC1.257.40 million at the end of 2016, compared to GHC547.96 million in December 2015. In 2016, e-wallet users received GH24.79 million in interest.
The Benefits and Challenges associated with the use of New Health System
In South Africa, Cline and Luiz (2013) look at how hospital information systems affect service delivery, user acceptability, and organizational culture. In two public tertiary healthcare facilities, 94 physicians, nurses, and hospital administrators were interviewed (in two provinces). The interviews used standardized questionnaires with both qualitative and quantitative data. Our two hospital groups, as well as the three sample groups of doctors, nurses, and administrators, had large disparities. Automation has been shown to improve patient experience, hospital staff workflow, and overall workplace morale in public-sector hospitals.
Mendiola, Kalnicki and Lindenauer (2015) identify the patient-consumer (user) characteristics that result in a good app rating. They examined 234 apps from the medical, health, and fitness categories of the Apple iTunes and Google Play stores for the presence of 12 app characteristics and attributes. Regression analysis was used to determine which aspects influenced a user’s app rating. Only five of the twelve criteria were statistically significant, accounting for 9.3% of the variation in each app’s rating (R square = 0.093, n = 234, P = 0.001). Plan or orders, data export, usability, and pricing all contributed positively to a user’s review while the tracker function detracted. User-friendly apps that communicate with designated people are preferred over time-consuming apps that do not communicate with designated people.
To assess how consumers, use health apps to monitor their health, Anderson, Burford and Emmerton (2016) conducted a comprehensive study. Customers aged 18 and over who use any health app for self-monitoring were invited to interviews in Perth, Australia. In only one study, a semi-structured interview guide based on the TAM and the Mobile Application Rating Scale was used. These models also aided in the deductive theme analysis of interviews. Inductive analysis was used to investigate non-model reactions.
Zhou, Bao, Watzlaf and Parmanto (2019) research mHealth app security barriers and facilitators. This study sought to establish a link between user characteristics and security and privacy issues in mHealth apps. The University of Pittsburgh’s Pitt + Me website was used to recruit research volunteers. Most mHealth app users are concerned about their privacy. Simple security measures and user privacy protection legislation may encourage consumers to use mHealth apps. The lack of security features and the high cost of apps have also been identified as barriers.
1.3. Purpose of Study
The study seeks to:
1) Determine the service’s perception and level of recognition in society by subscribers.
2) Examine the benefits and challenges associated with the usage of the Mobile Renewal Service.
2. Methodology
Research Design, Population, Sample Size Determination and Data Processing Procedure
The study used a descriptive survey design to assess subscribers’ perceptions of the service, as well as the benefits and challenges associated with its use. This study used the quantitative research method. The population considered in this study is subscribers selected from 11 District Offices of the NHIS in the Northern Region. A sample of about 50 subscribers purposively selected from the population from each District Office was randomly selected. These constituted a fair representation of the organization being studied and whose perception and orientation give a fair idea about the benefits and challenges associated with the use of the Mobile Renewal Service. The Technology Acceptance Model (TAM) helps to predict and make sense of user acceptance of information technologies. In TAM, two constructs, Perceived Usefulness (PU) and Perceived Ease of Use (PEOU), are the fundamental determinants of system use. These constructs predict attitudes towards using the system, that is, the user’s willingness to use the system.
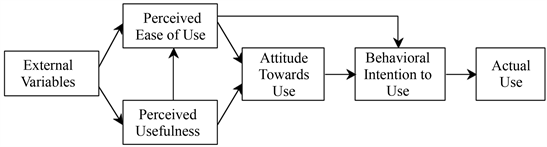
Source: Davis (1989).
The study utilized a survey questionnaire designed with the aid of elements of Technology Acceptance Model (TAM) namely; Perceived Ease of Use (PEOU), Perceived Usefulness (PU), Intention to Use (IU), System Quality (SQ), Transaction Cost (TC) and Accessibility (AC) in the collection of the quantitative data for the study.
The researcher entered, processed, and analyzed the participants’ data using IBM Statistical Package for Social Sciences (SPSS) Version 21, Smart PLS, and Microsoft Excel Package. The study used descriptive and inferential statistical tables. The demographic profile of the participants was determined using descriptive statistics of frequency distributions and means scores-standard deviation techniques, as well as the benefits and challenges associated with using the Mobile Renewal Service (Table 1).
![]()
Table 1. Cluster of district in the northern region.
