High rate of injuries among students in Southern Nigeria: An urgent call to action ()
1. INTRODUCTION
Injuries constitute a major public health problem globally that accounts for more than 5 million deaths annually [1,2]. Recent projections hold that deaths resulting from injuries will increase from 5 million to over 8 million in 2020 [3-5]. The majority of all injury-related deaths occur in low and middle-income countries [6-8] where information is scarce regarding injury distribution, pattern and prevention [9], as well as lack of resources for care following injury [7].
Several epidemiological studies have been conducted on injuries. Many of such studies had focused on the types of injuries and their socio-economic status factors [10,11], intent of injuries [12], pattern of sport related injuries [13], perception of injuries [14,15] and risk behaviors and injuries [16,17]. Although, injury has imposed a huge public health burden, studies had reported that over 70% of injuries are preventable by simple and reasonable means [12,18,19].
Injury causation is a multi-factorial phenomenon in which place of injury plays a very significant role [20]. Other than homes, schools have been found to be a common place of injuries. Furthermore, children and adolescent students spend a significant amount of their time at schools where many factors predispose them to different types of injuries. For example, the contact of the students amongst themselves during sports-related activities and with the environment can act as possible contributing factors towards injury. The majority of injuries that happen in school are however non-fatal in nature [20].
The magnitude, characteristics and pattern of injury vary considerably from country to country [5]. Yet, school-based injury as a research problem has been largely ignored in developing countries including Nigeria. Few studies have described the pattern of injuries, and associated factors, in Nigeria. However, the majority of these studies have been hospital-based which provide information on severe injuries [21].
Notably, many childhood and adolescent injuries do not result in hospital attendance and, in any case, admissions to hospital present only a partial picture of the circumstances in which injuries occur. Also, there is limited access to hospital care in poor countries. More importantly, there is evidence that school age children often report injuries of which parents are not aware, thus for these older children, parents may not be able to report the full extent of injuries [22,23]. Thus on the premises of these limitations, it is evident that school-based study may be considered a simple and better approach to understand more accurately the pattern of injuries among children and adolescent.
However, the descriptive epidemiology of injury among adolescent students in Nigeria is poorly understood, as a result accurate information on injury among schooling adolescents is lacking. Therefore, to develop effective injury prevention strategies for schools in Nigeria and similar low-income settings, this study examined the distribution of injury among schooling adolescents with respect to sex, age, intent, mechanism and types of injury among adolescents in Southern Nigeria.
2. METHODS
2.1. Participants
A total of 600 students from selected schools in Delta State Southern Nigeria, voluntarily participated in the study. Of the 600 students, incomplete data were removed and 585 were included in the analysis. Of these, 60.9% were male while 39.1% were female. The slight male predominance in the sample was because one of the schools is same sex (boys only) school. The average age of male participants was 15.0 ± 2.0 years while for female was 15.2 ± 1.7 years. The average age of all participants was 15.1 ± 1.9 years. The participants cut across both public and private schools and their parents were from varied educational and occupational backgrounds.
2.2. Study Design, Data Collection and Survey Instrument
The study design was a cross-sectional survey conducted at Delta State Southern Nigeria between July and August, 2013 using a self-administered questionnaire on general school health survey. The injury section was adapted from previous published study [7]. Socio-demographic and injury related information was collected with a structured questionnaire. The questionnaires were administered to students by trained field interviewers who explained how to fill out the instruments to the students. The questionnaire was completed anonymously. Prior to the study, participants were pre informed of the significance of the research and informed consent was obtained from those who agreed to participate in the study. Also, approval was obtained from the respective schools.
The questionnaire consisted of different sections. Demographic data; such as age, sex, setting of residence etc. (1), Injury (2), students were asked to report injury sustained during the past one year. Respondents who reported at least one injury were requested to answer a series of questions related to the place, mechanism, types and intent of injury respectively etc. Also assessed were; highest level of parents’ education: This is based on students self-reports and is divided into four levels: 1) not educated (illiterate); 2) primary school; 3) secondary education; 4) tertiary education; and parents’ occupation: A more direct measure of the family economic situation was derived from a question reporting the occupation of the parents. This is based on students self-reports and responses were 1) none; 2) farming; 3) fishing; 4) business/trading; 5) civil servant; 6) others. In the analysis, where necessary, “no response” or “do not know” were combined with others.
