Study of Lipocalin-2 Associated with Neutrophilic Gelatinases (uNGAL) in the Urine in Children with the Microbial Inflammatory Diseases of Kidneys and Urinary Tract ()


1. Introduction
In the recent years there has been an increase in the frequency of urinary system diseases in children, whose share in the structure of microbial inflammatory diseases of kidneys and urinary tract is up to 80%.
The prevalence of infectious and inflammatory diseases of the urinary system in childhood in the Russian Federation is 18 cases per 1000 pediatric population [1] [2]. The debut of this group of diseases is often observed on the background of upper respiratory tract infections RTI, intestinal infections , vaccination or exposure.
Urinary tract infections (UTI) are among the most common infectious diseases faced by pediatricians [3-[5]. Early diagnostics and treatment of UTI are very important [6] [7].
2. Materials and Methods
3. Results
As a result of comprehensive clinical laboratory and instrumental examination 2 groups were allocated. The first group included children with acute pyelonephritis (n = 15), the second group consisted of children with urinary tract infection (n = 15). Average age of the first group was 8.5 ± 0.6 years, of the second group―9.3 ± 0.9 years. Girls prevailed in both groups (Table 1).
All children with acute pyelonephritis marked symptoms of intoxication, fever from subfebrile to febrile values. 53.3% of patients during hospitalisation complained only about fever, making it difficult to diagnose and determing late hospitalization. 7 patients (46.6%) has abdominal pain syndrome, manifestating as anxiety in young children, some of the children’s condition required surgical consultation. 3 (20%) patients with pyelonephritis had disuria. In the group of children with urinary tract infection intoxication symptoms were less expressed, fever usually was subfebrile, 14 (93.3%) patients marked disuria in their clinical picture.
Laboratory tests of the first group revealed massive (more than 100 in sight) leukocyturia in 13 (86.7%) children, moderate (less than 100 in sight) leukocyturia―in 2 (13.3%) children. Microbiological examination of urine showed sowing of gram-negative flora (Escherichia coli, Klebsiella, Enterobacter) in 6 (40%) children.
12 (80%) children of the second group had moderate leukocyturia in urine analyses, massive leukocyturia was detected only in 3 patients (20%). 5 (33.4%) children had urine sowing of gram-negative flora (Escherichia coli).
Tubular disorders prevailed in children with pyelonephritis and were characterised by hyposthenuria, isosthenuria and nocturia. In the group of children with the UTI the decrease of concentrating renal function was registered much less often (Table 2).
Analyzing leukocytes blood level, ESR acceleration, CRP increase and leukocyturia it should be noted that children with active current microbial inflammatory process in the renal tissue had higher rates than children from the UTI group (Table 3, Image 1). Violation of the concentrational function is found in the children with hyperoxaluria or hypercalciuria.
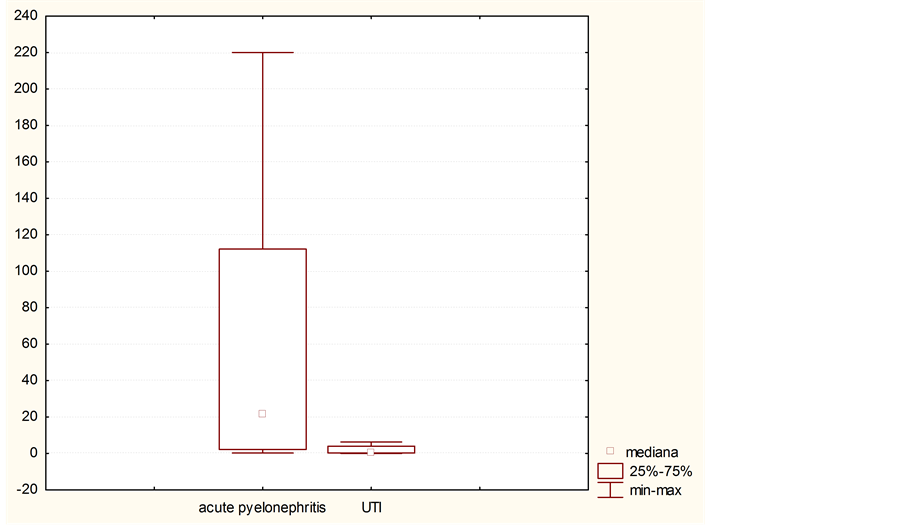
Image 1. The level of CRP in children with acute pyelonephritis and urinary tract infection on the day of admission to the hospital.
![]()
Table 1. Distribution of children by age and sex.
![]()
Table 2. Characteristics of kidneys’ functional state.
![]()
Table 3. Laboratory findings in children with acute pyelonephritis and the UTI during admission.
The uNGAL level in children with active current microbial inflammatory process in kidney tissue was significantly higher (Image 2) than in children from the UTI group (19.73 ± 12.37 and 0.85 ± 0.54 ng/mg of creatinine, respectively, р < 0.05). The uNGAL/ Cr excretion level in children with the UTI did not exceed 2.5 ng/ml and in patients with pyelonephritis the uNGAL/Cr excretion was 5.7 ng/ml and more.
In the group of children with acute pyelonephritis a direct correlation of moderate strength (r = 0.72; p < 0.05) was between the uNGAL/Cr excretion level and the amount of blood leukocytes, as well as the CRP blood level (r = 0.67; p < 0.05).
