Surgical Science
Vol.07 No.02(2016), Article ID:63751,7 pages
10.4236/ss.2016.72011
A Modified Three-Port Laparoscopic Cholecystectomy: Shifting the Third Port to the Umbilicus
Jianming Zhu*, Jianping Huang
Department of General Surgery, Shuguang Hospital Affiliated to Shanghai University of traditional Chinese Medicine, Shanghai, China

Copyright © 2016 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 25 January 2016; accepted 22 February 2016; published 25 February 2016
ABSTRACT
Aim: The aim is to shift the
Keywords:
Laparoscopic Cholecystectomy, Port, Modification

1. Introduction
Laparoscopic cholecystectomy is the gold standard for the surgical removal of the gallbladder as it results in a shorter hospital stay, lower levels of postoperative pain, a speedy return to work, superior cosmetic results and significantly lower morbidity rates [1] -[3] . In 1985, Prof. Dr. Erich Mühe of Germany performed the first laparoscopic cholecystectomy (LC). The general indications for laparoscopic cholecystectomy are the same as those for the corresponding open procedure. Although laparoscopic cholecystectomy is originally reserved for young and thin patients, it now is also offered to elderly and obese patients; in fact, these latter patients may benefit even more from surgery through small incisions. Initially, the four-port technique is used, but increasingly this has been replaced by techniques using fewer incisions which are less traumatic and have better cosmetic results [4] .
Given the reliability and safety of this surgical procedure, conventional three-port laparoscopic cholecystectomy is still the primary option in our hospital. Using the conventional method, the right upper port incision is
2. Methods
2.1. Patients
In total, 149 patients underwent laparoscopic cholecystectomy in our Department of Surgery between February 2013 and April 2015. All patients were diagnosed following preoperative abdominal ultrasonography or computerized tomography and underwent the same preoperative processes. All surgical procedures were carried out by a single surgeon who was experienced in laparoscopic surgery. Patients were consented to participate in the research process. This study was approved by the ethics committee of Shuguang hospital affiliated to Shanghai University of Traditional Chinese Medicine (NO.SGH-13075).
Preoperative preparation included a complete history and physical examination, routine laboratory tests and magnetic resonance cholangiopancreatography. Patients with prior upper abdominal surgery, suspected choledocholithiasis, pregnancy, ongoing peritoneal dialysis, pancreatitis, or Mirizzi’s syndrome were excluded from laparoscopic surgery. A history of low abdominal surgery, such as appendectomy, hernia repair, anorectal surgery, uterine or adnexal surgery, was not a criterion for exclusion.
The operating time, intra-operative blood loss, need for conversion to open cholecystectomy, postoperative wound infection, length of hospital stay and satisfaction with cosmetic outcome were recorded. Cosmetic outcome was assessed by patients using a numeric visual analog scale from 1 to 5 (worst to best) on the day of discharge.
2.2. Operative Technique
All procedures were performed under general anesthesia and patients were placed in the standard position for laparoscopic cholecystectomy. After performing two
The difference between the conventional laparoscopic cholecystectomy and the modified laparoscopic cholecystectomy was that one of the
2.3. Statistical Analysis
All statistical analyses were performed using IBM SPSS statics 19.0. Ordinal variables were calculated as me-

Figure 1. Ports position.