2.3. Analysis
Descriptive analyses of age, sex, mechanism, intent, types of injury and days of activity lost due to injury, were performed using STATISTICA version 12.0 and GraphPad Prism version 5.0. Chi-square test was used to compare differences among subjects by socio-demographic characteristics. Student t-test was used for parametric variables and where appropriate one-way ANOVA was also used to assess significant differences. All reported P values were made on the basis of two-tailed tests. Differences were considered statistically significant at P value < 0.05.
3. RESULTS
3.1. Characteristics of the Participants
A total of 585 students participated in the study. Most of the participants were males (60.9%), and (39.2%) were females. The mean age of the study population was 15 years. More than half of the study population resided in the urban area (65.8%). Overall, 45.0% attend public school while 55.0% attend private school. The majority of the students’ parents had tertiary education (66.0%), while less than 2% were uneducated, and 46.7% of the students’ parents were into business/trading while less than 1% were unemployed (Table 1).
3.2. Prevalence of Self-Reported Injuries among the Participants
Overall, there were 549 self-reported injuries in past one year (93.8%) among the respondents (95.5% for males and 90.8% for females, P = 0.6696). Sex wise, prevalence of injury differ by age, school setting, school ownership and parents’ occupation (P < 0.05), but the difference in injuries with respect to parents’ level of education was not significant (P = 0.6111) (Table 2).
