Intestinal parasitism in schoolchildren in 2005, 2006 and 2007: A real challenge to overcome by the national deworming campaign in Northwestern Mexico ()
1. INTRODUCTION
Intestinal parasitism has been recognized as a public health problem worldwide [1,2], because they are associated with malabsorption and growth disturbances [3,4]. Intervention programs have been introduced for the control of parasitic helminth infections and they have significantly reduced their prevalence, intensity and morbidity using mebendazole and albendazole [5]. In Mexico, these infections remain a public health problem in the population [6]. In 1987, Mexican schoolchildren were considered the most vulnerable group to these infections, and 35.2 and 83.2 million Mexicans were affected by helminths and protozoa, respectively [7]. This motivated the launch of a deworming campaign in 1993 influenced by the effectiveness of global programs for control of helminths; the recommendation by the World Health Organization; the political will of the Mexican government; and the infrastructure provided by the Health National Week [8]. The Ministry of Health determined that albendazole was provided to 95% of children (6 - 14 years old) to reduce the prevalence and excretion of helminth eggs, and re-infection and morbidity rates [8]. Chemically, the albendazole is methyl 5-(propylthio)-2- benzimidazolecarbamate and its molecular formula and weight are C12H15N3O2S and 265.34 respectively, and binds to tubulin preventing the formation of microtubules and cell division resulting in impairment of nutrient uptake by the parasite [5]. Between 1993 and 1998 the program reduced the prevalence of Ascaris lumbricoides and Trichuris trichiura from 20% to 8% and 15% to 11%, respectively [8] in more than 90,000 Mexican children. In 1995, the prevalence of Giardia duodenalis was estimated at 32% in Mexico [9] and remained the most important protozoan infection (14% to 49%) in northwestern Mexico [10,11]. Entamoeba histolytica is another protozoan pathogen with prevalence up to 50% in southern Mexico [12] but appears to be less prevalent than giardiasis in northwestern Mexico [10,11,13-15]. Currently, the Ministry of Health continues to administer a single dose of 400 mg twice a year of albendazole to schoolchildren in Mexico, but the intestinal parasites are recognized to contribute to morbidity of the general population of northwestern Mexico [13]. Therefore, the aim of this study was to investigate the current prevalence of intestinal parasites in children who are receiving periodically albendazole in northwest Mexico.
2. METHODS
This cross-sectional study was conducted in September 2005, September 2006 and April 2007 in Sonora (northwest Mexico). Sonora is bordering to the east with the state of Chihuahua, south to the state of Sinaloa, west to the Gulf of California, and north to the U.S. state of Arizona. The summer average temperature is 38˚C (June to August) and from 5˚C to 30˚C in winter (September to January). In 2005, the total population of Sonora was estimated in 662,000 and 60% of this was under 15 years of age [16]. Ten public primary schools of 3 municilities of Sonora were selected in suburban and rural areas based on high gastrointestinal infection rates in the population [13]: low socioeconomic status in the areas around the schools [17] and administration of twice a year for a single dose (400 mg) of albendazole by the national deworming campaign [8]. Up to date, no epidemiological surveillance to investigate the prevalence of intestinal parasitic infections has been conducted in Northwestern Mexico. A total of 3387 schoolchildren were officially enrolled in the schools selected from September 2005 to June 2007 [18]. The purpose of this study was described to the personnel of health services, municipalities, schools, parents and schoolchildren. All children were invited to participate while three plastic containers per child were distributed for stool collection. Only 1203 (35%) of the total of 3387 children participated in the 3 sampling periods. Administration of albendazole by the deworming campaign was confirmed by the school personnel.
A written consent was obtained from parents or guardians of the 1203 participating children. Of the remaining 1313 from the total 3387 enrolled schoolchildren, 1159 were unwilling to participate and 154 did not meet the study criteria (disabled, supplemented or medicated). Approval to conduct this study was granted by the Ethical Review Committee of the Research Center for Food and Development. If required, infected children received the proper treatment by the Ministry of Public Health.
Stool samples were collected and transported to the Research Center for Food and Development. Samples were stored at 5˚C and 7˚C for 24 - 72 hours prior to analysis by the techniques of Faust and Kato-Katz [19]. Faust was used for identification of protozoan cysts of G. duodenalis (Figure 1), Entamoeba histolytica (Figure 2), Entamoeba dispar, Entamoeba moshkovskii [20] , Entamoeba coli, Endolimax nana and Iodamoeba butschlii and helminth eggs of A. lumbricoides, T. trichiura and H. nana (Figure 3). Kato-Katz was used to count the number of eggs per gram of feces (epg) of helminth infections (defined as intensity of infection) using the 40x objective, and the final value was the average of epg divided per the number of samples (3.2 or 1) provided per child. The epg was calculated by multiplying twenty

Figure 1. G. lamblia. Immature binucleated infective cyst stained in iodine (40×).

