1. Introduction
Liposarcoma is a relatively uncommon mesenchymal tumor [1] .
This tumor originating from the spermatic cord is exceptional, with approximately 100 cases reported in the literature [2] . Clinical diagnosis is difficult. Inguinal orchidectomy is the standard treatment for this tumor with a well-known local recurrence risk after surgery.
2. Case Report
A 42 years old man, with past history of right inguinal hernia repair 15 years back, presented with a left inguinoscrotal hernia.
The patient underwent exploratory surgery via a left inguinal canal approach, during which a hernia associated with a mass located on the spermatic cord was discovered (Figure 1).
We proceeded with tumorectomy of the mass associated with Lichtenstein repair of the hernia.
Histopathology examination of the tumorectomy specimen confirmed an undifferentiated liposarcoma or a high grade myxofibrosarcoma.
Additional immunohistochemical study was performed showing a diffuse positivity of tumor cells staining with anti-MDM2 eliminating the diagnosis of high-grade myxofibrosarcoma and confirming the diagnosis of sclerosing variant of well differentiated liposarcoma (Figures 2(A)-(D)).
3. Discussion
Liposarcomas represent 7% of tumors of the spermatic cord [3] , they are rare tumors The largest series being that of Coleman et al. [4] , with 47 cases reported from 1982 to 2001. The few case reports reveal a predominance of retroperitoneal locations followed by the pelvis (bladder-prostate-vagina-cervix). Very few cases of paratesticular sarcomas and spermatic cord have been reported in the literature.
These tumors are rarely diagnosed and form a spectrum of lesions of variable aggressiveness.
In the literature, this tumor affects adult patients with variable ages ranging from 16 to 88 years [5] [6] .
Clinically, liposarcoma of the spermatic cord manifests in the form of a firm, painless nodular mass variable in size. It can be enormous.
Histologically, World Health Organization (WHO) classification of soft tissue tumors recognizes five subtypes of liposarcoma which can be divided in three distinct entities by their locations, their epidemiology, their clinical expressions and their imaging profiles [7] [8] .
Differential diagnosis of a lipoma with a well-differentiated liposarcoma can be difficult. However, over expression of MDM2 and/or CDK4 establishes the diagnosis, although this over expression is neither 100% sensitive (MDM2) or specific (CDK4), making the assessment of surgical margins delicate [8] .
The recommended treatment for liposarcoma of the spermatic cord consists of a surgical excision of the mass with radical orchidectomy via an inguinal canal [9] [10] .
Radiation therapy may be given in addition to surgical excision for large tumors whose complete resection might not be possible. But it remains the choice treatment to prevent local recurrences.
Radiotherapy reduces the local recurrence rate without direct impact on overall survival [11] .
Chemotherapy, on the contrary, has not proven its efficacy on these tumors [9] [11] . Liposarcoma evolves slowly; it is rather dominated by the frequency of relapses reported in 50%. This supports the need for local monitoring which could be prolonged [9] .

Figure 1. Mass developed at the expense of the spermatic cord.
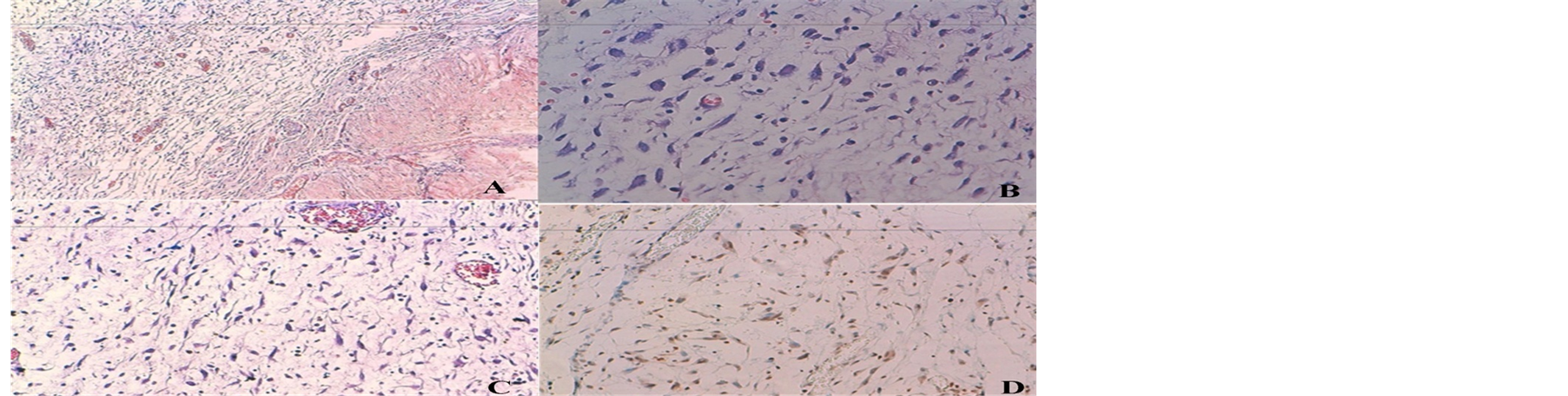
Figure 2. Histological images. (A) Myxoid stroma with fusocellular proliferation rich in capillaries with thickened walls (HES ×10); (B) Atypical tumor cells with irregular, hyperchromatic and pleomorphic nuclei with a few mitotic figures (HES ×40); (C) Fusocellular tumor proliferation on a rich fibromyxoid base (HES ×20); (D) Nuclear expression of tumor cells labelled with anti MDM2 antibodies in immunohistochemistry.
4. Conclusions
The liposarcoma of the spermatic cord is a rare tumor. Diagnosis of this tumor depends on histological examination.
The recommended treatment is inguinal orchidectomy. Although the prognosis is quite favorable, prolonged monitoring is required because of the risk of local recurrence which may occur very late.