 Psychology 2014. Vol.5, No.2, 160-165 Published Online February 2014 in SciRes (http://www.scirp.org/journal/psych) http://dx.doi.org/10.4236/psych.2014.52025 OPEN ACCESS Gender Dysphoria and Body Integrity Identity Disorder: Similarities and Differences Alicia Garcia-Falgueras The Official College of Psychologists, Madrid, Spain Email: algarfal@gmail.com Received November 21st, 2013; revised December 22nd, 2013; accepted January 17th, 2014 Copyright © 2014 Alicia Garcia-Falgueras. This is an open access article distributed under the Creative Com- mons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, pro- vided the original work is prop erly cited. In accordance of the Creative Commons Attributio n License all Copy- rights © 2014 are reserved for SCIRP and the owner of the intellectual property Alicia Garcia-Falgueras. All Copyright © 2014 a re guarded by law and by SCIRP as a guardian. Gender Dysphoria and Body Integrity Identity Disorder are sometimes together in the 19% of the cases. Other discomfort diseases related to identity, body scheme and/or integrity are discussed in relation to Gender Dysphoria. Because persons experiencing Gender Dysphoria need a precise diagnostic that pro- tects their access to care and will not be used against them in social, occupational or legal areas a distinc- tion diseases is provided in this text, because a meticulous description with clear exclusion criteria is re- quired. Keywords: Gender Dysphoria; Delusional Disorder-Somatic; Body Dysmorphic Disorder; Body Integrity Identity Disorder; Parietal Cortex Introduction: Concepts, Definitions and Consideration s f or Identity Identity and self are concepts not easy to describe or quantify. There has been thousands of thinkers and Philosophers across History and time who pursued to add some clarity to those eva- sive ideas, because at the time one thinks about them, they change their size and entity. In 1690, J. Locke realized memory had an important role for personal identity, as including our experiences and learning processes as part of our way to be, that is different from the rest. Locke hold personal identity as a matter of psychological con- tinuity (Nimbalk a, 2011). For declarative and procedural memories consolidation is required the hippocampus were bilaterally activated while the memory is being created, and later that event is consolidated and strengthened in the cortex, together with amygdale and orbitofrontal participation (Eichenbaum et al., 1996; Fink et al., 1996; Viard et al., 2007). Although there are several brain net- works to create a memory. Autobiographical memory is the one related to build our own identity, but there are quite an agree- ment between different authors, concerning to the necessity of awareness for timing course and an existence of a specifically personal engaged to the event to remember related to its mean- ing and to a motivation for being involved in the reconstruction of one’s own past and autobiographical memory (Fink et al., 1996; Fink, 2003). Amygdale (emotions) and will (anterior cingulated cortex) might be important brain areas to be in- volved in fixing memories, including autobiographical (Swaab, personal comm.). This role was such a crucial aspect of identity for Locke to say if someone does not remember nothing of his or her past, then he or she “literally has no identity” (Locke, 1975). This consideration of identity as the same as memory was defined by Joseph Butler as a “wonderful mistake”: “In other words, I can remember only my own experiences, but it is not my memory of an experience that makes it mine; rather, I remember it only because it’s already mine. So while memory can reveal my identity with some past experiencer, it does not make that expe- riencer me. What I am remembering”, then, insists Butler, “are the experiences of a substance, namel y, the same substance that constitutes me now” (Butler, 1975). Later on, the philosopher and psychologist William James at the end of 19th century tried to reorganize ideas for identity (Sollberger, 2013). He made a core distinction between two aspects of identity: the “me” and the “I”. The former referring to the permanence and continuity in present time and space of the self while the later also were including the past experiences as an integral part of consciousness. Kant were also more in line with James, since he sustained all knowledge, including self-knowledge, must be derived a posteriori from experiences of sensation and reflection. Although, perhaps the concepts of I, me, and min e are built empirically, but perhaps the primitive sense of the self or identity, as distinct from other objects and people in the environment, is given a priori. Self-consciousness for Kant therefore implies a priori knowledge about the neces- sary