Double Cystic Duct Not Detected by Imaging But Diagnosed on Intraoperative Dissection in Laparoscopic Cholecystectomy: A Case Report, Hatwan Hospital-Sulaimani Province-Kurdistan-Iraq (Case Report)
1. Introduction
Laparoscopic cholecystectomy is now a gold standard treatment modality for symptomatic gallstone diseases. However, the incidence rate of bile duct injury has not been changed for many years [1] . This may be because of biliary tree abnormalities, as variation in cystic duct anatomy is quite common, which may be detected by preoperative ultrasonography, magnetic resonant cholangiopancreatography [2] [3] .
However, a double cystic duct is extremely rare; only 9 cases have been reported in the literature with preoperative suspension or diagnosis of double cystic duct that was confirmed intraoperatively [4] . But there is only one report of double cystic duct in the literature, by (Mittelstaedt CA) that was found in laparoscopic cholecystectomy without diagnosis in preoperative preparation [2] [5] .
2. Case Report
A 58-year-old lady (Table 1) with symptomatic gallstones prepared for laparoscopic cholecystectomy, in the history had features of cholangitis and previous attacks of biliary colic.
Preoperative ultrasonography and MRCP were done to exclude CBD stones. Ultrasonography and MRCP showed normal gall bladder wall thickness and normal CBD and multiple small gallstones. Presence of double cystic ducts were confirmed by intraoperative suspension, meticulous dissection, and exploration of the cystohepatic (Calot’s) triangle , detailed in Table 2.
Formal four-port laparoscopy was started. After the initial dissection, the cystic duct was clipped and divided. Further dissection of the infundibulum revealed a tubular structure extending from the neck of the gallbladder to the common hepatic duct that was one centimeter above the insertion of cystic duct. It was not pulsating to be the Caterpillar hump of right hepatic artery.
Further dissection of the distal part of this tubular structure was connected to the infundibulum of the gallbladder. The tubular structure did not run over the surface of the gallbladder instead it ended in the infundibulum. After the exploration of the proximal side of the tubular structure, it ended like an ordinary cystic duct in the common duct one centimeter above the joining point of the cystic duct to the common duct as shown in Picture 1. The tubular structure
![]()
Table 1. Showing demographic data of the patient.
![]()
Table 2. Showing preoperative finding in imaging of the patient.
was then clipped and divided. The artery was then visible which was clipped and transected. The gallbladder was then removed.
Hand drawing of the gall bladder and double cystic ducts shown in Diagram 1.
Macroscopic examination of the extracted gall bladder revealed double cystic ducts and this was confirmed by probing of their lumens.
The patient had an uneventful early postoperative period, and was discharged on the first postoperative day in good general condition.
The patient’s first visit was after 7 days and on further follow-up, there were no features of complications with liver function tests being normal. The patient followed till now, she is in her 12th post-operative month having no features of complications with normal liver function tests and ultrasonography checkup.
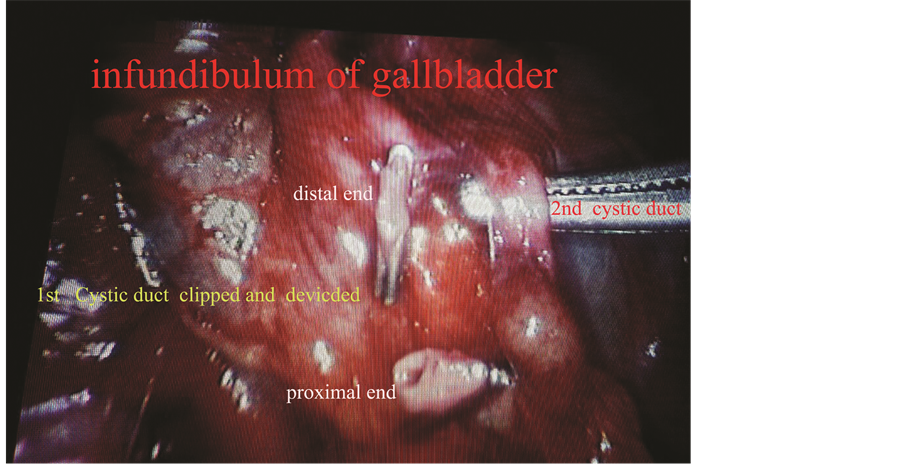
Picture 1. Detail of the exploration of first and second cystic duct.

Diagram 1. Showing position of the cystic ducts.
3. Discussion
Although imagings are of little help in diagnosis of double cystic duct, endoscopic retrograde cholangiopancreatography may suspect and be confirmed by intraoperative cholangiography [6] [7] .
The small caliber of the cystic duct and its tortuosity make detection difficult with axial CT and US and cholescintigraphy is further limited by low resolution. Optimal visualization of the cystic duct requires direct cholangiography or MR cholangiopancreatography, both of which depict the cystic duct in the coronal plane along its long axis [3] [6] [8] .
Color Doppler US may be used to distinguish bile ducts from the vessels [9] . Double cystic duct is extremely rare and poses a challenge for surgeons during an operation. Diagnosis of this condition is usually confirmed during laparoscopic cholecystectomy. This is the second report of double cystic duct found in laparoscopic cholecystectomy without even suspicion in preoperative preparation, the first case reported by Mittelstaedt CA [2] .
In practice of laparoscopic cholecystectomy, this abnormality which is extremely rare may be present without any suspension before surgery. The anticipation of the probable existence of such bile duct variation serves as the most important factor in preventing iatrogenic bile duct injuries [10] . Awareness among the surgeons regarding this anatomic anomaly could help in avoiding converted laparotomy and reduce the risk of complications.
4. Conclusion
In practice of laparoscopic cholecystectomy, this abnormality may be present without any suspension before surgery. Awareness of probable existence of double cystic duct may save us, in injury to bile tree and unnecessary conversion to open cholecystectomy.