International Journal of Clinical Medicine
Vol.06 No.01(2015), Article ID:53429,4 pages
10.4236/ijcm.2015.61008
Percutaneous Intervention in Kyphoscoliosis―Tackling a Tortuosity*
Jwalit Morakhia1, Padmakumar Ramachandran1, Naveenchandra Ganiga Sanjeeva1, Harikrishna Damodaran2, Tulsee Sitapara3, Nirlep Gajiwala3, Ashok Thakkar3
1Department of Cardiology, Kasturba Medical College & Hospital, Manipal, India
2Department of Cardiology, Pariyaram Medical College, Kannur, India
3Department of Clinical Trials, Sahajanand Medical Technologies Pvt. Ltd., Surat, India
Email: jwalitm@gmail.com
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 28 December 2014; accepted 14 January 2015; published 21 January 2015
Spine deformities have several associations with compromised cardiorespiratory function. Percutaneous coronary interventions rely on fluoroscopic anatomical landmarks to guide procedures, and distortion of the mediastinal soft tissue and skeletal anatomy in conditions like kyphoscoliosis can pose unique challenges for the interventional cardiologist. Here, we report a case of elderly kyphoscoliotic male patient with worsening angina, who underwent successful percutaneous co- ronary intervention via the radial route.
Keywords:
Kyphoscoliosis, Percutaneous Coronary Intervention, Spine, Technical Challenges

Severe spine deformities pose certain challenges to the interventionalist due to the distorted chest wall and cardiac malposition [1] . Percutaneous coronary intervention in such patients with kyphoscoliosis is rarely reported. Here, we report the challenges we faced during the percutaneous coronary intervention in an elderly male patient with advanced kyphoscoliosis. Our case report provides valuable insights in understanding the position of the heart in patients with thoracic spine deformities. The information provided in the report aids in knowing the need to modify angiographic views in such situations. A proper orientation to the anatomy and correct choice of vascular access are pivotal to the procedural success in such patients with kyphoscoliosis.
An 82-year-old frail male patient with advanced kyphoscoliosis presented with symptoms of worsening angina for past 3 months. His premorbid illness included mild hypertension, which was well-controlled. Baseline echocardiogram revealed normal left ventricular systolic function (ejection fraction―65%). We proceeded with the coronary angiogram via the radial route with a 6Fr sheath. After encountering some difficulty negotiating the aortic arch tortuosity, we used a Tiger 5Fr catheter (Terumo Medica Corp., USA) for the right coronary artery (RCA) injections. Left coronary artery (LCA) could not be cannulated with the Tiger 5Fr catheter; hence, we switched to a XBU 3.5, 5Fr guide catheter (Cordis Corp., USA) for LCA injections (Figure 1). The angiogram revealed chronic total occlusion (CTO) in RCA mid-segment and 90% stenosis in proximal left anterior descending artery (LAD) (Figure 2). We chose percutaneous revascularization of the LAD in favor of CABG as the patient was considered a poor candidate for general anesthesia. Through the XBU 3.5, 5Fr guiding catheter, the lesion was crossed with a Balance-Middle-Weight Universal guidewire (Abbott Vascular, USA) and was predilated with a 2.5 × 10 mm and 3 × 10 mm Pantera balloons (Biotronik, Germany). A 3 × 24 mm Supralimus- eluting stent was deployed at 14 atm pressure (Figure 3) and was post-dilated with a 3.5 mm non-compliant Pantera Leo balloon (Biotronik, Germany). A successful angiographic result was noted (Figure 4). Activated clotting time was maintained above 250 seconds throughout the procedure. Postoperative course in the hospital was uneventful and the patient was discharged in a stable condition. There was no evidence of symptom recurrence at up to 6-month postoperative follow-up.

Figure 1. Plain antero-posterior projection with XBU 3.5, 6Fr catheter in left coronary artery in patient with spine deformity.
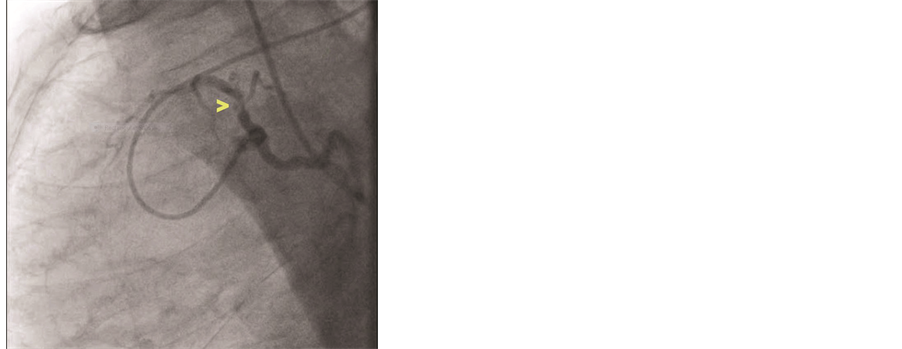
Figure 2. Spider view of the heart showing 90% stenosis in proximal left anterior descending artery (arrow).
Several technical difficulties were encountered during the procedure. Our patient was unable to maintain the supine posture for a long duration and preferred the left lateral position. This precluded a long procedure. While we positioned the patient in the center of the table, the cardiac shadow remained significantly to the left due to the gross mediastinal shift (Figure 1, Figure 5). This prevented certain angulated views since our cath lab uses a large detector system (i.e. Philips AlluraXper FD20). We also noted the gross counter-clockwise rotation of the heart and all views had to be accordingly modified. Indeed, the conventional “spider” view was replicated in a lateral-caudal angulation (Figure 2). The option of femoral access in case of failure to complete the procedure through the radial route was thought to be technically demanding and possibly dangerous. We attempted to change over to a XBU 3.5, 6Fr but could not cross the aortic arch tortuosity and cannulate the LCA. Hence, we proceeded with the 5Fr guide catheter with the backup support admittedly being suboptimal.