Figure 2. Umbilical 5 mm ports.
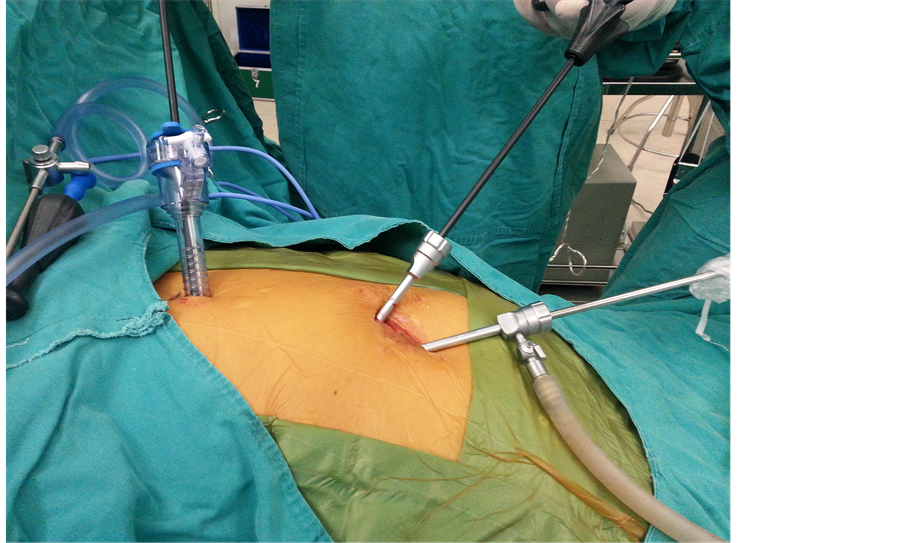
Figure 3. Performing the chelecystectomy.
dian (range) and compared using the Student’s t test. This test was also used to analyze differences in operating time, blood loss, hospital stay and cosmetic outcomes between the two groups. The Chi-square test was used to evaluate the effects of gender, disease history, conversion to open surgery and wound infection. A value of P < 0.05 was considered statistically significant.
3. Results
There were 98 female and 51 male patients. The age range was 24 - 71 years, with a mean age of 48.52 years. Conventional three-port laparoscopic cholecystectomy was performed in 82 patients, while modified three-port laparoscopic cholecystectomy was performed in 67 patients. Twenty-five patients were diagnosed with acute cholecystitis and 124 patients were diagnosed with chronic cholecystitis. Five patients in the conventional group and
Complications such as bile duct damage and massive bleeding were not observed. Two patients in the conventional group and one patient in the modified group were converted to open surgery due to celiac adhesion. There were no apparent differences in blood loss between the two groups. The modified three-port procedure was completed in a similar time to the conventional three-port method.
Four patients developed epigastric wound inflammation which was treated with conservative therapy. No significant differences in wound infection and length of hospital stay were observed between the two groups. Patients in the modified group scored higher than those in the conventional group in terms of cosmetic satisfaction (P < 0.05) (Table 2).
4. Discussion
Although laparoscopic cholecystectomy is initially performed with four incisions, over time there has been a tendency to reduce the number of incisions in order to achieve better cosmetic results [2] [4] .
The primary advantage of a single incision laparoscopic cholecystectomy (SILC) is cosmesis. However, SILC is still a relatively new technique and is more difficult than standard laparoscopic cholecystectomy [3] [4] . Long-term outcomes of SILC have yet to be determined. One of these long-term outcomes is port-site incisional hernia which typically occurs as a late postoperative complication [5] [6] . Laparoscopic surgeons agree that the diameter of the cannula or port is related to the development of port-site incisional hernia [7] -[9] .