and universal truth expressed in this principle of appercep- tion, (the lens of past experiences; (Ott, 2004)) through which identity is built a posteriori, but the original primitive a priori knowledge cannot be based on experience. Nowadays it is accepted memory is not only for identity as Locke sustained, but only the episodic memory as our autobio- graphical memory about the self for the events and experiences in our lives, which includes a mental representation of the self as the main acting role for some action, while other memories, A. GARCIA-FALGUERAS OPEN ACCESS such as semantic memory, are the personal generic knowledge about the world (Kihlstrom & Klein, 1997). Gender Dysphoria (GD) Being a woman or a man is a very relevant aspect of our- selves, configuring our behavior and preferences and also the social expectations. Transsexualism, the most extreme form of Gender Dysphoria, is an individual’s unshakable conviction of belonging to the opposite sex than the chromosomes say, which often leads to a request for sex-reassignment surgery and hor- monal treatment for life (Blanchard, 1993; Cohen-Kettenis & Gooren, 1999). Transsexual people desire to live and be ac- cepted as a member of the gender opposite to that assigned at birth (Hembree et al., 2009). The term Male-to-Female (MtF) transsexual refers to a chromosomally male who identified on the female gender; the term Female-to-Male (FtM) transsexual means a chromosomally female person who identified on the male gender. Gender dysphoria (GD) is a DSM-V diagnosis that recently has been separated from Sexual Dysfunctions and Paraphillic Disorders because persons experiencing gender dys- phoria need a diagnostic term that protects their access to care and will not be used against them in social, occupational or legal areas. In DSM-IV-TR it is defined as: A) A strong and persistent cross-gender identification, com- bined with a persistent discomfort with one’s sex or sense of inappropriateness in the role of that sex, causes clinically sig- nificant distress. B) Persistent discomfort with his or her sex or sense of inap- propriateness in the role of that sex. C) The disturbance is not concurrent with a physical intersex condition. D) The disturbance causes clinically significant distress or impairment in social, occupational or other important areas of functioning. Usually the gender assigned at birth is that one correspond- ing to the chromosomal information, but many exceptions hap- pens considering only genetic data (Kandhelwal et al., 2010). The reason why this criteria is still very used is because these two parameters (chromosomes-gender) are practically always correlated in an animal (Ngun et al., 2011). Recently, Australi- an and after them German legislation, which went into effect on Friday November 1st in 2013, were enacted in order to give parents and children more time before making life-changing sex reassignment decisions in cases of intersex genital characteris- tics at birth. This will happen in German legislation having a third option (blank for gender designation box in babies whose gender is not clear at birth) only of their birth certificates, not other legal registries such as passports, being possible to change this blank designation later on to male or female or can be left blank indefinitely (Stafford, 2013). Only in 23% of cases (1/3 according to the DSM-V) does a childhood gender problem leading to transsexuality in adult- hood. With regard to sexual orientation, the most likely out- come of childhood gender identity disorder is adult homosex- uality or bisexuality. This population is served by clinicians (Gender Teams) because they usually suffer from abuses and on one-fourth of patients reported childhood maltreatment (Ban- dini et al., 2011). According to the onset time, transsexuality can be divided in two different courses: early and late onset. In the early one, the discomfort is present since the beginning of cross gender iden- tification, between 2 and 4 years old. In late onset the cross gender identification appears during puberty or adulthood, in a more gradually way and being concurrent sometimes with Transvestism Fetishism (DSM-IV-TR). It must be noted, how- ever, that gender identity development is intrinsically pro- grammed and there is no way of prevention for the disorder (Looy & Bouma, 2005). On the other hand, some specific dif- ferences in onset timing might be happening between sexes, for Male-to-Female and Female-to-Male transsexuals (Lawrence, 2010). There are still many confusions and doubts about what trans- sexualism is in general population. The reason why might be related to some mixed definitions or not boundaries well estab- lished. For clarifying purposes, here we would like to explain what is NOT transsexualism (Table 