To assess kidneys’ function we defined glomerular filtration rate by Schwartz in children of the two groups (Table 4). All children with the UTI and most of the children (80%) with acute pyelonephritis had normal levels of GFR, however 2 (13.3%) children were diagnosed with hyperfiltration and 1 (6.7%) child was diagnosed with moderate decrease of glomerular filtration rate. In the first group of children a weak correlation between GFR and the uNGAL/Cr was found (r = 0.46; p < 0.05).
All children of the first group had voiding cystourethrography 3 months after the decrease in pyelonephritis activity, according to its results no vesicoureteral refluxes and malformations of urethra and urinary bladder were found. 13 (86.6%) children with pyelonephritis 6 and more months after its attack had sclerotic foci in kidneys’ parenchyma found by static nephroscintigraphy. 7 of them had 1 - 2 foci, 4 patients had 2 - 3 foci, 2 children were diagnosed with 4 foci without decrease of accumulative-excretory function of kidneys. In the group of children with the UTI sclerotic foci and accumulative-excretory kidneys’ disfunctions were not found by using static nephroscintigraphy. Strong positive correlation (r = 0.71; p < 0.05) was established between the
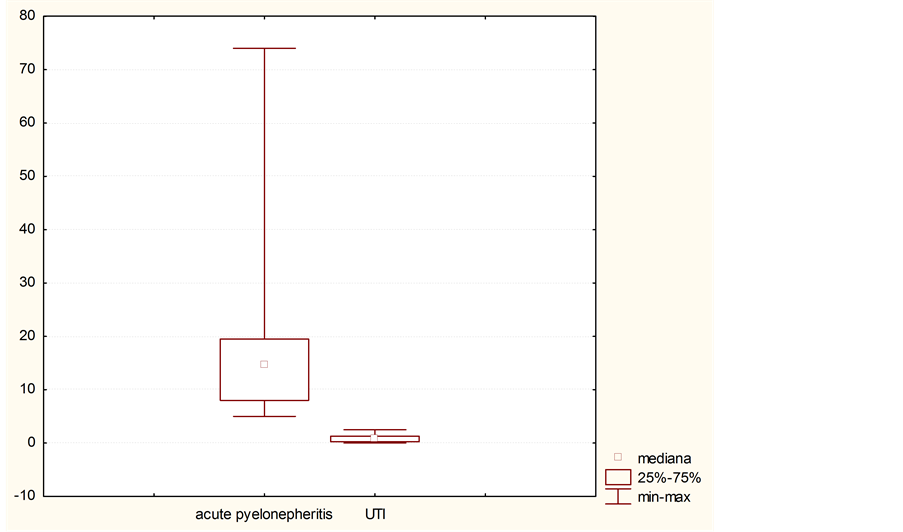
Image 2. The level of uNGAL/Cr in children with acute pyelonephritis and urinary tract infection at admission to the hospital.
![]()
Table 4. Indicators of Glomerular Filtration rate (Schwartz formula).
uNGAL increase level during the acute pyelonephritis and damage degree of renal parenchyma in children with acute pyelonephritis according to the results of the static nephroscintigraphy.
4. Discussion
Early diagnosis of the presence and degree of renal parenchyma damage, especially in the young children, is very difficult, but the correct assessment allows us to choose an adequate therapy. Published data about the possibility of non-invasive assessment methods vary. Inflammation that occurs on the background of the tissue damage is accompanied with a production of inflammatory cytokines, acute phase proteins, the excretion of enzymes, the identification of which may indicate severity of the inflammation, increases at the destruction of the tubules [16]-[18]. In our study we found that the uNGAL urine level depends on the degree of renal parenchyma damage. Positive correlation was revealed between the uNGAL/Cr and such acute phase indicators in blood as CRP and leukocytosis in children with acute pyelonephritis. In the patients of the first group symptoms of intoxication prevailed in clinical picture, febrile fever was more common, erythrocyte sedimentation rate significantly accelerated, tubular renal dysfunctions and massive leukocyturia were diagnosed.
Static DMSA-nephroscintigraphy is the “gold” standard of renal parenchyma damage diagnostics and of determination of the amount and localisation of nephrosclerosis foci [19] [20]. However, despite being highly informative method of renal parenchyma damage diagnostics, nephroscintigraphy currently remains an expensive method of examination and the possibility of its implementation is limited even in foreign clinics and diagnostic centres [21].
The dependence between the uNGAL/Cr excretion level and the amount of renal scars in children after acute pyelonephritis established according to the clinical laboratory data during an acute period of disease, confirmed by the static DMSA-nephroscintigraphy. To form a cohort of patients in need of static DMSA-nephroscintigraphy after acute pyelonephritis we can use high the uNGAL/Cr excretion level as a marker at the acute phase of the disease. Category of patients undergone severe course of acute pyelonephritis also needs non-invasive method of monitoring the state of tubular nephron part, therefore more research of the uNGAL excretion dynamics is needed in the large patients’ groups.
Received data points to the need of further research of the uNGAL significance as one of the diagnostic markers of renal parenchyma damage. Considering this it is important to determine the diagnostic significance of the uNGAL at the exacerbation of chronic microbial and inflammatory diseases of the urinary system, latent inflammatory process, at the development of pyelonephritis on the background of the congenital abnormalities of the urinary system, as well as an early marker of renal tissue scarring.
5. Conclusion
The determination of the uNGAL excretion in urine is available and non-invasive method for the early detection of renal parenchyma damage, an increase of differential diagnosis quality and a choice of curative tactics of the patients with microbial inflammatory diseases of the urinary system. However, further studies in the large groups of patients, conducted in dynamics, are required to confirm the results.