3.3. Cause of Injury
Overall, falls 293 (53.4%) was the leading cause of in-

Table 1. Characteristics of the participants.
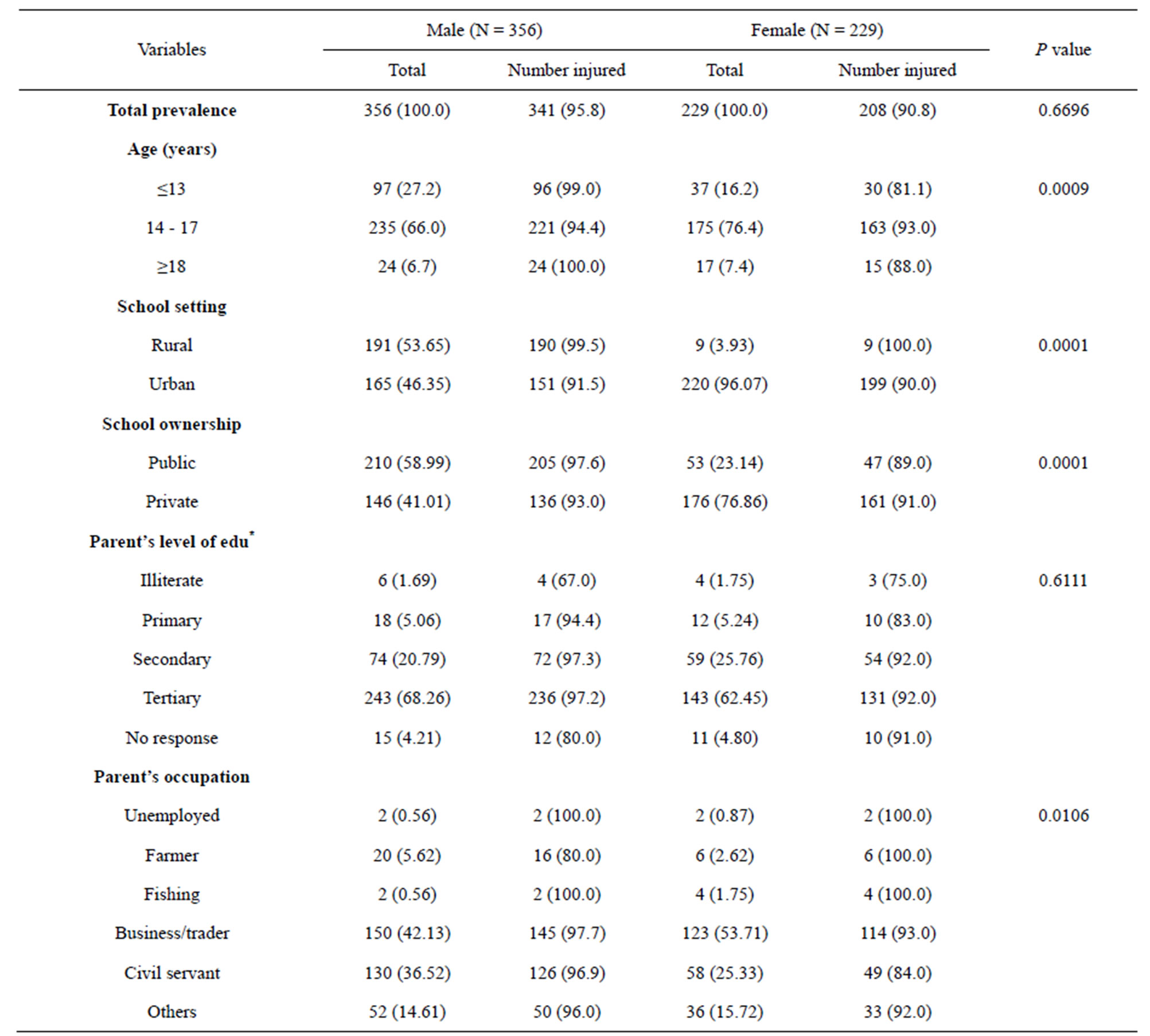
Table 2. Prevalence of self-reported injuries among the participants with respect to sex (N = 585).
*edu = education.
jury among the study population; followed by cuts/ stabs 52 (9.5%), and fire/heats 41 (7.5%). Sex wise, falls and animal bites were significantly higher in males compared to females [206 (60.4%) vs 87 (41.8%) P = 0.002, and 10 (2.9%) vs 0 (0.0) P = 0.016] respectively, while sexual assault and other were significantly higher in females than in males [9 (4.3%) vs 2 (0.6%) P = 0.004, and 47 (22.6%) vs 34 (10.0%) P = 0.001] respectively. In all cause of injuries, there was significant difference in the prevalence among female (P = 0.042), (Table 3). As expected, the cause of injury varied with age group (Table 4). Traffic injuries and falls decreases progressively with age while sexual assault, fire/heat, and stabs/cut increases with age. Injuries caused by animal bites were more common among aged ≤13 and ≥18 years. Although, there was no significant different in the cause of injury across age groups, in all cause of injuries, there was significant difference for aged ≥18 years (P = 0.012), (Table 4).