Table 1. Patient characteristics.
Table 2. Operative and post-operative data.
*Statistical significance
Natural orifice trans-luminal surgery is introduced by the authors due to its superior cosmetic outcome and technical feasibility [2] [10] . However, this technique is still controversial as it requires a multidisciplinary team, a long and difficult surgical procedure and there are ethical problems related to the trans-vaginal route [2] .
Double incision laparoscopic cholecystectomy (DILC) performed by an inexperienced surgeon is as successful and safe as traditional laparoscopic cholecystectomy [4] [11] . However, two fascial defects converted to a single larger fascial defect more than
Studies have shown that the three-port technique does not change the rate of conversion or increases the operating time when compared to the four-port technique [12] . With the aim of achieving better cosmetic results, we modify the conventional three-port technique. Although there is no reduction in port number, movement of the
The umbilical ports are located at the 2 o’clock and 8 o’clock position, respectively, which may have reduced instrument collision. Both
The specimen is removed via the
When compared with conventional three-port laparoscopic cholecystectomy, a modification of the
In conclusion, movement of the 5 mm port from the right upper abdomen to the umbilicus in conventional laparoscopic cholecystectomy can be performed with acceptable operative outcomes and superior cosmetic results.
Acknowledgements
We thank doctor Yining Xu for his assisitance in surgical operations. We also thank language editor Jingyun Ma for her significant revision of the manuscript.
Competing Interest
We have no conflict of interest to declare.
Authors’ Contributions
Jianming Zhu conceived and designed the study, conducted the analyses, data interpretation and manuscript production. Jianping Huang participated in study design, analytic method design and data interpretation, and approved the final submitted manuscript. Surgical operations were performed by Jiangming Zhu under the guidance of Jianping Huang.
Funding
There was no funding received for this work.
Cite this paper
JianmingZhu,JianpingHuang, (2016) A Modified Three-Port Laparoscopic Cholecystectomy: Shifting the Third Port to the Umbilicus. Surgical Science,07,82-88. doi: 10.4236/ss.2016.72011
References
- 1. Hao, L., Liu, M., Zhu, H., et al. (2012) Single-Incision versus Conventional Laparoscopic Cholecystectomy in Patients with Uncomplicated Gallbladder Disease: A Meta-Analysis. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 22, 487-497.
http://dx.doi.org/10.1097/SLE.0b013e3182685d0a - 2. Pollard, J.S., Fung, A.K. and Ahmed, I. (2012) Are Natural Orifice Transluminal Endoscopic Surgery and Single-Incision Surgery Viable Techniques for Cholecystectomy? Journal of Laparoendoscopic & Advanced Surgical Techniques, 22, 1-14.
http://dx.doi.org/10.1089/lap.2011.0341 - 3. Ahmed, M.U., Aftab, A., Seriwala, H.M., et al. (2014) Can Single Incision Laproscopic Cholecystectomy Replace the Traditional Four Port Laproscopic Approach: A Review. Global Journal of Health Science, 6, 119-125.
http://dx.doi.org/10.5539/gjhs.v6n6p119 - 4. Sabuncuoglu, M.Z., Benzin, M.F., Cakir, T., et al. (2014) Triple, Double- and Single-Incision Laparoscopic Cholecystectomy: A Prospective Study. International Journal of Clinical and Experimental Medicine, 7, 3385-3391.
- 5. Marks, J.M., Phillips, M.S., Tacchino, R., et al. (2013) Single-Incision Laparoscopic Cholecystectomy Is Associated with Improved Cosmesis Scoring at the Cost of Significantly Higher Hernia Rates: 1-Year Results of a Prospective Randomized, Multicenter, Single-Blinded Trial of Traditional Multiport Laparoscopic Cholecystectomy vs Single-Incision Laparoscopic Cholecystectomy. Journal of the American College of Surgeons, 216, 1037-1047.
http://dx.doi.org/10.1016/j.jamcollsurg.2013.02.024 - 6. Alptekin, H., Yilmaz, H., Acar, F., et al. (2012) Incisional Hernia Rate May Increase after Single-Port Cholecystectomy. Journal of Laparoendoscopic & Advanced Surgical Techniques, 22, 731-737.
http://dx.doi.org/10.1089/lap.2012.0129 - 7. Zemet, R., Mazeh, H., Grinbaum, R., et al. (2012) Incarcerated Hernia in 11-mm Nonbladed Trocar Site Following Laparoscopic Appendectomy. JSLS, 16, 178-181.
http://dx.doi.org/10.4293/108680812X13291597716780 - 8. Yamamoto, M., Minikel, L. and Zaritsky, E. (2011) Laparoscopic 5-mm Trocar Site Herniation and Literature Review. JSLS, 15, 122-126.
http://dx.doi.org/10.4293/108680811X13022985131697 - 9. Bunting, D.M. (2010) Port-site Hernia Following Laparoscopic Cholecystectomy. JSLS, 14, 490-497.
http://dx.doi.org/10.4293/108680810X12924466007728 - 10. Solomon, D., Shariff, A.H., Silasi, D.A., et al. (2012) Transvaginal Cholecystectomy versus Single-Incision Laparoscopic Cholecystectomy versus Four-Port Laparoscopic Cholecystectomy: A Prospective Cohort Study. Surgical Endoscopy, 26, 2823-2827.
http://dx.doi.org/10.1007/s00464-012-2253-0 - 11. D’Antonio, D., Franzato, B., Fusco, G., et al. (2013) Double Incision Laparoscopic Cholecystectomy (DILC) with Routinary Intra-Operative Cholangiography (IOC): Less Trauma, Same safety. Report on 30 Consecutive Non-Selected Cases. Updates in Surgery, 65, 109-114.
http://dx.doi.org/10.1007/s13304-013-0200-9 - 12. Al-Azawi, D., Houssein, N., Rayis, A.B., et al. (2007) Three-Port versus Four-Port Laparoscopic Cholecystectomy in Acute and Chronic Cholecystitis. BMC Surgery, 7, 8.
http://dx.doi.org/10.1186/1471-2482-7-8 - 13. Freimann, F.B, Ötvös, J., Chopra, S.S., et al. (2013) Differential Pressure in Shunt Therapy: Investigation of Position-Dependent Intraperitoneal Pressure in a Porcine Model. Journal of Neurosurgery: Pediatrics, 12, 575-581.
http://dx.doi.org/10.3171/2013.8.PEDS13205
List of Abbreviations
SILC: Single incision laparoscopic cholecystectomy
DILC: Double incision laparoscopic cholecystectomy
NOTES

*Corresponding author.