Figure 3. Guide stability and stent implantation.

Figure 4. Final angiogram showing good flow in the in left coronary artery after stent-implantation.

Figure 5. Position of the heart in the thorax of kyphoscoliotic patient.
Kyphoscoliosis or hunch back is a progressive deformity of the lateral and posterior spine curvatures, with an estimated prevalence of about 1 in 1000 people for 35˚ deformity angle and 1 in 10,000 people for >70˚ deformity angle [2] [3] . It occurs as a result of disruption of balance between structural and dynamic components or neuromuscular elements of the spine or the balance and the symmetry of the body as a whole. Kyphoscoliosis can be idiopathic or secondary to various neuromuscular, vertebral connective tissue disorders or therapeutic interventions such as thoracoplasty and surgery for recurrent pneumothorax [3] . It has wide-ranging implications with respect to cardiovascular pathology. This includes a higher prevalence of congenital heart disease, mitral valve prolapse syndrome, pulmonary hypertension secondary to the chest wall deformity, and low lung-ventila- tion volumes [1] . However, the technical aspects of coronary intervention in kyphoscoliotic patients have not been reported previously.
The distorted skeletal anatomy and the mediastinal shift can make cardiovascular diagnostics difficult in patients with kyphoscoliosis. Surface electrocardiogram can be unreliable in these patients and echocardiography is the preferred tool for pre-operative screening [4] which again may be impeded by suboptimal acoustic windows. Lung function is commonly impaired, [5] [6] but cardiac function is found to be within normal limits in the majority of patients [1] . While a literature search could not find any information specific to abnormalities in cardiac position in scoliosis, it seems a fair proposition that the heart should occupy more of the hemithorax with less compromised volume, which in most cases is ipsilateral to a concavity in the vertebral column. By the same logic, counter-clockwise or clockwise rotation with a left or right sided concavity respectively can also be ex- pected in scoliosis. It has been noted that the aorta persistently follows the abnormal curvatures of the spine [7] . This can provide guidance in selecting the correct hardware if the femoral route is chosen.
In the present case, we performed a successful stenting in old frail patient with kyphoscoliosis. A similar case of coronary intervention in a 32-year-old male patient with achondroplasia and kyphoscoliosishas been reported by Srinivas SK and colleagues [8] . They demonstrated that, despite the technical difficulties due to the short stature of patient, the coronary angioplasty can be performed safely without any additional risks in patients with dwarfism and achondroplasia. Although the kyphoscoliotic patient in our case was of very old age, we observed similar procedural outcomes (Figure 1, Figure 5). To the best of our knowledge, this is the first case report of successful coronary stenting in kyphoscoliotic patient. We suggest that further studies are warranted to improve the technical aspects of the intervention procedure in this group of patients.
In conclusion, we sought to highlight certain unique problems an interventionalist faces while treating a patient with kyphoscoliosis. A proper orientation to the anatomy and correct choice of vascular access are cardinal to procedural success in these patients.
- Liu, Y.-T., Guo, L.-L., Tian, Z., Zhu, W.-L., Yu, B., Zhang, S.-Y. and Qiu, G.-X. (2011) A Retrospective Study of Congenital Scoliosis and Associated Cardiac and Intraspinal Abnormities in a Chinese Population. European Spine Journal, 12, 2111-2114. http://dx.doi.org/10.1007/s00586-011-1818-2
- Sujay, M., Laxmi, P.K., Merajuddin, S., Venugopalan, V.M. and Raghunath, R. (2014) Anesthetic Management of an Anemic Parturient with Severe Kyphoscoliosis and Bilateral Poliomyelitis for Emergency Caesarean Section. Journal of Evolution of Medical and Dental Sciences, 3, 5461-5466. http://dx.doi.org/10.14260/jemds/2014/2614
- Gupta, S. and Singariya, G. (2004) Kyphoscoliosis and Pregnancy―A Case Report. Indian Journal of Anaesthesia, 48, 215-215.
- Ipp, L., Flynn, P., Blanco, J., Green, D., Boachie-Adjei, O., Kozich, J., Chan, G., Denneen, J. and Widmann, R. (2011) The Findings of Preoperative Cardiac Screening Studies in Adolescent Idiopathic Scoliosis. Journal of Pediatric Orthopaedics, 7, 764-766. http://dx.doi.org/10.1097/BPO.0b013e31822f14d6
- Caro, C.G. and DuBois, A.B. (1961) Pulmonary Function in Kyphoscoliosis. Thorax, 3, 282-290. http://dx.doi.org/10.1136/thx.16.3.282
- Mezon, B., West, P., Israels, J. and Kryger, M. (1980) Sleep Breathing Abnormalities in Kyphoscoliosis. The American Review of Respiratory Disease, 4, 617.
- Nathan, H. (1988) Relations of the Soft Structures of the Posterior Mediastinum in the Scoliotic Spine. Cells Tissues Organs, 3, 260-264. http://dx.doi.org/10.1159/000146650
- Srinivas, S.K., Ramalingam, R. and Manjunath, C.N. (2013) A Rare Case of Percutaneous Coronary Intervention in Achondroplasia. Journal of Invasive Cardiology, 6, E136-E138.

*Coronary Intervention in Kyphoscoliosis.