3.4. Intent of Injury
Overall, about 68.7% of the reported injuries were unintentional in nature, 13.3% were unintentional (self-inflicted) and 3.5% were intentional. Sex-wise, there was significant difference of the intent of injury (P = 0.001). Of the 341 injuries among males, 78.9% were unintentional while among female 46.2% of the 208 injuries
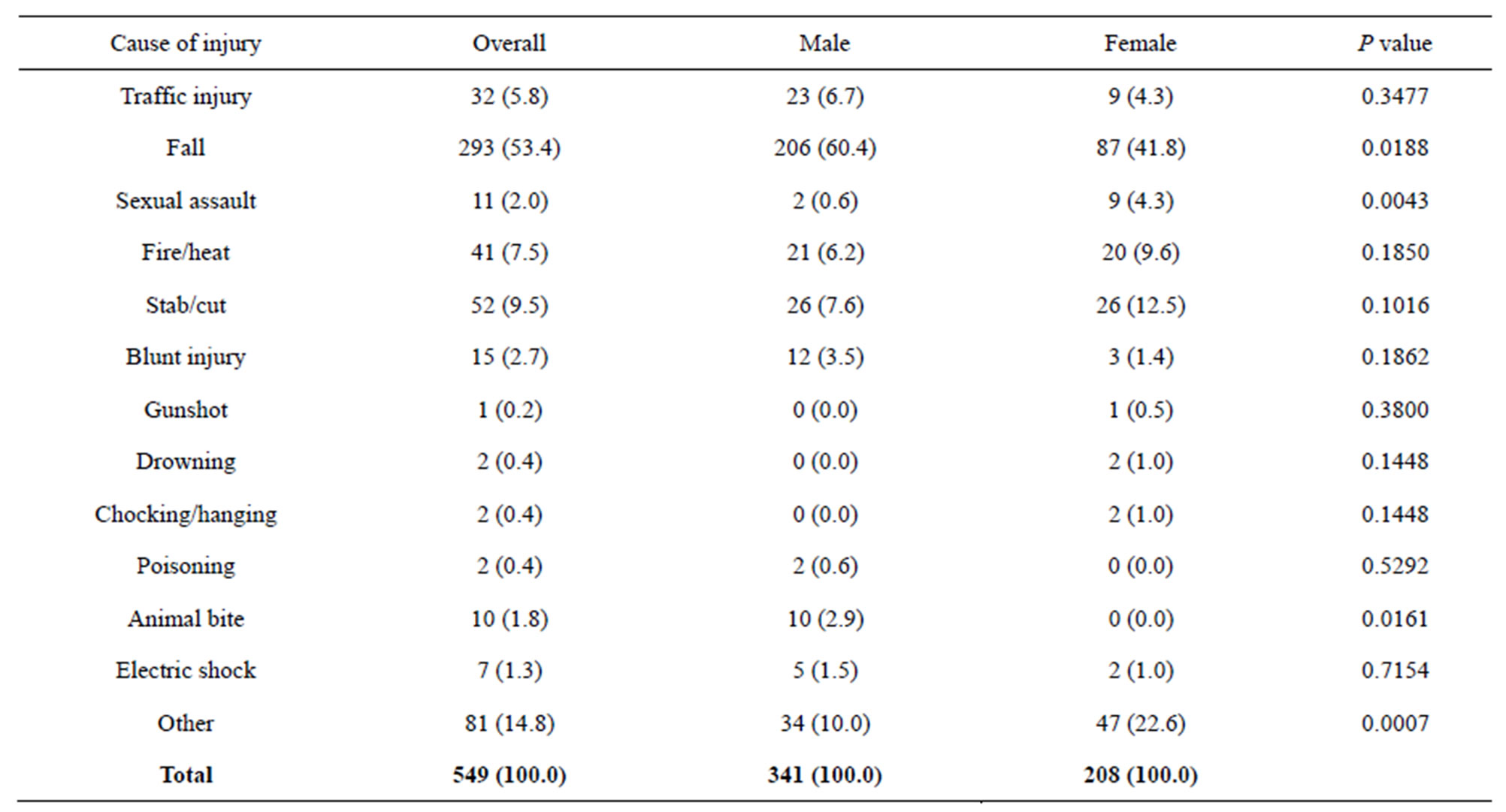
Table 3. Cause of injury in relation to sex.

Table 4. Cause of injury in relation to age.
were unintentional. The rate of unintentional (self-inflicted) and intentional injuries were higher among females compared to males (Figure 1).
3.5. Place of Injury
Generally, homes, schools and during sports were where injuries occurred mostly. There was significant sex difference in injury setting (P = 0.001), (Figure 2). For males, home injuries has the highest ratio (48.7%) followed by school (19.9%), and sport (15.0%), similarly, for females, home injuries has the highest ratio (46.2%) followed by others (20.7%), and school (13.9%), (Figure 2).