1) (as the extreme Gender Dysforia form): A) It is not an extreme form of homosexuality. Although homosexuality is not included in the DSM any more, some confusion it is still surrounding the two concepts: gender dysphoria and gender orientation are two independent processes in our brain. Neuroanatomical studies have shown there are some brain regions located in the hypothalamus which were related to sexual orientation in its volume—such as the subdivision INAH3-(LeVay, 1991) and also to gender dyspho- ria in its volume and number of neurons (Garcia-Falgueras & Swaab, 2008). Other regions were related only to gender dys- phoria in its intermediate values for volume and number of cells —INAH1—(Garcia-Falgueras et al., 2011) and the other region in human hypothalamus were not different among man and woman, nor related to sexual orientation or to gender dysphoria —INAH4—(Allen et al., 1989; LeVay, 1991; Garcia-Falgueras & Swaab, 2008; Garcia-Falgueras et al., 2011). On the other hand, there are many reasons to logically con- sider sexual orientation and gender dysphoria as different processes in our brains. For instance, it is widely accepted, since Kinsey’s scales, there are many grades in sexuality, de- fined as a continuum from 0 to 6, from exclusive heterosexual behavior to exclusive homosexual behavior. While for gender dysphoria there are two categories (male to female and female to male) although a third one can be also considered in cases of gender indeterminacy at birth (Stafford, 2013). Hypothetically those characteristics measured by different grades in scales might be belonging to different specialization brain networks, although they could share some components, such are those related to sexual arousal or libido which are located in the b rain in the insula, the inferior and middle frontal gyrus and the hy- pothalamus as well (Hu et al., 2008), also incuding more cor- tical areas such as the anterior cingulated cortex, the anterior temporal cortex, and the ventral globus pallidus (Rauch et al., 1999). B) It is not a delusional disorde r, somatic type. This is a primary disorder that is diagnosed when prominent nonbizarre delusions coming from the own body (odors, mal- formations, insects, etc.) are present for at least one month and the symptoms criteria for Schizophrenia have never been met. Hallucinations may be present but auditory or visual hallucina- tions cannot be prominent. For the somatic type the delusions are mainly related to physi cal defect, functions or general med- ical condition (DSM-IV-TR). The exclusion criteria for Gender Dysphoria might be: 1st) the prominent nonbizarre delusions are never related to the gender, role or sex, but with some physical defect or general 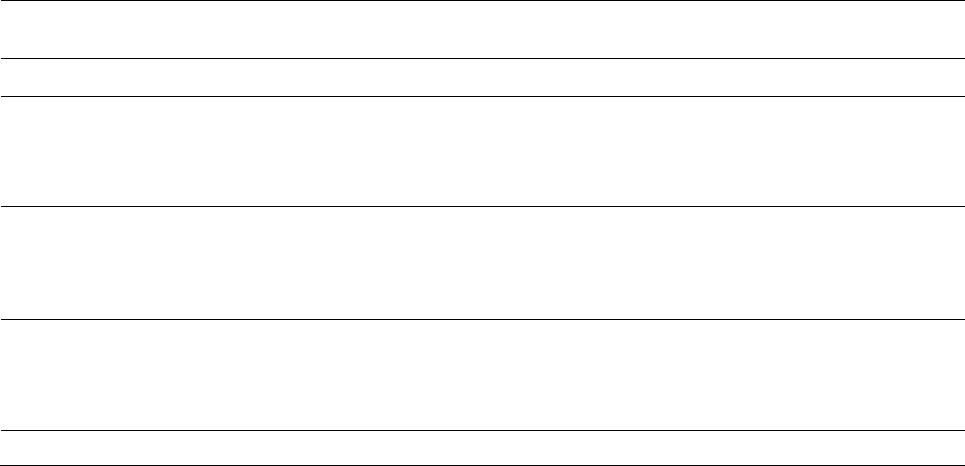 A. GARCIA-FALGUERAS OPEN ACCESS Table 1. Common aspects and main differences between Gender Dysphoria, homosexuality and some DSM disorders. Coincidenc e 58% (Sm i t h et al., 2005) Gender: cont inuum 3 levels Orientation: continuum 6 levels DELUSIONAL DISORDER, SOMATIC Discomfort coming from the own body ) the body dysmorphic disorder is about a real physical minor flaw (i.e. acne) exaggerated to the extreme of causing deep impairment but it is not related to gender, role or sex. nd) In Gender Dysphoric pat i ents, afte r hor mones and surgical intervention and rest or ation of c omfort bet ween body a nd gender, most of cases dysphoria do not persist. Discomfort coming from the own body st) the prominent nonbizarre delusions are never related to the gender, role or sex, but with some physical defect or general medical condition and nd) in Gender Dysphoric patients, after hormones and surgical intervention and rest or ation of c omfort bet we en body and gender, most of cases dysphoria do not persist. DISOCIATIVE IDENTITY DISORDER Inequal personalities or identities. ) in dissociative identity differe nt personalities are belonging to the nd) in dissociative identity memory problems are related. rd) In Gender Dysphoric patients, after hormones and surgical intervention and rest or ation of c omfort bet ween body a nd gender, most of cases dysphoria do not persist. BODY INTEGRITY IDENTITY DISORDER Coincidenc e 19% (First , 2005; Lawrence, 2006; First & Fisher, 2012) 1st) in Body Identity Integrity Disorder desires of amputations are related to arms a nd l egs, not to genitals or breasts. medical condition and 2nd) In Gender Dysphoric patients, after hormones and sur- gical intervention and restoration of comfort between body and gender, most of cases dysphoria do not persist. C) It is not a body dysmorphic disorder Body dysmorphic disorder is a secondary somatoform dis- order marked by a preoccupation and perpetual negative thoughts about their appearance with pain and discomfort. It is based on a