Health
Vol. 4 No. 2 (2012) , Article ID: 17482 , 14 pages DOI:10.4236/health.2012.42012
An epidemiological study on delay in treatment initiation of cancer patients
![]()
1Center for Biostatistical Services, Division of Biostatistics and Epidemiology, Department of Environmental Health, College of Medicine, University of Cincinnati, Cincinnati, USA; *Corresponding Author: dwivedak@ucmail.uc.edu, alok_bhu1@yahoo.co.in
2Department of Biostatistics, All India Institute of Medical Sciences, New Delhi, India
3Department of Surgical Oncology, All India Institute of Medical Sciences, New Delhi, India
4National Institute of Medical Statistics, Indian Council of Medical Research, New Delhi, India
5Department of NMR & MRI Facility, All India Institute of Medical Sciences, New Delhi, India
Received 25 October 2011; revised 29 November 2011; accepted 7 December 2011
Keywords: Delay; Cancer; Log Gamma Regression; Quantile Regression
ABSTRACT
Early diagnosis and timely initiation of treatment of cancer patients may improve survival and quality of life. Various measures of delay can be made during diagnosis and treatment initiation. Most of the studies were based on single type of cancer with different definitions and measurements of delay in diagnosis and treatment. Thus, it has been difficult to synthesize results and generalize to other types of cancer. The study proposes to measure total duration between onsets of symptom to start of treatment into three components, namely primary, secondary and tertiary delays. Primary delay is defined as onset of symptoms to contacting the first medical person, secondary delay is from first medical contact to confirmed diagnosis, and tertiary delay is from confirmed diagnosis to treatment initiation. The aim of this study is to determine factors associated with primary, secondary and tertiary delays in cancer patients. This study was planned as a cross-sectional study. Data was collected from patients admitted to the surgical wards of Department of Surgical Oncology, Institute Rotary Cancer Hospital, New Delhi during 2006-2007. Gamma regression and quantile regressions at 25th, 50th and 75th percentile of each of the delays were used to determine related factors. A total of 403 patients were included in the analysis. The median tertiary delay was found almost two folds (59; Interquartile range: 26 - 101 days) than the primary and secondary delays. Extremity cancer patients had longest primary, secondary and tertiary delays. Shortest primary, secondary and tertiary delays were observed for gastrointestinal cancer, breast and genitourinary cancer respectively. There is an urgent need and scope to reduce delay at each level primary, secondary and tertiary delay. Intervention studies are needed through information, education and communication/screening programs to reduce the diagnostic and treatment delays in cancer patients.
1. INTRODUCTION
Cancer is one of the most leading causes of death in many countries despite the advancement in cancer treatment and diagnosis [1]. One of the main reasons for this is delay in diagnosis or initiation of treatment at advanced stage [2]. Prolong duration of diagnosis and treatment may increase the proportion of advanced stages in cancer patients [3,4]. Thus, delay in diagnosis and treatment of cancer patients may impact on poor prognosis and quality of life [5-7]. Various studies have been conducted to measure delay in diagnosis and treatment initiation. Different types of delay can occur in total duration from onsets of symptoms to start of cancer treatment. Thus, numerous measurements of delay can be made in total duration. Previous studies differ with different definitions of delay and different measurements of delay in total duration [2] and are thus, inconsistent. As a result, it has become difficult to draw meaningful information from these studies. Only few studies were carried out on more than one organ specific cancer that can provide similarity and differences about delays across different types of cancers in one study. There is a need of a study on different types of cancer to provide clear picture of delays so that results can be generalized [8].
Dividing total duration into two components has been clearly understood by the researchers. Primary delay is defined as duration between onset of symptoms to first presentation to clinician. Next, clinician delay covers from first presentation to clinician until start of treatment [9]. This definition of primary delay has been found to be consistent in literatures. Primary delay has been referred to as patient delay since it is mainly influenced by the patients’ characteristics. One study referred this delay as evaluation time [10]. Clinician delay may not only influence by patient’s characteristics but it may also associate with doctor and system related factors. Thus, clinician delay is clearly considered as a separate process from primary delay. Criteria for measuring clinician delay have been varying across the studies. Some studies measured clinician delay from first presentation to reaching secondary care center; some up to diagnosis; and some even up to starting treatment. Further, each of these considerations have either been addressed by different names or defined further in shorter durations [11-17]. We suggest time at diagnosis is an important level in clinician delay that may change the process of subsequent delay. Thus, we propose to define total delay into three components to assess factors associated with total delay. First, primary delay is defined as the time from the onset of symptoms to first contact with medical persons. Second, secondary delay is defined as the time from contacting the first medical person to a confirmed diagnosis. Third and last, tertiary delay is defined as the time from a confirmed diagnosis to the start of treatment. If we model diagnostic delay to be defined as the time from the onset of symptoms to a confirmed diagnosis (i.e., the sum of primary and secondary delays), clinician delay to be defined as the time from the date of a confirmed diagnosis to the start of cancer treatment (i.e., sum of secondary and tertiary delays), and total delay to be defined as the time from the onset of symptoms to the start of treatment, then we may not be able to capture all the factors associated with delays. Here we show the advantages of defining clinician delay into two components (secondary and tertiary delays). Figure 1 shows the schematic diagram and conceptual framework of primary, secondary and tertiary delays in cancer patients.

Figure 1. Schematic diagram and conceptual framework of primary, secondary and tertiary delays in cancer patients.
There are numerous studies for estimating delay in diagnosis and initiation of treatment but very limited studies aimed to assess the factors associated with each component of delay. Most of the studies were focused upon organ specific cancer [8]. In recent years, several groups have given attention to identify factors associated with delays and their impact on cancer outcomes. A recent review indicates more work is needed to reduce delay in diagnosis of cancer [2]. Either socio-demographic characteristics or strictly psychological factors of the patients are mainly considered for primary delay [18-21]. Primary delay may be associated with patient related characteristics such as no accompanying person, lack of time, or family related problems. Clinicians and tumor related factors are being examined for secondary and tertiary delays [11,14,22-23]. However, patient related factors may also be associated with secondary or tertiary delay [24-26]. Studies dealing with tumor related factors associated with delays might not be of much relevance because these results might be the consequence of delays. A recent review indicates that no study has considered patient and clinician related factors together to assess association with clinician delay in common cancer patients [8]. There is also scarcity in the literatures from developing countries. As such, no study exists from India that provides an estimate for various levels of delay and their associated factors in cancer.
