Epidemiological and Clinical Study of Cardiac Diseases in the Pediatric Department of the University Hospital Gabriel Touré (UH GT), Bamako (Mali) ()
1. Introduction
Pediatric heart disease represents an underestimated heavy burden in developing countries where efforts are focused mainly on the control of infectious diseases. The prevalence of congenital heart disease (CHD) is estimated at 9.1 per 1000 live births according to van der Linde et al. [1] and their increasing incidence in the order of 9.7, 9.9, and 11.1 per 1000 live births respectively at 1 week, 1 month and 1 year [2] . Although acquired heart disease (AHD), particularly rheumatic heart disease (RHD), was a global problem until the middle of the 20th century, it is now only a problem for developing countries. In addition, age-adjusted prevalence has decreased in many parts of the world, remaining high in Oceania, sub-Saharan Africa and South-East Asia [3] .
The prevalence of pediatric heart disease in sub-Saharan Africa is estimated to be around 8 per 1000 live births for CHD and at least 1 in 14 per 1000 RHD [4] . Management of these children heart diseases in the countries of sub-Saharan Africa and particularly in Mali still pose enormous difficulties of diagnosis and access to treatment, particularly surgical treatment, thus contributing to an increase in infant mortality and morbidity [5] . Performed studies found prevalence of 5.8% in Cameroon [6] , 1.5% among children in Uganda [7] , 21.5% in Mozambique [8] and 0.61% in Burkina Faso [9] .
In Mali, until recently, studies on heart disease were mostly clinic-based [10] and nowadays more and more with the contribution of echocardiography [11] [12] in cardiology departments. Our study is one of the few in the pediatric community to routinely use echocardiographic diagnosis with the aim of providing more accurate data and filling the data gap in the field of pediatric heart disease publications in UH GT.
2. Patients and Methods
Our study was conducted at the University Hospital Center (CHU) Gabriel Touré (GT), 3rd Reference Hospital, located in Commune III in Bamako and easily accessible to the majority of the population.
It was a retrospective study from January 1st to December 31st, 2015 on a representative sample of all children aged 0 to 15 years hospitalized in the pediatric department of UH GT for heart disease.
For acquired diseases specially rheumatic heart diseases we used the revised Jones criteria of 1992 [13] and all echocardiographies were performed by pediatric cardiologist. RHD was retained if a patient had:
1) history of RF (more than 3 months) or not
2) recent (less than 3 months ) or past episode of RF
3) clinical or echocardiographic finding of
- valvular heart disease (mitral regurgitation, mitral stenosis, aortic insufficiency/stenosis) compatible with rheumatic heart disease.
- myocardial involvement.
- pericardial involvement.
Inclusion was based on echocardiographic confirmation of the diagnosis. Suspected cases with no echocardiographic confirmation were not included.
We developed a survey formulary that allowed us to collect patients data from outclinic and hospitalization registers. Records on socio-demographic, clinical and echocardiographic data were collected. Data collection was realized under consideration of confidential aspects.
The data was analyzed using Microsoft Excel 2013 and Epi Info version 3.5.3. The Chi-square test was used for statistical tests, with p considered significant if less than 0.05.
The study was approved by the administration of the hospital after consideration of ethical aspects.
3. Results
During the study period, among 8613 hospitalized children, we found 103 cases of heart diseases, giving an hospital prevalence of 1.2%.
3.1. Epidemiological Characteristics
The age group 0 - 4 years was the most represented with 73.80%, mean age was 4.11 years from 1 day to 15 years. Sex ratio was 1.2.
Patients from consanguineous marriages accounted for 19.42% and parents were largely unschooled (65.05%). An history of prematurity and a maternal risk factor were found in respectively 01.94% and 06.80% of cases (Table 1).
3.2. Clinical Features
The circumstances of discovery were dominated by respiratory distress (93.20%), cyanosis (31.06%) and edema (26.21%). Fever on admission was found in 38.80% of cases. A proportion of 55.30% of patients had a failure to thrive. Heart murmur and tachycardia were the most represented cardiac signs with respectively 88.35% and 83.50%. Tachypnea was the predominant respiratory sign and found in 89.32% of cases (Table 2).
CHD were the widely found pathologies with 70.87% versus 29.13% of RHD (Diagram 1). CHD were discovered before 5 years (98.6%) and RHD after 5 years (87.3%) (Table 3) with a significant p value of 0.037.
The most common complications were hypoxic spells and cardiac failure in 13.60% and 08.74% of cases respectively (Table 2).
3.3. Echocardiographic Features
CHD were dominated by Ventricular septal defect (VSD), atrial septal defect (ASD), Tetralogy of Fallot (TF), atrioventricular septal defect (AVSD) respectively in 30.14%, 19.18%, 12.33% and 8.22% (Diagram 2).
RHD were dominated by mitral regurgitation (MR) (56.67%), presumed myocarditis (10%) and pericarditis (6.66%) (Diagram 3).
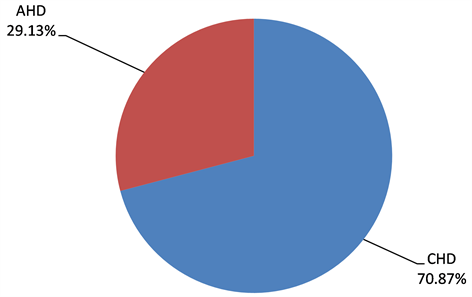
Diagram 1. Distribution of heart disease types for 103 patients in the pediatric department of the UH GT. CHD: congenital heart disease, AHD: acquired heart disease.