imagined or trivial defect in appearance (usually related to skin, hair or nose) that causes clinically significant distress or impairment in social, occupational or other impor- tant areas of functioning. The exclusion criteria for Gender Dys- phoria might be: 1st) the body dysmorphic disorder is about a real physical minor flaw (i.e. acne) exaggerated to the extreme of causing deep impairment but it is not related to gender, role or sex. 2nd) In Gender Dysphoric patients, after hormones and sur- gical intervention and restoration of comfort between body and gender, most of cases dysphoria do not persist. D) It is not a dissociative identity disorder DSM-IV-TR defines a dissociative disorder or multiple per- sonality disorder as an extremely rare mental secondary disord- er characterized by at least two distinct and relatively enduring identities or dissociative personality states that alternatively control a person’s behavior, accompanied by memory impair- ments, lapsus and asymmetric amnesia. The exclusion criteria for Gender Dysphoria might be: 1st) in dissociative identity different personalities are belong- ing to the same gender. 2nd) in dissociative identity memory problems are related. 3rd) In Gender Dysphoric patients, after hormones and sur- gical intervention and restoration of comfort between body and gender, most of cases dysphoria do not persist. E) It is not a Body Identity Integr i ty Disorder (BIID) Currently BIID is not included in the International Statistical Classification of Diseases 11th revision nor in the Diagnostic and Statistical Manual of Mental Disorders IV or V. As such this disorder is often not known to surgeons, neurologist and psychiatrists. Although both, the BIID and the transsexual desire of gona- dectomy could be defined as a deep discomfort sensations that causes clinically significant distress to the patient, in both dis- orders patients recognize reality, meaning those discomfort sensations are illusions, not delusions. In both cases, after sur- gical restoration discomfort between body and gender or iden- tity does not persist. Those people have in common that they are preoccupied (defined as extreme or excessive concern) with their body concept. That preoccupation causes clinically signifi- cant distress (depressed mood, anxiety, shame) or impairment in occupational or other important social areas. The distress increases and intensifies the desire of changing their bodies. The unique exclusion criteria for Gender Dysphoria might be: 1st) in Body Identity Integrity Disorder desires of amputa- tions are related to arms and legs, not to genitals or breasts. Then, could be those diseases related someway in the brain? Firstly described as apotemnophile (amputation lovers) by Money et al. (1977) and most recently as Xenomelia (McGeogh et al., 2011; Brugger et al., 2013), a holdover from sexological research at Johns Hopkins in the 1970s, Body Integrity Identity Disorder (BIID) is used to describe people who feel from an early age that part of their body does not belong to them and they want to get rid of it, no matter what the cost is. They do not accept a particular limb as part of their body, even if it there’s nothing wrong with its structure and function. Neuroanatomically the BIID is characterized by an increased excitability of the dorsal-horn neurons, a reduction of inhibitory processes, and structural changes at the central nerve endings of the primary sensory neurons, the interneurons and the projec- tion neurons. This central sensitization is mediated by the NMDA receptor and its transmitter is glutamate (Flor, 2002). Thalamic stimulation and recordings in human amputees have A. GARCIA-FALGUERAS OPEN ACCESS shown that reorganizational changes also occur at the thalamic level and are closely related to the perception of phantom limbs and phantom-limb pain. Tactile stimulation for undesired limbs causes a different brain activity (van Dijk et al., 2013). It has been suggested an absent memory process by a Hebbian learn- ing mechanism for the limbs after amputation that could ex- plain the weak phantom feelings (Ramachandram & Hirstein, 1998). After the amputation, a cortical reorganization via long- range horizontal collateral pyramidal neurons through the GABA releasing might be occurring adjacent to the deaffe- rented areas (DeFelipe et al., 1986). BIID patients usually report thinking about their perceived appearance flaws for an average of 3 - 8 hours a day and about one quarter report for more than 8 hours a day (Phillips et al., 2010). In BIID different motivations for wanting an amputation have been described and they usually report more than one reason, although restoring identity is much more likely to be reported as primary (First, 2005). This pathology is usually strongly