There is no consensus on an acceptable length of delay from diagnosis to the start of treatment in cancer patients. Studies often categorized delays to use simple regression models that obviously lose the information especially in absence of optimum time to define such delays [27-30]. Delay data in nature involves a positively skewed distribution even after exploring various transformations to achieve induced normality. No single study has attempted to use appropriate distribution to describe such delays in cancer patients. Due to different definitions of delay, their measurement and analytical procedures, it is more likely to get conflicting findings in estimating and assessing factors associated with such delays. Thus, we conducted a single planned study to measure total duration into three components primary, secondary and tertiary delays and assess their associated factors.
2. MATERIALS AND METHODS
2.1. Subjects
The study was planned as a cross-sectional study. The patients included in the study were newly registered indoor cancer patients admitted to surgical oncology wards during June 2006 to November 2007 at Institute Rotary Cancer Hospital (IRCH), All India Institute of Medical Sciences (AIIMS), New Delhi, India. Patients with any evidence of recurrence were excluded. Patients who could not receive any form of treatments (surgery/chemotherapy/ radiotherapy) before getting discharged from the surgical ward were also excluded. As approximately 80% of the solid tumors go for upfront surgery, data collection was done in surgical wards to avoid missing data for treatment initiation. Patients who consented to participate in the study were interviewed in the presence of one family member/relative who knew the entire referral pattern of the patients.
2.2. Variables and Data Collection
After pre-testing on few subjects, a semi structured questionnaire was used to collect data which includes three sections. First, a primary delay section where the patients were asked one question for primary delay, “What was the time taken from the onset of symptom to first contacting medical person?”. Next, in the secondary delay section, the patients were asked for details regarding delay between first contacting a medical person until diagnosis. These details included information on place of contact, whether a diagnosis was made, and if yes, which diagnostic procedures were done and what any treatment(s) (if any) were received before appropriate diagnosis. Patients were also asked about the possible reasons for such delay. In the case of a final diagnosis, by adding the time spent from contacting the first medical person until final diagnosis provided an estimate of secondary delay. In the tertiary delay section, the details related to each contact made starting from date of diagnosis until the commencement of appropriate cancer treatment was also recorded. Obviously, by summing the time spent between final diagnosis and commencement of treatment provided tertiary delay. Further, cross check was made for available durations from the respective patient’s file.
After exploratory analysis, only one continuous explanatory variable age (in years) was retained in their original form. The categorical variables retained in their original forms were sex (female/male); residential area (urban/ rural); family structure (nuclear/joint); and family history of cancer (yes/no). To enable a meaningful analysis, some of the categorical variables were modified based on theoretical and statistical consideration such as education (graduate & postgraduate/higher & secondary/less than and middle school/illiterate), religion [(Hindu/Muslim/ Sikh or Christian as Other], marital status (married/ separated or single/widower or widowed), patients relationship with the head of family (self/other), occupation (nonworker/worker); stage (early/advanced); and type of cancer (gas-trointestinal tract/breast/genitourinary/extremity/ head and neck/miscellaneous). Some of the variables were generated with the help of other variables. For example, patient who took the advice of any non-medical person prior to contacting first medical person (i.e., patients received treatment/advice with family members/ relatives or paramedical or quacks before contacting first medical person) were classified as contacting non-medical person prior to first medical person (no/yes). Further, multiple responses of the open question “what was the reason of primary delay (i.e., availing time duration from onset of symptom to first medical contacts)?” were transformed in to various covariates like fear of cancer/diagnosis (yes/no); no body to accompany for medical aid (yes/no); lack of time to seek medical help (yes/no); lack of awareness/ self-limiting disease/ignorance (yes/no); distance problem (yes/no); economical problem(yes/no); and family related problems (e.g., marriage, pregnancy, childbirth, death, examinations, sickness of some person in family etc.) as (yes/no). Similarly, multiple responses to open question “what was the reason of availing time between each of the contacts?” under the secondary and tertiary delays were also transformed into similar covariates as described under primary delay. Some additional variables considered based on qualitative analysis for tertiary delay were doctor assurance (i.e., doctor assured to the patients that he/she may receive cancer treatment after some time period or no major problem) as (yes/no) and exploration for better place in treatment as exploration (yes/no). Some of the variables were generated with the help of more than one variable such as misdiagnosis (i.e., other than the cancer diagnosis was made up at any of the contacts before confirmed diagnosis) as (yes/no); symptomatic treatment before diagnosis (i.e., any treatment was given before the confirmed diagnosis of cancer at any of the contacts) as (yes/no); previous inadequate treatment {i.e., any treatment that is not adequate for cancer (other than surgery, radiotherapy or no complete surgery) after making diagnosis as cancer was given to patients at any of the visit to doctor, as mentioned on the patients’ file by the concerned clinician} as (yes/no); referral (i.e., the patients got diagnosed with cancer and got referral for other contacts as (yes/no); number of contacts made to medical person (including first medical contact) until diagnosis (1/2/3+); and number of contacts made to medical person after diagnosis (0 - 1/2/3+).
2.3. Statistical Analyses
Delay was measured in days and described using various summary statistics; mean, median, standard deviation (SD), inter-quartile range (IQR) and range. All of the qualitative variables are presented using frequency and proportions whereas quantitative variables are summarized using mean and SD. Delays were compared according to stage and types of cancer using t-test and one-way analysis of variance respectively. Primary, secondary and tertiary delays revealed a positively skewed distribution even after exploring a log transformation. Thus, the log gamma regression under a generalized linear regression model (GLM) was used to assess the factors associated with each of the delays. Box Cox regression was used to identify the link function for the GLM. Park test was used to determine the family distribution under the GLM for each of the delay. Modified Hosmer Lemshow test was carried out to assess the goodness of fit of the developed regression model. Finally, a residual plot was constructed between the deviance residuals and predicted delay transformed to constant variance. Residuals were randomly scattered and lie within (–2, 2) range which provides an indication of good fit of the model [31]. Log gamma regression is a parametric regression and provides the prediction of mean of the logarithmic delay. Since delay distribution is heavily skewed, the median would be a better summary statisticsthan the mean. Thus, median regression (special case of quantile regression) was also used to assess the factors associated with each of the delays. Further, to assess the effect of cofactors on the entire distribution of each of the delays, lower quartile (i.e., 25th) and upper quartile (i.e.,75th) of the log transformed delay was also modeled separately for each of the delays. In the quantile regressions, standard errors were obtained using bootstrap method with 300 replications. Univariate regression analysis was carried out using both approaches (gamma and quantile regressions) for each of the delays. A common set of variables were selected which emerged significant (at 0.05 level of significance) in any of the univariate regression models used for the development of multivariable log gamma and quantile regression for each separate delay. Pregibon’s link test was used to assess the linearity assumption in the model. First order interaction effect was also explored for some of the important cofactors before development of the model. Multicollinearity was also assessed by estimating a variance inflation factor (VIF) through an ordinary least square regression. VIF as 10 or higher indicates the presence of multicollinearity. Exploratory analysis revealed no presence of multicollinearity and interaction effects. Multivariable results obtained from log gamma and quantile regression analyses are presented using adjusted coefficient (ARC) with 95% confidence interval (CI). Results are considered to be significant at 5% level of significance. STATA 10 was used to conduct the analysis.