3. Analysis and Discussion
3.1. Demographic Profile of Respondents
This section examines respondents’ backgrounds. Primary data analysis assesses participants’ socio-economic characteristics to determine their suitability for responding to study questions. Gender, age, education, and employment status are among the socio-economic factors considered.
Table 2 shows the study’s participants’ demographics. The study reports 224 males (55.31%) and 181 females (44.69%). Males dominated the study, according to the findings. With 197 (48.64%) and 144 (35.56%) of those aged 21 - 29 and 30 - 39, respectively, the least participating age group is 50 years and older (2.72 percent). The study’s main participants are youngsters. The respondents’ education attainment distribution was 134 (33.09%) for Diploma and 118 (29.14%) for Bachelor. Other educational distributions include 50 (12.35%) Masters and Two (0.49%) PhD holders. The findings show that most participants are highly educated, making them ideal study subjects. Finally, the Public Sector reported 194 (47.90%) and the Unemployed 167 (41.23%) employees, with the Private Sector having the least representation. The results show that the Public Sector is the most represented group.
![]()
Table 2. Reliability test outcome for constructs under investigation.
Source: Author’s construct.
3.2. Descriptive Statistics
This section summarizes the study’s measurement items’ descriptive statistics. The questionnaire used 19 items. Items used to assess the research construct came from prior research on new system acceptance. Several items were changed to fit the current study’s purpose. The standard deviations, mean scores, skewness, and kurtosis of the 19 items were assessed. Table 3 summarizes the measurement items’ descriptive statistics. Standard deviation indicates a narrow distribution around the mean, between 0.73 and 1.40. Except for negative items, the study reports mean scores greater than 2.50. Overall, this indicates a positive response to the study’s constructs. This suggests a normal distribution because all of the values fall within the appropriate ranges for normality (i.e., −1.0 to +1.0) skewness and less than 10 kurtosis (Kline, 2010).
4. Results and Discussion
This section of the work presents an analysis of the field findings with respect to the benefits and challenges associated with the use of the mobile renewal service
![]()
Table 3. Descriptive statistics of measurement items.
Source: Author’s construct.
in response to the third research question: What benefits and challenges are associated with the use of the Mobile Renewal Service by subscribers? The NHIS was introduced to address the problems plaguing Ghana’s healthcare system, namely the “Cash and Carry” payment system, which requires patients to pay cash before receiving care, resulting in inequities in financial access to healthcare (Kesse-Tachi et al., 2019). NHIS members were supposed to be relieved of the burden of long-term enrollment and renewal expenditures at NHIS offices by the NHIA’s implementation of cell phone membership renewal (Boaheng et al., 2019). The use of mobile phones for membership renewal and subscription payments is expected to increase membership enrolment, retention, and overall healthcare delivery in Ghana. The NHIA mobile renewal system is not without its challenges. National Health Insurance Authority Ghana (2019) cites network issues, card activation issues, double renewals, lengthy processes, and some NHIS users’ lack of IT expertise as major obstacles to implementing and using mobile renewal.
The subsequent sub-sections provide the summary of results about the benefits and challenges associated with the use of the Mobile Renewal Service using the Mean (M) and Standard Deviation (SD) techniques and percentages of Likert Scale of “1”, “2”, “3”, “4”, and “5” respectively for Strongly Disagree, Disagree, Neutral, Agree, and Strongly Agree. Following Atunde and Aliyu (2019), measurement items with mean scores less than 2.50 and higher dispersion are deemed irrelevant and rejected. The underlying statistical principle is that an acceptable measure is associated with a higher mean score and reduced variability. The percentage distribution from the Likert Scale data follows the usual statistical proportional analysis.
4.1. The Benefits Associated with the Use of the Mobile Renewal Service
This section discusses the advantages of implementing Mobile Renewal Service in Ghana’s Northern Region. Table 4 summarizes the findings on the subject. The study asked participants about the benefits of implementing mobile renewal
![]()
Table 4. Benefits associated with the use of the mobile renewal service.
Source: Author’s construct.
service. All items have higher mean scores with low standard deviations. The first statement “Members can now conveniently renew their NHIS subscription from the comfort of their homes via mobile renewal service” received a M score of 4.23 and an SD of 0.85, indicating that on average, participants agreed.
