Cribriform Adenocarcinoma Salivary Gland-Type of the Nasopharynx: Case Report and Review of the Literature ()
1. Introduction
Adenoid cystic carcinoma (ACC) is the most common histological subtype of salivary gland malignancies, but it is very rare in the nasopharynx, with relatively few cases reported in the literature. Some of these cases are poorly documented and not well characterized given to the rarity of cases. The ACC is characterized by a slow evolution but locally aggressive and high risk of recurrence. The optimal treatment remains debated, even though recent evidence provides support for a multimodality approach [1] [2] .
2. Case Presentation
We report a case of a 70-year-old woman, diagnosed and treated in radiotherapy department at Hassan II University Hospital in Morocco. The patient had in her medical history a cardiac failure, but no prior smoking or radiation. She presented 6 months before the diagnosis, unilateral hearing loss with nasal obstruction. Clinical examination found a 3-centimeter lymph node of the IVth left cervical area. Nasopharyngeal endoscopy had showed a tumor process occupying totally the nasopharynx. Chest x-ray and blood tests were normal. A contrast computed tomography (CT) of the facial cranium and neck had showed an extensive lesion occupying all the nasopharynx with absence of bony erosion or involvement of adjacent structures. It revealed also two cervical ganglions with central necrosis in the jugulo-carotid area. The patient underwent a biopsy of the nasopharyngeal mass, under general anaesthesia. Histology revealed a cribriform adenocarcinoma salivary gland-type (Figure 1).
Regarding treatment strategy, Patient received radiotherapy alone without chemotherapy given to the geriatric assessment and co-morbidities. She received a total of 70 Gy of the radiations, divided into 2 Gy per session over a period of 7 weeks. Follow-up with nasal endoscopic examination and nasopharyngeal CT was performed and showed no recurrence 12 months after the end of treatment.
3. Discussion
Primary salivary gland type carcinoma is one of the most common malignancies of salivary gland origin, with widely varied histological subtypes, diverse clinical behaviours, and different prognoses [1] . Previously termed “cylindroma” by Bilroth in 1856, the adenoid cystic carcinoma (ACC) is the most common histologic subtype of the salivary gland malignancies, but it is very rare in the nasopharynx. A few cases had been reported in the literature. It is the most common malignancy of the submandibular and minor salivary glands and it can be seen in other glandular tissues such as the lacrimal glands, ceruminous glands of the external auditory canal, esophagus, breast, prostate, uteri cervix and Bartholin’s glands [3] [4] . In the nasopharynx, the primary salivary gland type carcinoma is an uncommon malignancy that represents about 0.48% of all nasopharyngeal cancers [5] , likely owing to the low density of salivary gland tissue in the nasopharynx. Within the nasopharynx, adenoid cystic carcinoma is the most common salivary gland tumor, followed by adenocarcinoma [5] . This tumor is considered to be derived from nasopharyngeal surface epithelium rather than from underlying minor salivary glands, based on histological appearance and immunohistochemical staining profile [6] . ACC affects women predominantly and usually occurs in the 5th and 6 th decade of life and is rare in people younger than age 20 [5] -[7] . Regarding histology, it presents three patterns, cribriform, tubular and solid. The cribriform (landular) pattern is the most classic and best recognized appearance, characterized by islands of basaloid epithelial cells that contain multiple cylindric, cyst-like spaces resembling swiss cheese. These spaces often contain a mildly basophilic mucoid material, a hyalinized eosinophilic product, or a combined mucoid hyalinized appearance. Sometimes, the hyaline-
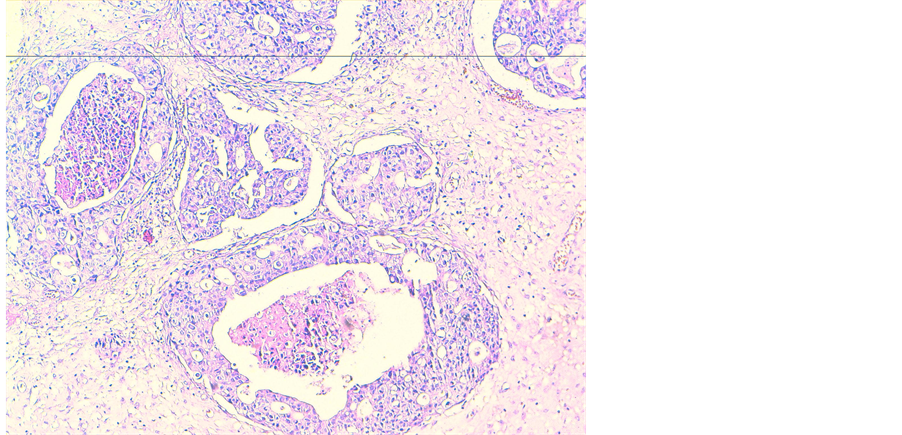
Figure 1. HES ×400 definitive histologic examination indicating a cribriform adenocarcinoma salivary gland-type.