3. RESULTS
Out of total 403 patients, 60% of patients were females. Mean age of the patients were 48.3 (SD: 14.3 years and range: 14 - 85). Most of the patients were Hindu (86.4%) and from urban areas (67.7%). Most of the patients (79.9%) were married. Only one patient had separated marital status. Twenty six percent of the patients were not the head of the family. Fifteen percent of the patients reported family history of cancer. Most of the patients (64.5%) were not found to be working. More than one third of the patients had breast cancer (35.2%) followed by gastrointestinal tract (18.6%), head & neck (18.4%), genitourinary (10.9%), extremity (8.4%) and miscellaneous (8.4%).
Median total delay was observed as 194 (IQR: 112, 370) days. The median tertiary delay (IQR) was found to be almost twice (59; IQR: 26, 101 days) that of primary (30; IQR: 3, 120 days) and secondary (33; IQR: 8, 124 days) delays (Table 1). Figure 2 reveals the comparison of delays according to organ specific cancers. Extremity cancer patients had maximum primary, secondary and tertiary delays. Patients with gastrointestinal cancers had the minimum primary delay followed by genitourinary, breast, head and neck and extremity cancer patients. Secondary delay was observed to be minimum for breast cancer followed by genitourinary, gastrointestinal tract, head and neck and extremity cancer patients. Tertiary delay was observed to be minimum for gastrointestinal tract followed by breast, head and neck, genitourinary and extremity cancer patients. Patients presented to the hospital were mostly in the advanced stages of cancer (73.5%). The lump/swelling was the most common symptom at presentation (15.9%). The ulcer and pain were equally prevalent. There was no correlation observed among primary, secondary and tertiary delays. A comparison of primary, secondary and tertiary delays according to clinical stage of the cancer reveals that only the secondary delay was higher in advanced stage patients as compared to patients with lower stage (p = 0.003).
The lack of awareness (54.6%) was the most common of factors reported for primary delay. Economical problem (12.4%) and lack of time (9.7%) were also reported to be important covariates. Fear of cancer was reported by only 3.5% of the patients while 9% of the patients got delayed in contacting to first medical person due to nonpresence of accompanying person. The factors such as distance, economical and family related problems were observed among 4.5, 12.4 and 8.7% of the total patients respectively. More than 30% of the patients made three or more medical contacts until their confirmed diagnosis whereas 22% of the patients contacted three or more medical persons after getting diagnosed through the start of treatment. The most common patients related factors reported for secondary delay were number of contacts until diagnosis (median 2; range: 1, 8), economical problem (10.4%), distance (10.2%) and then lack of awareness (9.4%). However, the major non-medical related factors reported for tertiary delay were number of contacts after diagnosis (median 4; range: 1 - 10), exploration (11.2%), and economical problem (10.4%).The medical factors recorded for secondary delay include doctors making an inappropriate diagnosis among 27.5% of the patients and symptomatic treatment before their confirmed diagnosis among more than 50% of the patents. Related with tertiary delay, 11% of the patients were treated inadequately before their start of proper treatment. One third of the patients reached to this tertiary hospital without taking referral. Further, more than 7% of the patients got assurance by the concerned doctor that they may receive their treatment later on or their disease is not a matter of serious concern. Nearly one fourth of the patients contacted medical person for the first time at specialized health centers. More than 60% of the patients contacted primary health centers. Few

Table 1. Summary of delays and validity Indices related to log gamma regression model for each of the delay.
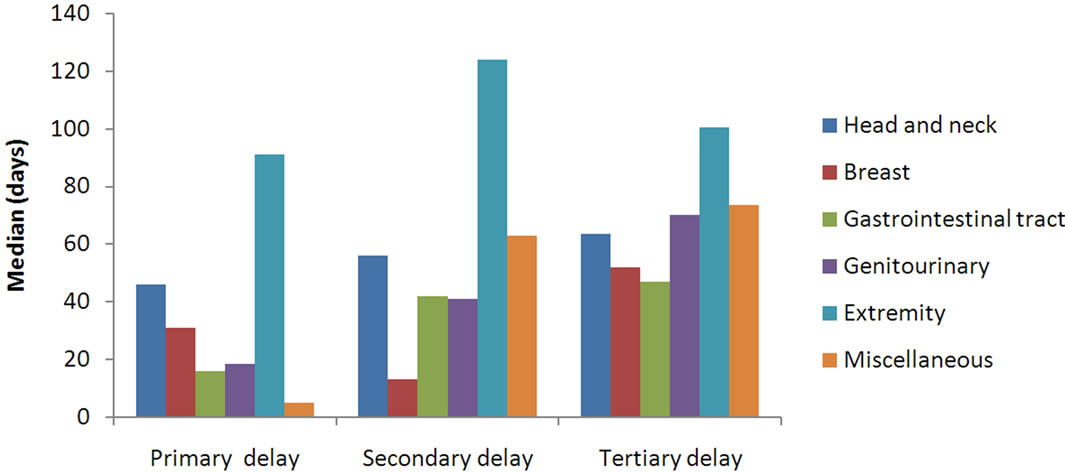
Figure 2. Primary, secondary and tertiary delays according to types of cancer patients.
patients (8%) took a first opinion from alternative medicine practitioners. Almost half of the patients were diagnosed at the specialized centers. At this tertiary center, 16.7% of the patients were confirmed diagnosed with cancer.
In the univariate analysis of primary delay, residential area, types of cancer, contacting non-medical person prior to medical person, lack of awareness, economical problem and family related problems were found to be associated with median, first quartile and third quartile of logarithmic primary delay. In addition, education status of the patient was found to be associated with median primary logarithmic delay and lower quartile of logarithmic primary delay. Fear, nobody to accompany for medical aid problems, lack of time, distance, were found to be associated with lower level of primary delay. These factors except education and no availability of accompanying person remained significant for mean of logarithmic primary delay. In addition, sex was also found to be associated with mean of logarithmic primary delay. Multivariable analysis revealed that residential area, types of cancer, contacting non-medical person prior to medical person, lack of awareness, economical problem and family related problems were found to be associated with mean of logarithmic primary delay after adjusting other significant cofactors from univariate analysis. Among these variables, contacting non-medical person prior to medical person, lack of awareness and economical problem were associated with entire range of the primary delay distribution. However, family related problem and type of cancer were found to be associated with median and higher level of primary delay only (Table 2).