associated with high levels of social anxiety and some obsessive compulsive behaviors (i.e. mirror checking) have been described. Very poor functioning and high levels or rates of depression, anxiety, social anxiety, anger/hostility, suicidali- ty and other proxy measures of distress are usually described (Phillips et al., 2010). There is a small subgroup of Gender Dysphoric patients who also present with symptoms relevant to BIID (Phillips et al., 2010) or BIID patients that present similar symptoms that Gender Dysphoric (First, 2005; Lawrence, 2006; First & Fisher, 2012). The conviction that a lower leg or arm does not belong to them develops at an early age, generally when patients are a child, or sometimes as a young adult. A child with BIID will cut figures out of newspapers, and then chop off the leg that they want to have amputated themselves. Although very little research has been done during development, several similarities were found for body dysmorphic disorders (BDD) between youth and adults (Phillips et al., 2010). Some patients have these feeling increased progressively over his early adult years and would intensify these feelings when they are under stress (First, 2005). This leads to an overpowering desire for amputa- tion. Only once their limbs have been amputated, they do feel “complete”. Surgeons who carry out these requests run the risk of being condemned for amputating a healthy limb. It seems that two-thirds of those patients, who do ultimately manage to have an amputation, damage their unwanted limb to the extent that it has to be amputated. Sometimes this involves putting their whole life in danger by putting a bullet through the knee- cap, freezing the leg or using a saw to do the job themselves and paradoxically they finally “feel c omplete” and with the only regret of no having done it sooner. They can even get agitated, extremely envious or even sexually arousal activated when they see handicapped people who have to live without a leg or an arm, and sometimes this is the moment that they first realize that this is what they themselves wa nt (First , 2005; First & Fisher, 2012). Often they will try to imitate the desired situation as close as possible, for example by using an elastic bandage to bind a leg against their buttocks, wearing wide trousers which hide the lower part of the leg, folding up a trouser leg, walking with crutches or using a wheelchair. Males are more likely affected by BIID than females (Braam et al., 2006). The connection with transsexuality is especially intriguing due to the percentage (19 percent) of BIID patients who also exhibit a gender identity problem and the high percentage of homosexual and bisexual BIID patients (also 19 percent) (First, 2005; Lawrence, 2006). Comorbidity with depressive, anxiety or somatoform disorders have been described (First, 2005). But psychotherapy or pills do not generally change the minds of those afflicted with the disorder, al though there is one report of a BIID patient feeling less miserable after taking anti-depres- sants and following cognitive behavioral therapy (Flor et al., 2002). Later this patient told that, although it was nice to talk to someone it did not change his desire for amputation at all . A recent research on BIID and MRI have proved the tactile stimulation for undesired limb is reduced in its brain activity, involving the parietal lobe, suggesting the BIID might be cause by altered integration or somatosensory and propioceptive information (van Dijk et al., 2013). Curiously parital cortex has been related to body scheme for perception of the self in my- tical experiences (Beauregard & Paquette, 2006). There is evi- dence that the parietal cortex is part of the neuronal systeme implicated in the processing of visuospatial representation of the body schema in the process of self/other distintion (Neggers et al., 2006). The BIID and the GD can be both e xpla ine d by a me cha nism hard-wiring where the body image is represented innately into the brain. It has been suggested the image of the sex organs of transsexuals are “hard-wired” in the brain in a manner which is opposite to that of their biological sex (Ramachandran & McGeoch, 2007; Brang et al., 2008). This idea is based on the fact that in transsexual population a different pattern of phan- tom syndromes occurs after castration or breast extirpation (Ramachandram & McGeogh, 2007; Brang et al., 2008). After gonadectomy and breast removal, transsexual patients expe- rience a phantom syndrome less frequently than the non-trans- sexual population (Ramachandram & McGeoch, 2007). Around 60% of men who have to have their pennies amputated for cancer will experience a phantom penis post-penectomy, but only 30% of the post-operative male-to-female transsexuals reported the incidence