The statement “Renewal time has been reduced to minutes” had M 4.13 and SD 0.87. This indicates that, on average, respondents agreed that the mobile renewal service reduced renewal time by minutes. The study also wanted to know if respondents agreed or disagreed with the statement that members can renew without incurring travel costs, resulting in financial savings. The V value for this statement is 4.11, with an SD of 0.89, indicating that respondents agreed that the mobile renewal service allows NHIS members to renew without incurring travel costs.
Participants viewed almost all items as signals to evaluate the benefits of using the mobile renewal service. As a result of the mobile renewal service, NHIS members can now conveniently renew their subscription from the comfort of their homes without incurring travel costs.
Table 5 shows the percentage distribution of Likert Scale data used to support M and SD techniques on the benefits of using the mobile renewal service (%). In response to the statement “Members can now conveniently renew their NHIS subscription from the comfort of their homes via mobile renewal service”, 46.17 percent agreed, 41.98 percent strongly disagreed, and 6.42 percent moderately agreed. Moreover, 3.95 percent of those polled disagreed, and 1.48 percent strongly disagreed. Members can now conveniently renew their NHIS subscriptions from the comfort of their homes via mobile renewal service.
According to the findings, 49.14 percent of respondents strongly agreed with the second statement, while 36.05 percent agreed. However, 8.40% of them agreed with the statement, while 4.94% disagreed, and 1.48 percent strongly disagreed. According to the results, most subscribers agreed that “Renewal time has been reduced to minutes”.
![]()
Table 5. Benefits associated with the use of the mobile renewal service.
Source: Author’s construct.
The research also asked respondents if “Members can renew without incurring travel costs, resulting in financial savings”. The data collected shows that 47.90% of them agreed with the statement while 35.80% strongly agreed. Again, 10.37 percent of those polled agreed moderately, 3.70 percent strongly, and 2.22 percent strongly. The results show that most subscribers strongly agreed with the statement “Members can renew without incurring travel costs, resulting in financial savings”.
4.2. The Challenges Associated with the Use of the Mobile Renewal Service
Participants were asked about the challenges of using the mobile renewal service. Table 6 summarizes the above descriptive statistics. It has a 4.28 M score and an SD of 0.90. In the sampled Districts, the main problem associated with using the service to renew membership was “Lack of user understanding of steps involved in using mobile renewal service”.
“Mobile network challenges in renewing insurance premium” was also discussed in Table 6. That’s the second most concerning issue associated with the Mobile Renewal Service, after the aforementioned 4.25 M score. These results indicate that most respondents agreed that “Mobile network challenges in renewing insurance premium” was true, and that renewing insurance premium is another major challenge for NHIS members using the mobile renewal service.
“Subscriber resistance to switching from manual renewal to mobile renewal service mode” is the next major concern. The responses indicate a 4.22 M score with a 0.85 SD. As a result, “Subscriber resistance to switch from manual to mobile renewal service mode” is one of the main challenges associated with using the Mobile Renewal Service in the studied areas.
A score of 4.02 with 0.81 for “Lack of knowledge and skills to use the Mobile Renewal Service”. The results show that subscribers lack knowledge and skills to effectively use the mobile renewal service to renew their NHIS membership in
![]()
Table 6. Challenges associated with the use of the mobile renewal service.
Source: Author’s construct.
the sampled districts in Northern Ghana. This indicates that respondents agreed that “lack of knowledge and skills to use the Mobile Renewal Service” is a challenge.
Following the field data collected and analyzed, it can be inferred that in assessing the challenges associated with the use of the Mobile Renewal Service in the selected districts, the findings presents the following in order of severity as the main issues:
1) Lack of user understanding of steps involve in using Mobile Renewal Service;
2) Mobile network challenges in renewing insurance premium;
3) Subscriber resistance to switch from the manual renewal method to the mobile renewal service mode;
4) Lack of knowledge and skills to use the Mobile Renewal Service and mobile network challenges in renewing insurance premium.
This implies that NHIS subscribers in the study area perceive the afore-stated challenges as major obstacles to the use of the system.
Table 7 shows the percentage distribution of Likert Scale data supporting M and SD techniques on the challenges associated with using the Mobile Renewal Service. On the statement “Subscriber resistance to switch from manual renewal to Mobile Renewal Service mode”, 43.21 percent strongly agreed, 41.48 percent agreed and 10.62 percent agreed moderately. 3.95 percent of those polled disagreed with the statement, and 0.74 percent strongly disagreed. It appears that most subscribers strongly agree that switching from manual to mobile renewal is a difficult transition.