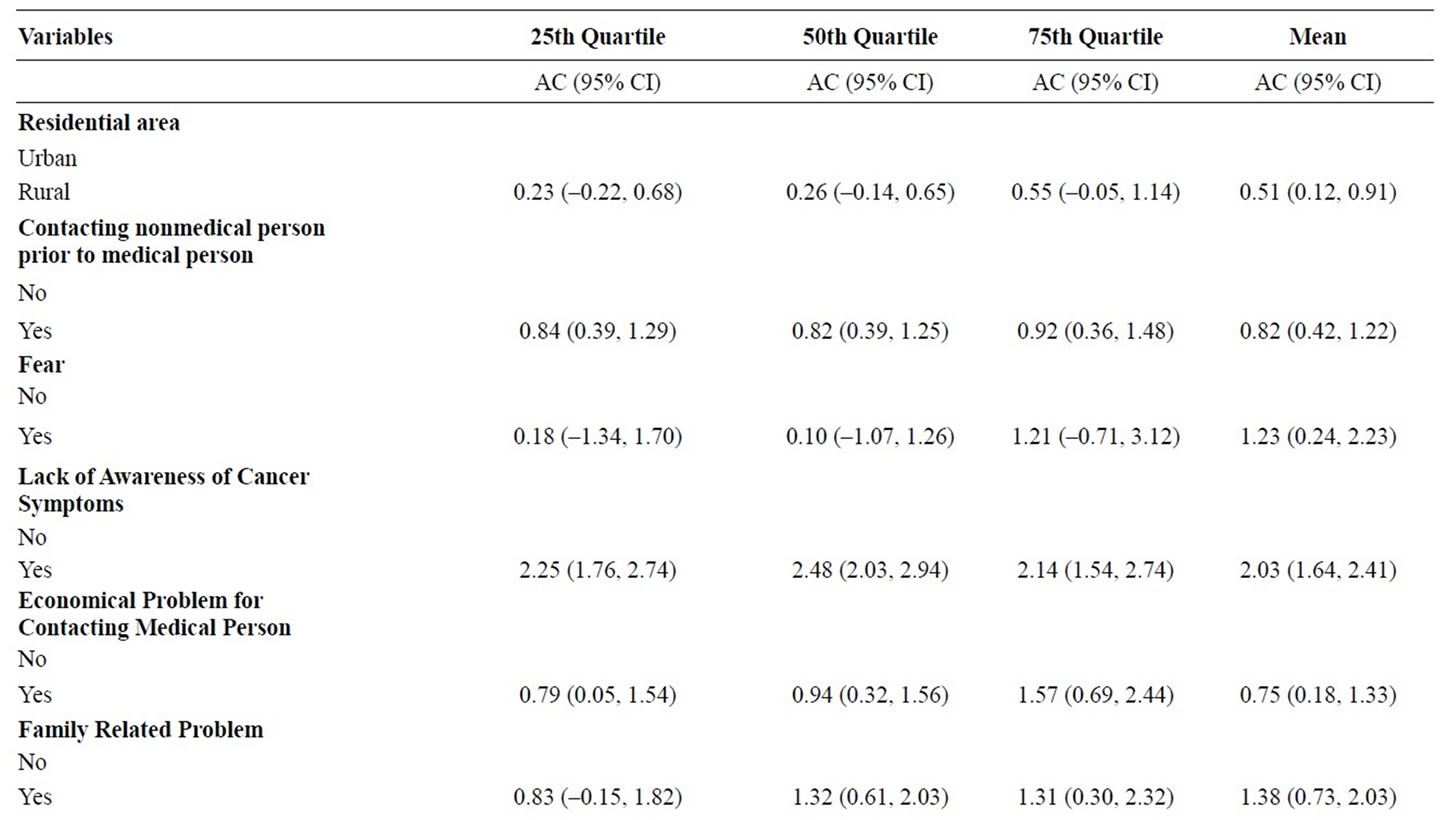

Table 2. Adjusted coefficients (with 95% CI)* using multiple quantile regression and gamma regression analysis of log primary delay (days) in relation to considered covariates.
Table 3 reveals that types of cancer, number of times contacting medical persons until diagnosis, lack of awareness, misdiagnosis and symptomatic treatment before diagnosis were found to be associated with entire range of logarithmic secondary delay (mean, median, first quartile and third quartile) in the univariate analysis. In addition, sex was also found to be associated with the mean of log transformed secondary delay. This variable was also associated with median and higher quartile of log transformed secondary delay. Age of the patient was found to be associated with median and higher logarithmic secondary delay whereas family structure and distance were only associated with lower quartile of logarithmic secondary delay. Economical problem was associated with the higher quartile of logarithmic secondary delay and mean of the logarithmic secondary delay. Among these cofactors in multi-variable analysis, only number of contacting medical persons till diagnosis was found to be associated on entire range of secondary delay. Misdiagnosis was found to be associated with mean of log secondary delay only. Symptomatic treatments before diagnosis was only associated with lower quartile of logarithmic secondary delay. Median, higher quartile and mean of log secondary delay were also found to be higher for those patients who reported economical problem. Patients reported lack of awareness was found to be associated with lower and higher quartile of logarithmic secondary delay. Patients with extremity cancer had higher median and mean of logarithmic secondary delay whereas head and neck cancer patients had significantly higher mean of logarithmic secondary delay as compared to genitourinary cancer patients after adjusting other cofactors.

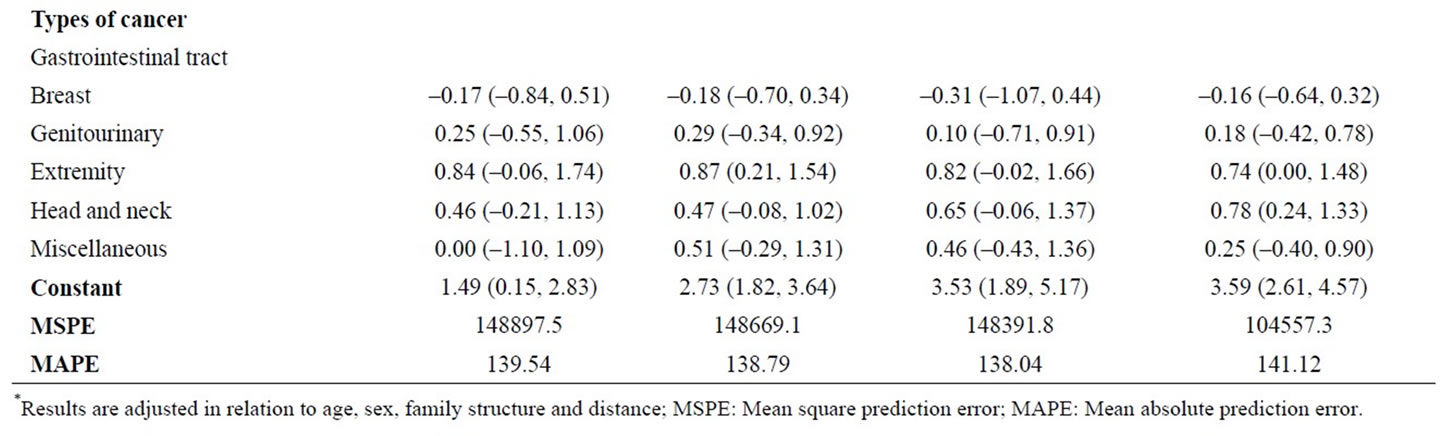
Table 3. Adjusted coefficients (with 95% CI)* using multiple quantile regression and gamma regression analysis of log secondary delay (days) in relation to considered covariates.