Figure 2. E. histolytica. Mature 2 visible nuclei infective cyst iodine-stained (40×).

Figure 3. H. nana. An inner membrane with two poles and polar filaments spread out between the two membranes (40×).
times the number of eggs counted in 50 mg of feces. Infection was defined as the state with one or more species of parasites, poliparasitism with two or more species of parasites, helminth infection only with species of helminth parasites, protozoa infections only species of protozoan parasites.
The prevalence of intestinal parasitism was the percentage of children with parasites spp. in any of the fecal samples provided. The Fisher test was used to test the difference between proportions (prevalence of parasites spp.). The intensity of infection with helminth species was expressed as a median with confidence interval and Kruskal Wallis to test the difference between the ageintensity data (epg). Data were analyzed using the Number Crunching Statistical System 2007, Version 1.6.0. (Utah 84037.com.USA). P-values < 0.05 were considered as statistically significant.
3. RESULTS
A total of 450, 389 and 364 children participated in September 2005, September 2006 and April 2007 respectively. The mean ages were 7.7 (±1.2), 8.1 (±1.3) and 7.9 (±1.3) in the 3 sampling periods. 220 (49%), 217 (56%) and 199 (55%) were girls in 2005, 2006 and 2007 respectively. No differences were found between the proportions of boys and girls (χ2 = 2,342, df = 1, P = 0.7003 in 2005; χ2 = 3.476, df = 1, P = 0.6231 in 2006 and χ2 = 1.936, df = 1, P = 0.1455 in 2007). The overall prevalence of intestinal parasites between boys and girls was 48% vs. 44% (P = 0.708) in 2005; 29% vs. 35% (P = 0.357) in 2006; and 41% vs. 42% (P = 0.8466) in 2007. In addition, no difference was found between the prevalences of parasites spp. by gender (data not shown). A total of 1231, 861 and 890 fecal samples were collected in September 2005, September 2006 and April 2007 respectively. 62% and 26% of the children provided 3 and 2 stool samples in September 2005; 47% and 26% provided 3 and 2 samples in September 2006; and 63% and 19% provided 3 and 2 stool samples in April 2007. High prevalences for intestinal parasitic infections, and protozoa infections were found in 2005, 2006 and 2007 respectively (Table 1). H. nana and G. duodenalis also showed important prevalences. E. histolytica/dispar/ moshkovskii showed a low prevalence in all sampling periods. Helminth infections by A. lumbricoides, T. trichiura and hookworms were not detected in this study.
The prevalence of intestinal parasites showed an increasing trend with age (group 6 - 7.9 vs. group 8 - 9.9, P = 0.2796, and group 6 - 7.9 vs. group 10 - 11, P = 0.2773 in 2005; group 6 - 7.9 vs. group 8 - 9.9, P = 0.8770, and group 6 - 7.9 vs. group 10 - 11, P = 0.6631 in 2006; and group 6 - 7.9 vs. group 8 - 9.9, P = 0.2284, and group 6 - 7.9 vs. group 10 - 11, P = 0.2282 in 2007) (Table 2).
During the study, 50 of 450 (September 2005), 42 of 389 children (September 2006), and 41 of 364 (April
Table 1. Prevalence of intestinal parasites in 1203 schoolchildren of 10 primary schools during 3 sampling periods in northwestern Mexico.