of a phantom penis. On the other hand surprisingly the 62% of the female -to-male transsexual patients reported having felt vivid phantom penises, including phantom erections for many years. Moreover only the 10% of those fe- male to male transsexual patients experienced phantom breast sensations post-operatively (Ramachandram & McGeoch, 2008). One important difference between GD and BIID persons is the fact cortical reorganization might happen in different areas. For BIID the motor parietal area is crucial, while for genitals the location is more inside the brain, c lose to the foot represen- tation in the Penfield homunculus (Ramachandram & Hirstein, 1998). In some cases (19%) these can be overlapped, but no so often, making them different diseases. Exclusion diagnosis have to be done for other identity disorders, such as the Body Integrity Identity Disorder (BIID), because the connection with transsexuality is especially intriguing in these cases due to the percentage of BIID subjects (19%) (First, 2005; Lawrence, 2006) who also exhibit a gender dysphoric problem. In both cases the satisfying patient’s demands for a surgical interven- tion still remains the only way to improve their clinical condi- tions and to avoid the onset of many other different and dra- matic complications. Without any treatment the trouble might became chronic without remission and with high suicides rates. Psychology for Transsexuali sm Sexual minorities are at a higher risk of maltreatment and  A. GARCIA-FALGUERAS OPEN ACCESS abuse (Corliss et al., 2002), together with their higher body dissatisfaction and a worse lifetime mental health reported. Maltreatment was defined in this study as an emotional abuse and/or neglect, physical abuse and/or neglect and sexual abuse (Bandini et al., 2011). However, an accurate mental health pro- fessional diagnosis is usually recommended to be made for the Gender Disorders (Hembree et al., 2009). Any treatment deci- sions, even when reversible, mig ht always be tak en by a whole clinical team after considering social and familiar circum- stances (Kreukels & Cohen-Kettenis, 2011). Since the benefits of clinical treatment for Gender Dysphoria are translated into a reduction of social ostracism, the complexities of sex-reassign- ment surgery, its biomedical treatment and the importance of reducing family psychopathologies or stress when they are present (Zucker et al., 2012) could be the clinical goals, toge- ther with an accurate and precise diagnosis, which are per- spective to be always considered and supported. For those rea- sons a commitment of health in psychology/psychiatric and physicians/endocrine professionals to collaborate in under- standing and properly care treating these difficult diseases (Hem- bree et al., 2009) would be required. Acknowledgemen ts I thank Prof. Dick F. Swaab for his help in research and Dr. Jenneke Kruisbrink for her literature resource help. REFERENCES Allen, L. S., Hines, M., Shryne, J. E., & Gorski, R. A. (1989). Two sexually dimorphic cell groups in the human brain. The Journal of Neuroscience, 9, 497-506. http://www.jneurosci.org/content/9/2/497.long Bandini, E., Fisher, A. D., Ricca, V., Ristori, J., Meriggiola, M. C., Jannini, E. A., Ma nieri, C., Corona, G., Monami, M., Fanni, E., Gal- leni, A., Forti, G., Mannucci, E., & Maggi, M. (2011). Childhood maltreatment in subjects with male-to-female gender identity disord- er. International J our nal of Impotence Researc h, 23, 276-85. http://dx.doi.org/10.1038/ijir.2011.39 Beauregard, M., & Paquette, V. (2006). Neural correlates of a mystical experience in Carmelite nuns. Neuroscience Letters, 405, 186-190. http://dx.doi.org/10.1016/j.neulet.2006.06.060 Bentz, E. K., Hefler, L. A., Kaufmann, U., Huber, J. C., Kolbus, A., & Temp f e r, C. B. (2008). A polymorphism of the CYP17 gene related to sex steroid metabolism is associated with female-to-male but not male -to female transsexualism. Fertility and Sterility, 90, 56-59. http://dx.doi.org/10.1016/j.fertnstert.2007.05.056 Bentz, E. K., Schneeberger, C., Hefler, L. A., van Trotsenburg, M., Kaufmann, U., Huber, J. C., & Temp fer, C. B. (2007). A common polymorphism of the SRD5A2 gene and transsexualism. Reproduc- tive Sciences, 14, 705-709. http://dx.doi.org/10.1177/1933719107306230 Blanchard, R. (1993). Partial versus complete autogynephilia and gen- der dysphoria. Journal of Sex & Marital Therapy, 19, 301-307. http://dx.doi.org/10.1080/00926239308404373 Braam, A. W., Visser, S., Cath, D. C., & Hoogendijk, W. J. (2006). Inves- tigation of the syndrome of apotemnophilia and course of a cogni- tive-behavioural therapy. Psychopathology, 39, 32-37. http://dx.doi.org/10.1159/000089661 Brang, D., McGeoch, P. D., & Ramachandran, V. S. (2008). Apotem- nophilia: A neurological