Table 4 shows the results related to tertiary delay. In univariate analysis, logarithmic tertiary delay was found to be associated with patient head, type of cancer, lack of awareness, fear, number of made contacts between diagnosis and treatment, inadequate treatment and doctor assurance. Among these factors, fear, type of cancer, and number contacts between diagnosis and treatment were found consistently to be associated with all the three quartiles of log tertiary delay. Inadequate treatment and patient head factor were associated with only lower quartile of log tertiary delay. Those patients who reported lack of awareness of cancer had longer median log tertiary delay. In addition to these factors, sex was found to be associated with median and higher quartile of tertiary delay and referral was found to be associated with lower and higher delay. Some of the factors such as education, economic and no accompaniment for medical aid were found to be associated with lower quartile and median log tertiary delay. However, sex, education, number of made contacts, previous inadequate treatment, fear, doctor assurance and type of cancer were remained significant after adjusting other cofactors in multivariable analysis. Patient’s educational status and number of made contacts were found to be associated with entire range of the tertiary delay. Previous inadequate treatment was found to be associated with 25th quartile, 75th quartile and mean of the log transformed tertiary delay. Type of cancer and patient reported fear of the cancer treatment were associated with mean, median and 75th quartile of log transformed tertiary delay. However, doctor assurance was only found to be associated with mean of the log transformed tertiary delay. Male patients had longer upper level of tertiary delays than the females.


Table 4. Adjusted coefficients (with 95% CI)* using multiple quantile regression and gamma regression analysis of log tertiary delay (days) in relation to considered covariates.
Median diagnostic and clinician delays were found to be 107 (IQR: 40, 273) and 117 (IQR: 69, 236) days respectively. The results related to diagnostic delay (sum of primary and secondary delays), clinician delay (sum of seconddary and tertiary delays) and total delay using gamma regression are shown in Table 5. The analysis of diagnostic delay does not capture all the significant factors associated with primary and secondary delays. The combined analysis of secondary and tertiary delays as clinician delay does not retain the same factors obtained under separate analysis of secondary and tertiary delays. Some of the significant factors for tertiary delay such as inadequate treatment, education and number of made contacts after diagnosis could not obtain in the analysis of clinician delay. It indicates that there is need to consider tertiary delay separately from clinician delay. As obvious, analysis of total does not provide all the factors associated with primary, secondary and tertiary delays.
Box Cox regression showed that log link as the best link function under GLMs for primary delay, secondary and tertiary delays. Under Park test, the estimated regression coefficients were 2.06, 2.03 and 2.30 for primary, secondary and tertiary delays respectively. These coefficients were not found to be statistically significant different than 2 indicating use of gamma regression as appropriate for each of the delays. Accordingly, the log gamma regression models were used for each of the delays. The Hosmer Leme show (HL) test revealed that there is presence of systemic pattern (p < 0.001) but not for secondary (p = 0.64) and tertiary delays (p = 0.44) (Table 1). The


Table 5. Adjusted coefficients (with 95% CI) using gamma regression analysis.
standardized deviance residual plots against predicated value of primary, secondary and tertiary delays on constant scale showed that all the points are scattered and most of them are found to be in range (–2, 2) indicating the good fit of the log gamma regression. Comparisons of log gamma model with quantile regression models were done using mean square prediction error (MSPE) and mean absolute prediction error (MAPE). Both errors were found to be higher for log gamma regression as compared to any of the used quantile regression models favoring the use of quantile regressions in case of explaining primary delay in relation to considered covariates. However, for secondary delay, MSPE was found to be minimum using log gamma regression as compared to quantile regressions but MAPE was found to be slightly higher for this delay using log gamma regression. Both MSPE and MAPE were found to be minimum for tertiary delay using log gamma regression as compared to quantile regression.
4. DISCUSSION
Early diagnosis of any cancer has become one of the primary goals under various cancer control programs worldwide. Screening programs to reduce the diagnostic delay are only amenable for some of the cancers [32]. Thus, identifying the important cofactors that can be modifiable through appropriate intervention programs related to delay would not only reduce delays in diagnosis but also minimize time in initiating treatment. It is now a well-recognized problem that studies differ in general with study designs including different definitions of delays, measurements of delays, considered cofactors for delays, analytical procedures and reporting the study findings [8]. No study has aimed to estimate various delays and their associated non-medical and medical factors in common cancer patients.
In this study, we tried to define the time involved from onset of symptoms to start of appropriate treatment in three components; primary, secondary and tertiary delays. Delays may be defined appropriately upon the data generation process. The data generation for primary delay is completely separate process than any other delays in the total duration. This delay is solely associated with patient’s characteristics. Further, after contacting first medical person until diagnosis of cancer (secondary delay), the data generation process remains same and heterogeneity of this period may be explained by patient, doctor and system related characteristics. Once the patients get diagnosed, the data generation process may change. The date of diagnosis works like exposure that may change the distribution of further delays. Timing in initiating treatment and the speed of the referral process may depend on the stage of the cancer at diagnosis, biology of tumor behavior, patients understanding about severity of disease as well as some other patient, doctor and system characteristics [33]. Thus, statistically, as well as clinically, studies identifying factors associated with diagnostic delay [28,34,35] or clinician delay [17,36] or total delay [30] may not be appropriate. In other words, studies identifying factors associated with delay including secondary delay may not provide appropriate cofactors associated with treatment delay. To study the factors associated with diagnosis or treatment delays, the total symptom duration needs to be considered as three components. We also showed in the present study that analyzing diagnostic delay, clinician delay or total delay may not be able to provide all factors associated with primary, secondary and tertiary delay. Any other rationale may be possible to divide these components into shorter intervals. However, there is a need to make recommendation to define various delays in total duration to study the factors related with delays in diagnosis and treatment and their impacts on cancer outcomes. This will help in combining and generalizing the results from various studies. In the absence of established cut offs for these components of total duration, it should be recommended to consider an original measure of these delays.