ized material also surrounds these cribriform islands, or small strands of tumor are found embedded within this hyalinized stroma. The tumor cells are small and cuboidal exhibiting deeply basophilic nuclei and little cytoplasm. These cells are fairly uniform in appearance, and mitotic activity is rarely seen [8] . Mitotic figures are generally scarce in cribriform and tubular areas; however they are easily visualized in solid standards that have been associated with the worst prognosis [9] . The histological type found in our patient was the cribriform type, which is a subtype with better prognosis.
Adenoid cystic carcinoma of the nasopharynx has tendency to invade the nerves and to propagate perineurally (80% of the specimens found invaded). Even if some studies showed that there is not strong correlation between survival and perineural invasion alone, the majority believes that the invasion of a main nerve trunk or at least a large nerve by the tumor means a poor prognosis [6] [10] [11] . ACC typically presents an indolent and slow growth associated to frequent late distant metastases, which are together with local recurrences, the reasons for the low long-term survival rate [2] -[4] [12] , in 70% of cases metastases are localized at lung, it can also be done to the liver, bone [11] [13] .
Multiple treatment modalities exist for the treatment of salivary gland tumors of the nasopharynx [14] . The best treatment for ACC, contains radical surgical resection followed by radiotherapy [7] [15] -[21] . In cases of nasopharyngeal ACC, the frequent perineural and perivascular infiltrations, associated with the anatomical characteristics of the nasopharynx, however, make the surgical approach risky on account of technical difficulties, due substantially to the proximity of surgical margins to critical neural and vascular structures [22] . The traditional therapeutic approach for patients with high-grade or unresectable (T4) disease is radiotherapy. A surgical approach is more appropriate for low-grade, low-stage adenocarcinomas [6] .
Given the proven radiosensitivity of the ACC, this tumour is, in fact, regarded as a radiosensitive, even if not radiocurable, neoplasm, thus exclusive radiotherapy can determine a reduction in tumour volume with a meaningful improvement in the clinical symptoms [23] [24] . Vikram et al. reported regression of the tumoural mass in 96% of 49 patients treated only with radiotherapy, although in 93% of the cases they observed recurrence of the disease within 5 years [22] . Although the surgical approach with attempts of oncological radicality, followed by radiotherapy, remains the treatment of choice for ACC, but exclusive radiotherapy is a good option in case of impossibility of surgery for general reasons or for technical difficulties. It is a valid therapeutic alternative guaranteeing good control of the disease and minimal side-effects. Moreover in the literature, many studies have shown that survival rates, over a long period of time, in patients with nasopharyngeal ACC do not seem to be significantly influenced by different (more or less aggressive) types of treatment [1] [22] [23] .
In our patient, given to the impossibility of total resection, because of the locoregional extension, furthermore its geriatric assessment and co-morbidities, an exclusive radiotherapy was indicated. The evolution was marked by disease control at the imaging and endoscopy.
4. Conclusion
Nasopharyngeal cribriform adenocarcinoma salivary gland-type is an uncommon tumor with only very few cases reported in the literature. The treatment management must be discussed in a multidisciplinary approach for each case. Radiotherapy alone seems to be a good option in case of localized disease especially when chemotherapy is not applicable. But data are still insufficient for an appropriate treatment protocol or an accurate prognosis prediction for the disease and we still need larger clinical series and longer follow-up periods to establish the best treatment strategy for these patients.