3.6. Types of Injury
Table 5 presents the distribution of types of injury in relation to sex and age. The commonly reported injuries were bruises and cuts/bite/open wounds followed by other unclassified injuries and sprains; least common were internal injuries and concussion. For all types of injures, there was significant sex difference within age groups (P < 0.05). Across age groups, the prevalence of fracture, bruise and sprain/strain was higher among males than females. Though significant sex difference was only observed among age group 14 - 17 years for bruise (P < 0.05). On the other hand, the prevalence of cut/bite/open wounds and unclassified injuries was higher among females than males (Table 5).
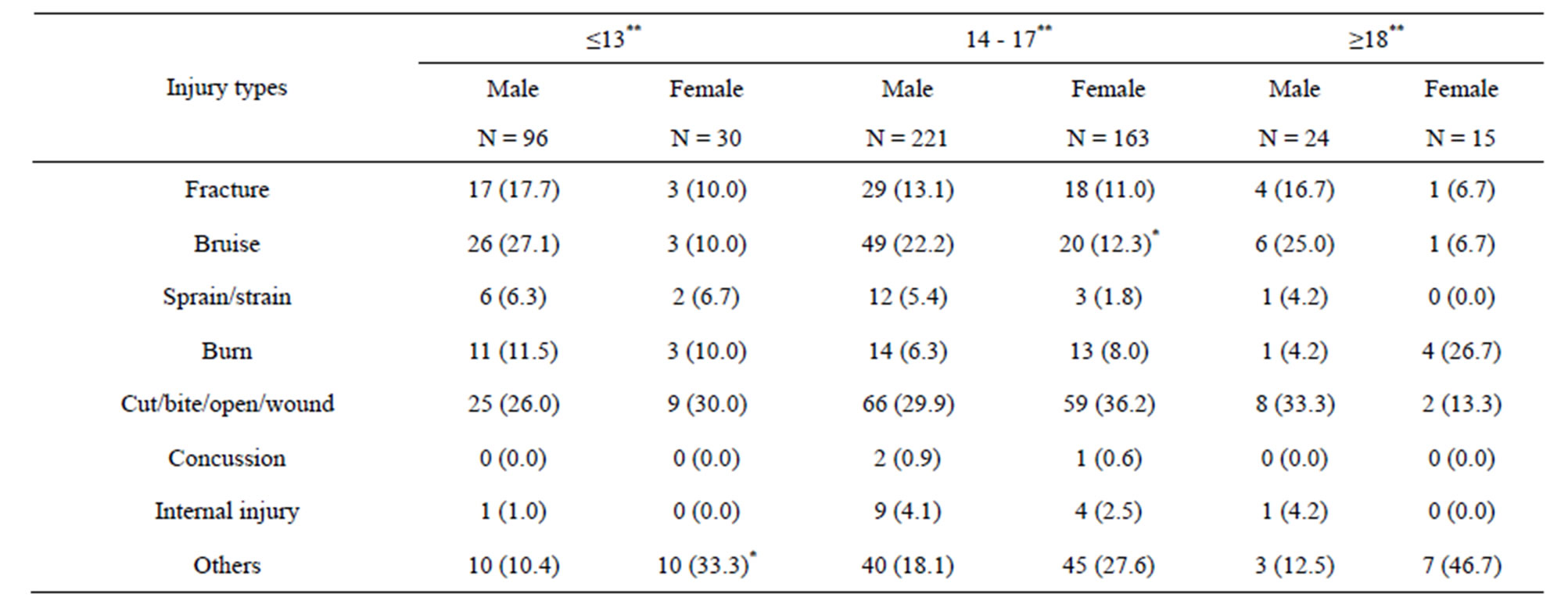
Table 5. Percentage distribution of injury types in relation to sex and age.
*P < 0.05; Significance values are for sex comparison for injury type. **P < 0.05; Significance values are for sex comparison for age group.
3.7. Initial Help Sought during Injury
Figure 3 presents information on initial help sought by the injured persons. There was significant variation on the category of persons from which help was sought (P = 0.0039). About 68.1% and 62.0% of the injured males and females respectively reported been helped by friend/ family at time of injury. For both males and female, only less than 8.0% were initially assisted by teacher.