Approximately 194 days (6.5 months) of total delay suggests that there is a need to make faster diagnostic process and initiation of cancer treatment. Estimated tertiary delay was found to be longer than the primary and secondary delays that are obvious at the tertiary hospital in the present study because patients tend to search through the hospital to get all possible treatments. At this hospital, patient first review for confirmatory diagnosis. This extends delay in getting treatment. Also, due to burden of the patient at this hospital, patients get further delay in start of treatment. This indicates there is a need to set up more specialized centers for cancer treatment to the community. Inherently, primary delay was found to be longer for outer organ specific cancers than the inner organ cancers. Secondary delay was shortest for breast cancer patients because of a straight forward presentation of signs and symptoms and simpler and easily available diagnostic procedures. Total delay was associated with advanced stage of cancer [37]. In the total delay, only secondary delay was found to be associated with advanced stage of cancer. Tertiary delay was found twice of this period. This in directly indicates that delays may matter for survival and quality of life.
The median primary delay in the present study was observed as 30 (IQR: 3, 120) days. This is slightly higher than a recent study reported the median primary delay as 21 (IQR: 7, 56) days [19]. Most of the existing studies dealt with organ specific cancer and reported varied primary delay across the studies. For example, the median primary delay varied from 30 days to 900 days in head and neck cancer [20,38-39]; 9 days to 35 days in breast cancer [29,37]; 10 days to 46 days in thorax cancer [12,37,40,41]; 8 days to 157 days in gastrointestinal tract [4,15,37,42-44]; 10 days to 14 days in genitourinary [29,45] and 10 days to 14.8 months in soft tissue sarcoma patients [37,46].In the present study, the median primary delay for head and neck cancer patients was observed as 46 (IQR: 16, 153) days; 31 (IQR: 5, 121) days for breast cancer; 16 (IQR: 3, 76) days for gastrointestinal tract; 18.5 (IQR: 3.5, 104.5) days for genitourinary and 91 (IQR: 13, 181) days for extremity cancers. To our knowledge, no study has beenreported to estimate primary delay among irrespective of organ specific cancer patients using its original form in India. Most of the earlier studies used to describe the primary delay either using logistic model or using ordinary linear regression model. However, both approaches seem to be inappropriate especially in absence of proper cut off of primary delay under logistic model and distribution of its original structure under ordinary linear regression model. Under distributional assumption, log gamma regression was found to be appropriate. This regression approach assumes that the primary delay should be strictly positive. However, in the present study, primary delay consists some zero observations (i.e., no primary delay) due to presentation of asymptomatic patients to the medical person. The frequency of patients at zero delays was quite less in the dataset. Comparative results reveal that quantile regressions seem to be more appropriate in case of describing log primary delay. However, combined results obtained under both models may provide better understanding regarding its policy implications. The results were found to be consistent except few exceptions. The factors such as residential area, contacting non-medical personprior to first medical person, fear, lack of awareness, economical problem, family related problem and types of cancer were found to be associated with primary delay. Quantile regression provided additional information such as these factors remained significant for higher level of primary delay except residential area. Similar results were obtained in another study for primary delay. The reported factors were lack of information about cancer, patient education and financial considerations related with this delay [21]. There may be need of Information Education and Communication (IEC)/intervention programs to make community aware about common sign/symptoms related to all cancers as well as they may be counseled/educated towards the need of early reporting of symptom to doctor/ referral centers. The economical problem may be reduced by facilitating through more free health checkup as well as specialized treatment providing centers to the community. There is a need to educate the community towards hazards related to the late diagnosis over other major family related problems to reduce primary delay. To minimize primary delay, genitourinary cancer, extremity and head and neck cancer patients may be targeted through imparting symptoms awareness or using screening program related to these types of cancer.
The median secondary delay observed under the present study was 33 (IQR: 8, 124) days. To our knowledge, none of studies has examined secondary delay as considered in the present study. The median secondary delay was reported as 36 days in head and neck cancer [39], 7 days to 28 days in breast cancer [29,36], 65 days in thorax [12], 0 days to 21 days in gastrointestinal tract [15,43]. In the present study, the median secondary delay for head and neck cancer patients was observed as 56 (IQR: 22, 190) days; 13 (IQR: 5, 60) days for breast cancer; 42 (IQR: 13, 124) days for gastrointestinal tract; 41 (IQR: 7.5, 167) days for genitourinary and 124 (IQR: 30, 246) days for extremity cancers. MSPE was found to be minimum for secondary delay using log gamma regression as compared to quantile regressions whereas MAPE was slightly higher for log gamma regression. In view of advantages of mean modeling over other location modeling, use of log gamma regression may be preferred in describing secondary delay. However, use of both approaches simultaneously may provide additional information in describing factors associated with entire range of the secondary delay distribution. In summary, the non-medical factors such as number of contacts made till diagnosis, lack of awareness, economical problem and types of cancer whereas under medical factor misdiagnosis and symptomatic treatment before cancer diagnosis were related with secondary delay. Quantile regression provided additional information such asnumber of contacts made till diagnosis, lack of awareness and economical problem were associated with prolong secondary delay. To reduce secondary delay, there may be need of IEC/intervention programs not to make community more aware about cancer related information only but also to get the doctors more updated towards making confirmatory diagnosis of cancer. The focus should preferably be on head and neck cancer and extremity cancer patients making them educated about sign and symptoms as well as doctors related to its accurate diagnosis.
Median tertiary delay was observed as 59 (IQR: 36, 101) days. The other studies dealing with organ specific cancer, median tertiary delay reported as 7 days to 8 days in gastric cancer [4,15,43] and 26 days in genitourinary [47]. In the present study, the median tertiary delay was 47 (IQR: 27, 80) days for gastrointestinal tract; 70 (IQR: 40.5, 110.5) days for genitourinary cancers. The non-medical factors such as sex, education, number of contacts made after diagnosis, fear and types of cancer and medical factors such as previously received inadequate treatment and doctor’s assurance were found to be associated with tertiary delay. There is a need to make community aware about need of in time treatment as well as the doctors towards proper treatment. The focus may also be given to patients who previously received inadequate treatment. On the part of doctor’s assurance leading to extended tertiary delay should also be minimized. In order to minimize each of the considered delays especially tertiary delay, there has to be a well-defined referral system by setting acceptable waiting time to make diagnosis and start of treatment. The findings observed under studies related to delay may be helpful to plan community level intervention program propagating information about signs/symptoms related to cancer, need of timely contacting doctor as well as getting in time diagnosis and start of appropriate treatment.
Although the study was planned in a systematic manner, the data collection mainly focused on the cancer patients registered at IRCH, AIIMS. Many other departments registering cancer patients of this institute could not be included in this study. This study is planned at tertiary level. As obvious, the patients coming to this setup are expected to have peculiar characteristics mainly because of dealing referred patients. Strictly speaking, the findings under this study may not be easily generalizable for other health setup. Some of factors considered for various delays in cancer may not be suitable for western countries.