CI: Confidence interval at 95%; +: Pathogens; −: No pathogens; Δ: E. histolytica is pathogen and E. dispar and E. moshkovskii are no pathogens (These species were not confirmed in this study).
Table 2. Prevalence of intestinal parasites by age group in 1203 schoolchildren of 10 public primary schools during 3 sampling periods in northwest Mexico.
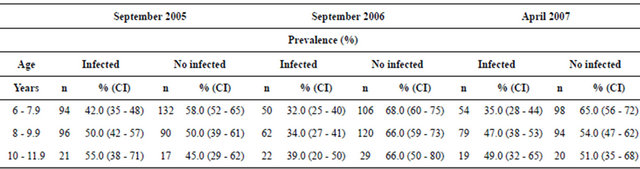
CI: Confidence interval.
2007), excreted a median of 520, 630 and 820 epg of H. nana respectively. From these children, 16 (32%) and 16 (32%) children in 2005, 20 (48%) and 8 (19%) in 2006, and 4 (5%) and 19 (26%) in 2007 showed intensities ≤100 and ≥1000 epg respectively. The intensity of infection with H. nana showed a tendency of increasing with age in this study (Table 3).
4. DISCUSSION
Almost half of our children were suffering from intestinal parasites. Previous local publications considered to G. duodenalis to be the predominant pathogenic protozoan [11,12,15] and H. nana followed by T. trichiura and A. lumbricoides as the most important helminth species in northwest Mexico. Our study confirmed that G. duodenalis is the predominant protozoan species and H. nana as unique helminth detected in the study sites. Before the Mexican campaign (1993), prevalences of 58.9% in 1957 and 19.5% in 1968 for ascariasis [21] and prevalences of 39.7% in 1957 and 19.5% in 1978 for trichuriasis were published in Mexico [22, 23]. Similarly, the prevalence of giardiasis and amibiasis ranged from 14% to 16% and 12% to 21%, respectively from 1982 to 1984 in children under 15 years of age in different Mexican regions [24-26]. After 1993 [27-30], the prevalences of T. trichiura, A. lumbricoides, H. nana, G. duodenalis and E. histolytica were peaking around 16%, 8%, 15%, 24% and 60% respectively in the general population. This revealed a substantial reduction of trichuriasis and ascariasis, but a persistent giardiasis, hymenolepiasis and amebiasis in Southern Mexico. Probably this pattern was associated with the national deworming campaign and this may explains the absence of ascariasis and trichuriasis in our study. Furthermore, no differences were found in the prevalence of intestinal infections between boys and girls. Studies in Mexico and other Latin American countries have found similar findings probably due to similar transmission risk activities related to poor hygiene between genders [31]. On the other hand, the prevalence of intestinal parasites showed an increasing trend with age in our study. Khosrow, et al. [32], published a similar finding in 405 Iranian schoolchildren (6 to 10 years) without identifying the risk factors. This probably reflects the major attention from parents to younger children that may favor that older children are more easily infected. It is also probable, the higher the prevalence of H. nana, the greater its intensity in this study. In spite of the deworming campaign, the persistence of these infections may be a reflection of poverty, clean water supplies and poor hygiene practices of our children’s families. This study is not evaluating the effectiveness of the deworming campaign, due to inappropriate sample size and lack of a methodological strategy of sampling. Nevertheless, we recognized that the Mexican campaign is aimed primarily at the soil-transmitted helminthiasis and albendazole is the drug of choice. However, a passive attitude should not be taken by the authorities meanwhile our study site’s population is at high risk of acquiring giardiasis and hymenolepiasis. Our schoolchildren had received albendazole in April 2005, April 2006 and October 2006. This suggested that health education strategies should be integrated into the deworming campaign and decision-makers should improve the quality of basic services provided to the study sites, since albendazole alone will not improve health conditions of our study children.
5. CONCLUSION
This study provided data on the current prevalence of intestinal parasitic infections in schoolchildren of marginal communities of northwestern Mexico and who are periodically treated with albendazole by the national campaign. Results showed that the parasite spp. causing intestinal infections in our study children are not apparently sensitive to the twice yearly administration of albendazole (400 mg/day). It is well recognized that these infections have multifactorial origin and probably a campaign that administers albendazole combined with
Table 3. Distribution of eggs of H. nana per gram of feces in 133 schoolchildren by age group of 10 public primary schools during 3 sampling periods in northwest Mexico.

CI: Confidence interval.
other antiparasitic drug and accompanied with educational strategies may provide major benefits to the children of this study.
6. ACKNOWLEDGEMENTS
Authors thank to the Q.B. Carmen Maria Lugo Flores in formatting the manuscript for the journal. This work was based on the knowledge and contribution of my Professors DWT Crompton and Stephen Phillips. We also thank the primary schools, academic staff, schoolchildren and the financial support granted by CONACYT (Funds SON- 2004-C01-005 MIXTOS) and the Secretaria de Educación Pública Estatal.