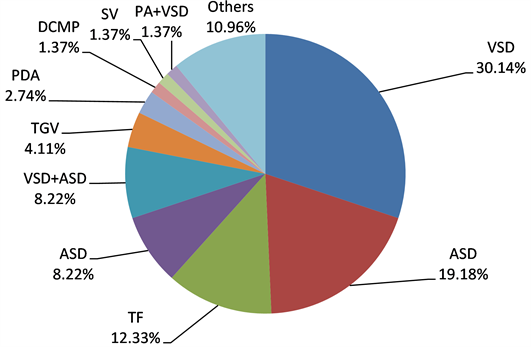
Diagram 2. Distribution of CHD types for 73 diseases found in the pediatric department in the UH GT. VSD: ventricular septal defect, ASD: atrial septal defect, TF: Tetralogy of Fallot, AVSD: atrio-ventricular septal defect, TGV: Transposition of great vessels, PDA: Persistent ductus arteriosus, DCMP: dilated cardiomyopathy, SV: single ventricle, PA + VSD: pulmonary atresia + VSD.
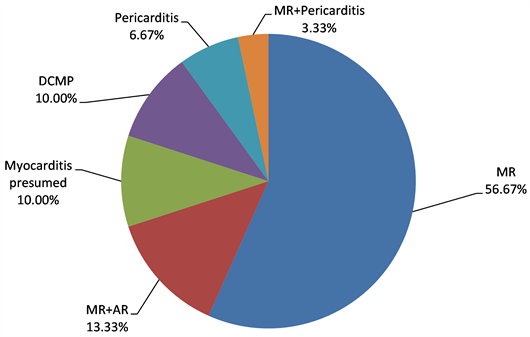
Diagram 3. Distribution of AHD types for 30 cases in the pediatric department of the UH GT. MR: mitral regurgitation, AR: aortic regurgitation, DCMP: dilated Cardiomyopathy.
![]()
Table 1. Distribution of socio-demographics and history of 103 hospitalized patients in the pediatric department of UH GT.
NA* No answer ** Hypertension (4), Diabetes (1), alcohol consumption (2).
![]()
![]()
Table 2. Clinical characteristics of 103 patients with heart diseases in pediatric department of the UH GT.
![]()
Table 3. Distribution of heart disease type related to age group.
3.4. Outcome
Mortality was higher among CHD with 31% versus 11% of RHD patients during the hospitalization period (p = 0.037) (Table 4).
4. Discussion
Our study shows a significant prevalence of 1.2% in pediatric heart disease in the pediatric department of UH GT. Ellena M. et al. [14] found 1.7% of cases whereas Ba et al. [15] reported a very low prevalence 4.3/1000.
The 0 to 4 age group was the most affected (73.80%) with a mean age of 4.11 years. Diarra B. [16] had recorded 57.33% of patients aged between 10 and 15 years. This difference could be explained by the high prevalence of rheumatic heart disease in his study.
In our study, 103 cases of heart disease were identified by echocardiography, and CHD was much more common (70.87%) than AHD (29.13%). The same results were reported by several African publications [14] [16] [17] [18] . The vast majority of CHD cases (98.6%) were diagnosed before the age of 5. Tougouma SJB [9] , Kinda G [19] in Ouagadougou, Cloarec [20] in France, and Abena [21] recorded lower rates with respectively 53%, 03%, 55%, 61% and 70%. The delay in the discovery and management of cardiac diseases in general and CHD in particularly could be partly explained by the absence of systematic screening at birth, difficulties in accessing echocardiographic examination and also to the
![]()
Table 4. Outcome of 96 patients with heart diseases in the study period in the pediatric department.
p = 0.037, Nota Bene: 5 cases of CHD and 2 of AHD were considered lost.
presence of certain forms that are not very symptomatic and may go unnoticed on clinical examination.
About AHD, 86.66% were discovered after the fifth year of life, as found by other [22] [23] . This could be explained by the long latency period required for development of post-rheumatic complications.
The most current CHD in our study was isolated VSD with 30.13% as found several African authors [12] [24] [25] .
Isolated MR with 56.67% of cases was the most common AHD. This was the same finding in other African studies [15] [22] .
We recorded 31.90% of deaths among CHD patients and 11.10% among those with AHD. Ba et al. [15] recorded 24.4% overall lethality. In contrast, Bitwe MR et al. [24] had death rates higher than ours with 34.29%. Some of our unpublished data from Thesis for medical student, found 45.09% of deaths but in pediatric resuscitation unit. These deaths are most often due to a delay in diagnosis and/or the management of complications such as hypoxic spells, heart failure, broncho-pulmonary diseases. Moreover the lack of human resources, material and/or financial issues is contributing factors to the poor outcome of heart diseases specially in children age. These issues had been already underlined by Ba [11] and Diarra [26] .
There is some progress related to management of diseases such ductus closure, pulmonary blood supply through external conduit, but open-heart surgery is up to day not possible in Mali, contribution to the high mortality of pediatric heart diseases.
5. Conclusion
This study, although containing some limitations, shows that children heart diseases are frequent, CHD more represented than AHD. We had a similar pattern than in other countries but higher mortality rate. There is also urgent need to focus on the early detection of childhood heart disease and improve their access to cardiac surgery.
Limits of the Study
This was a retrospective study that has the disadvantage of not providing all the desired data. Otherwise, neonates with severe CHD who died shortly after birth, patients who did not receive Doppler ultrasound and those who could not access the hospital were not included.
We had only echocardiography as investigation tool for confirmation. Other diagnostic tool, namely the cardiac catheter and magnetic resonance imaging that could have provided an accurate diagnosis or limited false negatives, are not available.