5. CONCLUSION
Current study describes various levels of delay in diagnosis and treatment of common cancer patients and their associated factors. Total duration can be appropriately described using three components as primary, secondary and tertiary delays. Gamma regression and quantile regressions together provide more information than merely use of anyone regression. Study reveals that there is an urgent need and scope to reduce delay at each level-primary, secondary and tertiary. Irrespective of the types of delay, these results suggest a need for universal education to achieve reduction in delay. Medical factors are also responsible for delays. There is a need to set up optimum time for diagnosis and treatment initiation irrespective of types of cancer. In India, there is a need to have well defined referral pattern. Reduction of delays in diagnosis and treatment may reduce the advance stage of cancer.
6. ACKNOWLEDGEMENTS
The authors would like to express their thanks to Dr. V. Sreenivas, Department of Biostatistics, All India Institute of Medical Sciences, New Delhi; Dr. Kishore Chaudhry and Dr. D. K. Shukla, Division of Non-Communicable Diseases, Indian Council of Medical Research, New Delhi, for their critical comments throughout this study.
![]()
![]()
REFERENCES
- World Health Organization (WHO) (2006) Cancer. Geneva, WHO.
- Neal, R.D. (2009) Do diagnostic delays in cancer matter? British Journal of Cancer, 101, 9-12. doi:10.1038/sj.bjc.6605384
- Korsgaard, M., Pedersen, L. and Laurberg, S. (2008) Delay of diagnosis and treatment of colorectal cancer—A population-based Danish study. Cancer Detection and Prevention, 32, 45-51. doi:10.1016/j.cdp.2008.01.001
- Hosseini, S.N., Mousavinasab, S.N., Moghimi, M.H. and Fallah, R. (2007) Delay in diagnosis and treatment of gastric cancer: From the beginning of symptoms to surgery—An andomi study. Turkish Society of Gastroenterology, 18, 77- 81.
- Pitchers, M. and Martin, C. (2006) Delay in referral of oropharyngeal squamous cell carcinoma to secondary care correlates with a more advanced stage at presentation, and is associated with poorer survival. British Journal of Cancer, 94, 955-958. doi:10.1038/sj.bjc.6603044
- Nystrom, L., Rutqvist, L.E., Wall, S., Lindgren, A., Lindqvist, M., Ryden, S., Andersson, I., Bjurstam, N., Fagerberg, G., Frisell, J., et al. (1993) Breast cancer screening with mammography: Overview of Swedishrandomizedtrials. Lancet, 341, 973-978. doi:10.1016/0140-6736(93)91067-V
- Risberg, T., Sorbye, S.W., Norum, J. and Wist, E.A. (1996) Diagnostic delay causes more psychological distress in female than in male cancer patients. Anticancer Research, 16, 995-999.
- Almuammar, A., Dryden, C. and Burr, J.A. (2010) Factors associated with late presentation of cancer: A limited literature review. Journal of Radiotherapy in Practice, 9, 117-123. doi:10.1017/S146039690999029X
- Facione, N.C. (1993) Delay versus help seeking for breast cancer symptoms: A critical review of the literature on patient and provider delay. Social Science & Medicine, 36, 1521-1534. doi:10.1016/0277-9536(93)90340-A
- Abdo, E.N., Garrocho, A., Barbosa, A.A., Oliveira, E.L., Franca-Filho, L., Negri, S.L. and Pordeus, I.A. (2007) Time elapsed between the first symptoms, diagnosis and treatment of oral cancer patients in Belo Horizonte, Brazil. Medicina Oral Patologia Oral y Cirugia Bucal, 12, 469-473.
- Gorin, S.S., Heck, J.E., Cheng, B. and Smith, S.J. (2006) Delays in breast cancer diagnosis and treatment by racial/ethnic group. Archives of Internal Medicine, 166, 2244-2252. doi:10.1001/archinte.166.20.2244
- Salomaa, E.R., Sallinen, S., Hiekkanen, H. and Liippo, K. (2005) Delays in the diagnosis and treatment of lung cancer. Chest, 128, 2282-2288. doi:10.1378/chest.128.4.2282
- Allgar, V.L. and Neal, R.D. (2005) Delays in the diagnosis of six cancers: Analysis of data from the national survey of NHS patients: Cancer. British Journal of Cancer, 92, 1959-1970. doi:10.1038/sj.bjc.6602587
- Gwyn, K., Bondy, M.L., Cohen, D.S., Lund, M.J., Liff, J.M., Flagg, E.W., Brinton, L.A., Eley, J.W. and Coates, R.J. (2004) Racial differences in diagnosis, treatment, and clinical delays in a population-based study of patients with newly diagnosed breast carcinoma. Cancer, 100, 1595-1604. doi:10.1002/cncr.20169
- Look, M., Tan, Y.Y., Vijayan, A., The, C.H. and Low, C.H. (2003) Management delays for early gastric cancer in a country without mass screening. Hepatogastroenterology, 50, 873-876.
- Amir, Z., Kwan, S.Y., Landes, D., Feber, T. and Williams, S.A. (1999) Diagnostic delays in head and neck cancers. European Journal of Cancer Care, 8, 198-203. doi:10.1046/j.1365-2354.1999.00165.x
- Caplan, L.S. and Helzlsouer, K.J. (1992) Delay in breast cancer: A review of the literature. Public Health Reviews, 20, 187-214.
- Tjemsland, L. and Soreide, J.A. (2004) Operable breast cancer patients with diagnostic delay—Oncological and emotional characteristics. European Journal of Surgical Oncology, 30, 721-727. doi:10.1016/j.ejso.2004.05.005
- Hansen, R.P., Olesen, F., Sorensen, H.T., Sokolowski, I. and Sondergaard, J. (2008) Socioeconomic patient characteristics predict delay in cancer diagnosis: A Danish cohort study. BMC Health Services Research, 8, 49-59. doi:10.1186/1472-6963-8-49
- Kumar, S., Heller, R.F., Pandey, U., Tewari, V., Bala, N. and Oanh, K.T. (2001) Delay in presentation of oral cancer: A multifactor analytical study. National Medical Journal of India, 14, 13-17.
- Love, N. (1991) Why patients delay seeking care for cancer symptoms. What you can do about it. Postgraduate Medicine, 89,151-158.
- Kantola, S., Jokinen, K., Hyrynkangas, K., Mantyselka, P. and Alho, O.P. (2001) Detection of tongue cancer in primary care. Journal of the Royal College of General Practitioners, 51, 106-111.