disorder. Neuroreport, 19, 1305-1306. http://dx.doi.org/10.1097/WNR.0b013e32830abc4d Brugger, P., Lenggenhager, B., & Giummarra, M. J. (2013). Xenomelia: A social neuroscience view of altered bodily self-consciousness. Frontiers in Psychology, 4, 204. http://dx.doi.org/10.3389/fpsyg.2013.00204 Butler, J. (1975). “Of Personal Iden tity” in “The Analo gy of Religio n”. Berkeley: University of California Press. Cohen-Kettenis, P. T., & Gooren, L. J. (1999). Transsexualism: A re- view of etiology, diagnosis and treatment. Journal of Psychoso- matic Research, 46, 315-333. http://dx.doi.org/10.1016/S0022-3999(98)00085-3 Corliss, H. L., Cochran, S. D., & Mays , V. M. (2002). Reports of pa- rental maltreatment during childhood in a United States population- based survey of homosexual, bisexual and heterosexual adults. Child Abuse & Neglect, 26, 1165-1178. http://dx.doi.org/10.1016/S0145-2134(02)00385-X DeFelipe, J., Con ley, M., & Jones, E. G. (1986). Long-range fo cal col- lateralization of axons arising from corticocortical cells in monkey sensory-motor c ortex. The Journal of Neuroscience, 6, 3749-3766. http://www.jneurosci.org/content/6/12/3749.long Eichenbaum, H., Schoenbaum, G., Young, B., & Bunsey, M. (1996). Functional organization of the hippocampal memory system. Pro- ceedings of the Nation al Academy of Scien ces of the United S tates of America, 93, 13500-13507. http://dx.doi.org/10.1073/pnas.93.24.13500 Fink, G. R., Markowitsch, H. J., Reinkemeier, M., Bruckbauer, T., Kessler, J., & Heiss, W. D. (1996). Cerebral representation of one’s own past: Neural networks involved in autobiographical memory. The Journal of Neuroscience, 16, 4275-4282. http://dx.doi.org/10.1093/brain/awg212 Fink, G. R. (2003). In search of one’s own past: The neural bases of autobiographical memories. Brain, 126, 1509-1510. http://brain.oxfordjournals.org/content/126/7/1509.long First, M. B., & Fisher, C. E. (2012). Body integrity identity disorder: The persistent desire to acquire a physical disability. Psychopathol- ogy, 45, 3-14. http://dx.doi.org/10.1159/000330503 First, M. B. (2005). Desire for amputation of a limb: Paraphilia, psy- chosis, or a new type of identity disorder. Psychological Medicine, 35, 919-928. http://dx.doi.org/10.1017/S0033291704003320 Flor, H. (2002). Phantom-limb pain: Characteristics, causes, and treat- men t. The Lancet Neurology, 3, 182-189. http://dx.doi.org/10.1016/S1474-4422(02)00074-1 Garcia-Falgueras, A., Ligtenberg, L., Kruijver, F. P., & Swaab, D. F. (2011). Galanin neurons in the intermediate nucleus (InM) of the human hypothalamus in relation to sex, age, and gender identity. Journal of Comparative Neurology, 519, 3061-3084. http://dx.doi.org/10.1002/cne.22666 Garcia-Falgueras, A., & Swaab, D. F. (2008). A sex difference in the hypothalamic uncinate nucleus: Relationship to gender identity. Brain, 131, 3132-3146. http://dx.doi.org/10.1093/brain/awn276 Hembree, W. C., Cohen-Kettenis, P., Delemarre-van de Waal, H. A., Gooren, L. J., Meyer 3rd, W. J., Spack, N. P., Tangpricha, V., & Montori, V. M. (2009). Endocrine treatment of transsexual persons: An endocrine society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 94, 3132-3154. http://dx.doi.org/10.1210/jc.2009-0345 Huh, J., Park, K., Hwang, I. S., Jung, S. I., Kim, H. J., Chung, T. W., & Jeong, G. W. (2008). Brain activation areas of sexual arousal with olfactory stimulation in men: A preliminary study using functional MRI. The Journal of Sexual Medicine, 5, 619-625. http://dx.doi.org/10.1111/j.1743-6109.2007.00717.x Khandelwal, A., Agarwal, A. & Jiloha, R. C., (2010). A 47, XXY fe- male with gender identity diso rder. Archives of Sexual Behavior, 39, 1021-1023. http://link.springer.com/article/10.1007%2Fs10508-010-9628-x Kihlstrom, J. F., & Klein, S. B. (1997). Self-knowledge and self-aware- ness. Annals of the New York Academy of Sciences, 818, 4-17. http://dx.doi.org/10.1111/j.1749-6632.1997.tb48242.x Klempan, T., Hudon-Thibeault, A. A., Oufkir, T., Vaillancourt, C., & Sanderson, J. T. (2011). Stimulation of serotonergic 5-HT2A recep- tor signaling increases placental aromatase (CYP19) activity and ex- pression in BeWo and JEG-3 human choriocarcinoma cells. Placenta, 32, 651-656. http://dx.doi.org/10.1016/j.placenta.2011.06.003 Kreukels, B. P., & Cohen-Kettenis, P. T. (2011). Puberty suppression in gender identity disorder: The Amsterdam experience. Nature Re-  A. GARCIA-FALGUERAS OPEN ACCESS views Endocrinology, 7, 466-472. http://dx.doi.org/10.1038/nrendo.2011.78 Lawrence, A. A. (2010). Sexual orientation versus age of onset as b ases for typologies (subtypes) for gender identity disorder in adolescents and adults. Archives of Sexual Behavior, 39, 514-545. http://dx.doi.org/10.1007/s10508-009-9594-3 LeVay, S. (1991). A difference in hypothalamic structure between