The study found that 58.77 percent of respondents agreed with the statement “Lack of knowledge and skills to use the Mobile Renewal Service”, and 25.19 percent strongly agreed. 96.33% agreed with the statement, compared to 5.433% disagreeing and 0.993% strongly agreeing. Overall, most subscribers agreed with the statement “Lack of knowledge and skills to use the Mobile Renewal Service”.
![]()
Table 7. Challenges associated with the use of the mobile renewal service.
Source: Author’s construct.
The researcher also asked the participants about “Mobile network challenges in renewing insurance premium”. The data collected shows that 49.63 percent strongly agreed with the statement while 33.33 percent agreed. Again, 10.12% of the sample agreed moderately, 5.93% disagreed, and 0.99 strongly disagreed. Overall, most subscribers agreed with the statement “Mobile network challenges in renewing insurance premium”.
Finally, on the statement “Lack of user understanding of steps involved in using Mobile Renewal Service”, 48.89% strongly agreed, while 36.79% agreed. 2.72 percent strongly disagreed with the statement, and 0.99 percent strongly disagreed. Overall, most subscribers agreed with the statement “Lack of user understanding steps involved in using Mobile Renewal Service”.
5. Conclusion
The study examined the benefits and drawbacks of implementing the Mobile Renewal Service in Ghana. The NHIS was created to address the problems caused by Ghana’s healthcare system’s “Cash and Carry” payment system, which requires patients to pay cash before receiving care, and the resulting inequities in financial access to healthcare. Following some of these breaches, the NHIA planned to deploy mobile membership renewal to relieve NHIS members of the burden of long-term enrollment and renewal spending at NHIS offices. This will improve membership renewal, enrolment and retention, and overall healthcare delivery in Ghana. However, implementing the NHIA mobile renewal system is not without challenges. The NHIA report (2020) cites network issues, card activation issues, double renewal, lengthy process stages, and a lack of IT experience on the part of some NHIS clients.
Concerning the benefits associated with the implementation of Mobile Renewal Service in selected districts within the Northern region of Ghana, the analysis shows that almost all the items are perceived by the participants as signals to assessing the benefits associated with the use of the mobile renewal service. The findings present the following in order descending as the gains associated with the System’s use: Members can now conveniently renew the NHIS subscription from the comfort of their home via mobile renewal service; Renewal time has been cut down to minutes; and Members are able to renew without incurring travel costs and this directly translates into monetary savings. This suggests that following the implementation of the mobile renewal service, NHIS members are able to now conveniently renew the NHIS subscription from the comfort of their home via Mobile Renewal Service, renew without incurring travel costs and that this directly translates into monetary savings supporting the predictions in National Health Insurance Authority Ghana (2019). The findings corroborates those of several other studies (Anderson, Burford, & Emmerton, 2016; Cline & Luiz, 2013; Mendiola, Kalnicki, & Lindenauer, 2015).
With respect to the challenges associated with the use of the Mobile Renewal Service, it presents the following in order of severity as the main issues: Lack of user understanding of steps involved in using Mobile Renewal Service; Mobile network challenges in renewing insurance premium; Subscriber resistance to switch from the manual renewal method to the mobile renewal service mode; Lack of knowledge and skills to use the Mobile Renewal Service and mobile network challenges in renewing insurance premium. This implies that NHIS subscribers in the study area perceive the afore-stated challenges as major obstacles to the use of the System. This corresponds to prognostications made in the existing literature on new systems (Aljedaani et al., 2020; Peng et al., 2016). Among the main challenges identified by Aljedaani et al. (2020) are inadequate security awareness, little or no security expenditure, lack of participation of security professionals during application development, weak security decisions during the development phase, assumptions about security problems resolved by app testing team, project constraints that break the system, a lack of vulnerability assessments, and the assumption that subscribers are not that concerned about security.
6. Recommendations
The high rate of subscriber awareness of the Mobile Renewal Service, but the low rate of patronage, as reported in this study, suggests that additional considerations are required, as reported in this study. It’s important for policymakers to pay attention to the following factors: system quality, transaction cost, accessibility, perceived ease of use, and perceived usefulness. It is recommended that the National Health Insurance Scheme consider making the mobile payment process as simple as possible for members who are less educated or live in rural areas.
The methodology of the study can be applied in other countries, but only with caution. Qualitative means can be employed to consider service providers’ opinions on implementation challenges.