- Lynch, B.M., Baade, P., Fritschi, L., Leggett, B., Owen, N., Pakenham, K., Newman, B. and Aitken, J.F. (2007) Modes of presentation and pathways to diagnosis of colorectal cancer in Queensland. The Medical Journal of Australia, 186, 288-291.
- Allison, P., Franco, E. and Feine, J. (1998) Predictors of professional diagnostic delays for upper aerodigestive tract carcinoma. Oral Oncology, 34, 127-132. doi:10.1016/S1368-8375(97)00078-X
- Habermann, W., Berghold, A., Devaney, T.T. and Friedrich, G. (2001) Carcinoma of the larynx: Predictors of diagnostic delay. The Laryngoscope, 111, 653-656. doi:10.1097/00005537-200104000-00018
- Tromp, D.M., Brouha, X.D., Hordijk, G.J., Winnubst, J.A. and De Leeuw, J.R. (2005) Patient factors associated with delay in primary care among patients with head and neck carcinoma: A case-series analysis. Family Practice, 22, 554-559. doi:10.1093/fampra/cmi058
- Barber, M.D., Jack, W. and Dixon, J.M. (2004) Diagnostic delay in breast cancer. British Journal of Surgery, 91, 49-53. doi:10.1002/bjs.4436
- Pitiphat, W., Diehl, S.R., Laskaris, G., Cartsos, V., Douglass, C.W. and Zavras, A.I. (2002) Factors associated with delay in the diagnosis of oral cancer. Journal of Dental Research, 81, 192-197. doi:10.1177/154405910208100310
- Abdel-Fattah, M.M., Anwar, M.A., Mar, E., El-Shazly, M.K., Zaki, A.A., Bedwani, R.N. and Nicolucci, A. (1999) Patientand system-related diagnostic delay in breast cancer evidence from Alexandria, Egypt. European Journal of Public Health, 9, 15-19. doi:10.1093/eurpub/9.1.15
- Montella, M., Crispo, A., D’aiuto, G., De Marco, M., De Bellis, G., Fabbrocini, G., Pizzorusso, M., Tamburini, M. and Silvestra, P. (2001) Determinant factors for diagnostic delay in operable breast cancer patients. European Journal of Cancer Prevention, 10, 53-59. doi:10.1097/00008469-200102000-00006
- Dodd, S., Bassi, A., Bodger, K. and Williamson, P. (2006) A comparison of multivariable regression models to analyse cost data. Journal of Evaluation in Clinical Practice, 12, 76-86. doi:10.1111/j.1365-2753.2006.00610.x
- National Institute of Family and Welfare (2003) National Cancer Control Programme. http://www.nihfw.org
- Esteva, M., Ramos, M., Cabeza, E., Llobera, J., Ruiz, A., Pita, S., Segura, J.M., Cortes, J.M. and Gonzalez-Lujan, L. (2007) Factors influencing delay in the diagnosis of colorectal cancer: A study protocol. BMC Cancer, 85, 272-276.
- Onizawa, K., Nishihara, K., Yamagata, K., Yusa, H., Yanagawa, T. and Yoshida, H. (2003) Factors associated with diagnostic delay of oral squamous cell carcinoma. Oral Oncology, 39, 781-788. doi:10.1016/S1368-8375(03)00075-7
- Norsa’adah, B., Rampal, K.G., Rahmah, M.A., Naing, N.N. and Biswal, B.M. (2011) Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer, 11, 141-149. doi:10.1186/1471-2407-11-141
- Arndt, V., Sturmer, T., Stegmaier, C., Ziegler, H., Becker, A. and Brenner, H. (2003) Provider delay among patients with breast cancer in Germany: A population-based study. Journal of Clinical Oncology: American Society of Clinical Oncology, 21, 1440-1446. doi:10.1200/JCO.2003.08.071
- Neal, R.D. and Allgar, V.L. (2005) Sociodemographic factors and delays in the diagnosis of six cancers: Analysis of data from the “National Survey of NHS Patients: Cancer”. British Journal of Cancer, 92, 1971-1975. doi:10.1038/sj.bjc.6602623
- Khoo, S.P., Shanmuhasuntharam, P., Mahadzir, W.M., Tay, K.K., Latif, A. and Nair, S. (1998) Factors involved in the diagnosis of oral squamous cell carcinoma in Malaysia. Asia-Pacific Journal of Public Health, 10, 49-51. doi:10.1177/101053959801000111
- Koivunen, P., Rantala, N., Hyrynkangas, K., Jokinen, K. and Alho, O.P. (2001) The impact of patient and professional diagnostic delays on survival in pharyngeal cancer. Cancer, 92, 2885-2891. doi:10.1002/1097-0142(20011201)92:11<2885::AID-CNCR10119>3.0.CO;2-G
- Ozlu, T., Bulbul, Y., Oztuna, F. and Can, G. (2004) Time course from first symptom to the treatment of lung cancer in the eastern black sea region of turkey. Medical Principles and Practice, 13, 211-214. doi:10.1159/000078318
- Radzikowska, E., Roszkowski, K. and Glaz, P. (2001) Lung cancerdiagnosis and therapy delay. Pneumonologia i Alergologia Polska, 69, 600-610.
- Khattak, I., Eardley, N.J. and Rooney, P.S. (2006) Colorectal cancera prospective evaluation of symptom duration and GP referral patterns in an inner city teaching hospital. Colorectal Disease, 8, 518-521. doi:10.1111/j.1463-1318.2006.00967.x
- Wang, J., Liu, F., Gao, H., Wei, W., Zhang, X., Liang, Y. and Cheng, Y. (2008) The symptom-to-treatment delay and stage at the time of treatment in cancer of esophagus. Japanese Journal of Clinical Oncology, 38, 87-91. doi:10.1093/jjco/hym169
- Langenbach, M.R., Schmidt, J., Neumann, J. and Zirngibl, H. (2003) Delay in treatment of colorectal cancer: Multifactorial problem. World Journal of Surgery, 27, 304-308. doi:10.1007/s00268-002-6678-9
- Wallace, D.M., Bryan, R.T., Dunn, J.A., Begum, G. and Bathers, S. (2002) Delay and survival in bladder cancer. British Journal of Urology International, 89, 868-878. doi:10.1046/j.1464-410X.2002.02776.x
- Ashwood, N., Witt, J.D., Hallam, P.J. and Cobb, J.P. (2003) Analysis of the referral pattern to a supraregional bone and soft tissue tumour service. Annals of the Royal College of Surgeons of England, 85, 272-276. doi:10.1308/003588403766275015
- Subramonian, K.R., Puranik, S. and Mufti, G.R. (2003) How will the two-weeks-wait rule affect delays in management of urological cancers? Journal of the Royal Society of Medicine, 96, 398-409. doi:10.1258/jrsm.96.8.398