1. Introduction
The leukemoid reaction (LR) is a potential marker for malignant behaviour and poor prognosis in advanced tumours. This is kind of paraneoplastic syndrome. Most paraneoplastic syndromes appear only during the late stages of malignancy when the diagnosis has long been established, but sometimes may be an early sign of the malignancy. However, it’s rarely found in cases of breast cancer. Herein, we reported a case of advanced breast cancer related LR and the LR disappeared after disease controlled.
2. Case Report
A 38-year-old woman, presented with progressive lump in right breast. Physical examination showed a palpable huge mass in the right breast (Figure 1). Laboratory test results showed leukocytosis (79.9 × 103/uL) with a neutrophil predominant differential cell counts. Core biopsy of breast tumor was done and the pathology showed infiltrating ductal carcinoma. Chest X-ray, abdominal ultrasonography and whole body bone scan showed no evident of metastasis. She received four courses of chemotherapy (Paclitaxel and Adriamycine). She underwent modified radical mastectomy (MRM) after the fourth course of chemotherapy because of recurrent leukocytosis developed. After completion of MRM, the condition of leukocytosis subsided. Two months later, tumor local relapse was found and white blood cells (WBC) rose again. After completion of wide excision, the condition of leukocytosis subsided again. Figure 2 demonstrated the series of WBC change during the treatment course. She was well and no leukocytosis and tumor relapse at one month later.
3. Discussion
The WBC count more than 50 × 109/l associated with a cause outside the bone marrow is termed as leukemoid reaction (LR) [1]. The major causes of LR include severe infection, intoxications, malignancies, severe hemorrhage, or acute hemolysis [2]. Malignancy-associated LR are observed in several carcinomas, most commonly in lung [2,3]. Kasuga I. et al. reported 227 patients with carcinoma of the lung, 14.5% were associated with tumor-related leukocytosis and 2.6% with LR [4]. However, breast cancer associated with LR was rarely reported. But, there are several animal models [5,6]. The mechanism may be due to secretion of granulocyte colony-stimulating factor (GCSF) by the tumor cells. Its target cells are late myeloid progenitors enhancing production and function. LR is diagnosed by the exclusion of a malignant hematological disorder, chronic myelogenous leukemia and chronic neutrophilic leukemia.
Our patient was a case of huge breast cancer (T4 lesion) and leukocytosis was found. Every time she underwent chemotherapy, the WBC counts dropped. Nimieri HS et al. reported the good response of a LR to chemotherapy

Figure 1. Physical examination showing huge mass in the right breast.
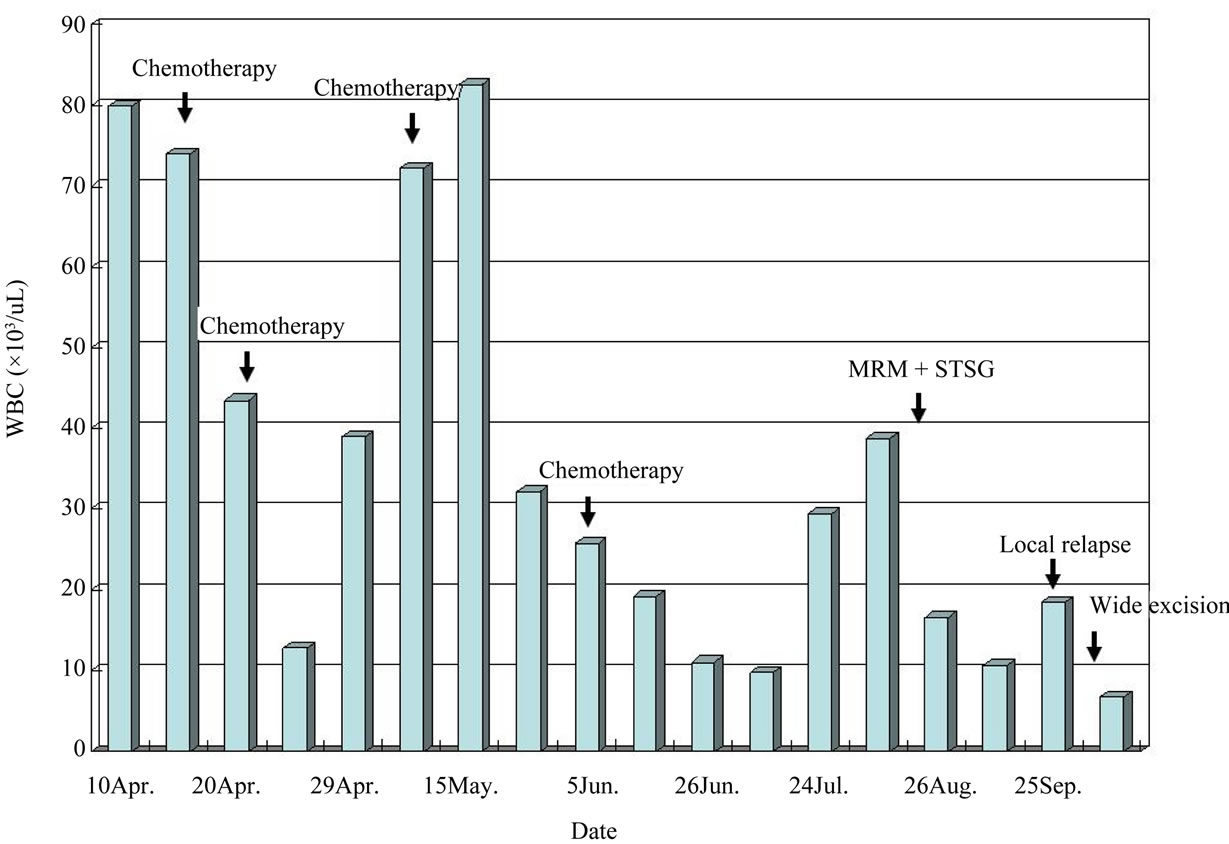
Figure 2. Clinical course of leukemoid reaction. (WBC: white blood cells, MRM: modified radical mastectomy).
and local radiotherapy in a patient diagnosed with cervical cancer [1]. Our patient also got good response of LR to chemotherapy. But the LR recurred. We decided to control the primary lesion and we were surprised with such good response of LR after MRM. The LR came back while tumor relapse two months later and was decline after complete resection.
This case supports the theory that the tumor cells produce the G-CSF, then result in marked leukocytosis. The LR will be disappeared after well control of tumor cells or primary lesion. Leukocytosis may be as a hint of tumor relapse.
NOTES