he- terosexual and homosexual men. Science, 253, 1034-1037. http://dx.doi.org/10.1126/science.1887219 Locke, J. (1975). Of identity and diversity. In Essay concerning human understanding. Reprinted in John Perry John, 1975, Personal identity. Berkeley: University of California Press. Looy, H., & Bouma , H. (2005). The nature of gender: Gender identity in persons who are intersexed or transgendered. Journal of Psychol- ogy and Theology, 33, 166-178. http://journals.biola.edu/jpt/volumes/33/issues/3/articles/166 McGeoch, P. D., Brang, D., Song, T., Lee, R. R., Huang, M., & Ra ma - chandran, V. S. (2011). Xenomelia: A new right parietal lobe syn- drome. Journal of Neurology, Neurosurgery & Psychiatry, 82, 1314- 1319. http://dx.doi.org/10.1136/jnnp-2011-300224 Money, J. (1977). Bisexual, homosexual, and heterosexual: Society, law, and medicine. Journal of Homosexuality, 2, 229-233. http://dx.doi.org/10.1300/J082v02n03_05 Neggers, S. F., Van der Lubbe, R. H., Ramsey, N. F., & Po st ma , A. (2006). Interactions between ego- and allocentric neuronal represen- tations of space. Neuroimage, 31, 320-331. http://dx.doi.org/10.1016/j.neuroimage.2005.12.028 Ngun, T. C., Ghahramani, N., Sánchez, F. J., Bocklandt, S., & Vilain, E. (2011). The genetics of sex differences in brain and behavior. Fron- tiers in Neuroendocrinology, 32, 227-246. http://dx.doi.org/10.1016/j.yfrne.2010.10.001 Nimbalkar, N. (2011). John locke on personal identity. Mens Sana Mo- nogr, 9, 268-275. Nishizawa, S., Benkelfat, C., Young, S. N., Leyton, M., Mzengeza, S., de Montigny, C., Blier, P., & Diksic, M. (1997). Differences between males and females in rates of serotonin synthesis in human brain. Proceedings of the National Academy of Sciences of the Uni ted Sta tes of America, 94, 5308-5313. http://www.pnas.org/content/94/10/5308.long Ott, C. (2004). The evolution of perception and the cosmology of sub- stance, James W: Principles of psychology, volume 1. New York: Henry-Holt & Co. Phillips, K. A., Wilhelm, S., Koran, L. M., Didie, E. R., Fallon, B. A., Feusner, J., & Stein, D. J. (2010). Body dysmorphic disorder: Some key issues for DSM-V. Dep ress Anxiety, 27, 573-591. http://onlinelibrary.wiley.com/doi/10.1002/da.20709/abstract Ramachandran, V. S., & McGeoch, P. D. (2008). Phantom penises in transsexuals evidence of an innate gender-specific b ody image in the brain. Journal of Consciousness Studies , 15, 5-16. http://www.imprint.co.uk/jcs_15_1.html#rama Ramachandran, V. S., & Hirstein, W. (1998). The perception of phan- tom limbs. The D. O. Hebb lecture. Brain, 121, 1603-1630. http://dx.doi.org/10.1093/brain/121.9.1603 Ramachandran, V. S., & McGeoch, P. D. (2007). Occurrence of phan- tom genitalia af ter gen der reassignment s urgery. Medical Hypo theses, 69, 1001-1003. http://dx.doi.org/10.1016/j.mehy.2007.02.024 Rauch, S. L., Shin, L. M., Dougherty, D. D., Alpert, N. M., Orr, S. P., Lasko, M., Mackli n, M. L., Fischman, A. J., & Pitman, R K. (1999). Neural activation during sexual and competitive arousal in healthy men. Psychiatry Research, 91, 1-10. http://dx.doi.org/10.1016/S0925-4927(99)00020-7 Ruhe, H. G., Maso n, N. S., & Schene, A. H. (2007). Mood is ind irectly related to serotonin, norepinep hrine and dopamine levels in humans: A meta-analysis of monoamine depletion studies. Molecular Psy- chiatry, 12, 331-359. http://dx.doi.org/10.1038/sj.mp.4001949 Smith, Y. L., van Goozen , S. H., Kuip er, A. J., & Cohen-Kettenis, P. T. (2005). Transsexual subtypes: Clinical and theoretical significance. Psychiatry Research, 137, 151-160. http://dx.doi.org/10.1016/j.psychres.2005.01.008 Sollberger, D. (2013). On identity: From a philoso phical point of view. Child and Adolescent Psychiatry and Mental Health, 7, 29. http://dx.doi.org/10.1186/1753-2000-7-29 Stafford, N. (2013). Germany is first European country to recognise third sex on birth certificates. BMJ, 22, Article ID: f5249. http://dx.doi.org/10.1136/bmj.f5249 van Dijk, M. T., van Wingen, G. A., van Lammeren, A., Blom, R. M., de Kwaasteniet, B. P., Scholte, H. S., & Denys, D. (2013). Neural basis of limb ownership in individuals with body integrity identity disorder. PLoS One, 8, Article ID: e72212. http://dx.doi.org/10.1371/journal.pone.0072212 Viard, A., Piolin o, P., Desgranges, B., Chételat, G., L ebreton, K., Lan - deau, B., Young, A., De La Sayette, V., & Eustache, F. (2007). Hip- pocampal activation for autobiographical memories over the entire lifetime in healthy aged subjects: An fMRI study. Cereb Cortex, 17, 2453-2467. http://dx.doi.org/10.1093/cercor/bhl153 Zucker, K. J., Wood, H., Singh, D., & Bradley, S. J. (2012). A devel- opmental, biopsychosocial model for the treatment of children with gender identity disorder. Journal of Homosexuality, 59, 369-397. http://dx.doi.org/10.1080/00918369.2012.653309
|