Antimicrobial Assay of Chlorhexidine-Wetted Textile Napkins for Surgical Site Disinfection in Ocular Surgery
580
cavity. Thus, for a certain period of time, the oral cavity
becomes a CHG reservoir, which prolongs its chemical
activity in preparations [22]. The ocular surface (cornea
and conjunctiva) is also negatively charged [23,24], and
the paracellular space is more permeable to cations than
to anions at physiological pH [25,26] consistently the
ocular surface may also become a CHG reservoir, which
prolongs its chemical activity in preparations. This phe-
nomenon depathogenizes the ocular surface flora intra-
operatively and postoperatively but bacteriological cul-
ture from the ocular surface may continue to be positive.
Results showed that the use of BSS during cataract
surgery did not totally decrease th e antimicrobial activity
of the textile napkins due to CHG absorbed in the fibers
of certain textile, pa rticularly cotton, and consistently re-
sisted removal by washing [5]. Thereby, the textile nap-
kin virtually serves as a sustained release reservoir of
CHG during phacoemulsification. Moreover, equal di-
ameter of the growth inhibition zones before and after
phacoemulsification cataract extraction also indicates
that 0.5% levofloxacin ophthalmic solution instilled pre-
operatively is not an antagonist of 0.02% CHG. Addi-
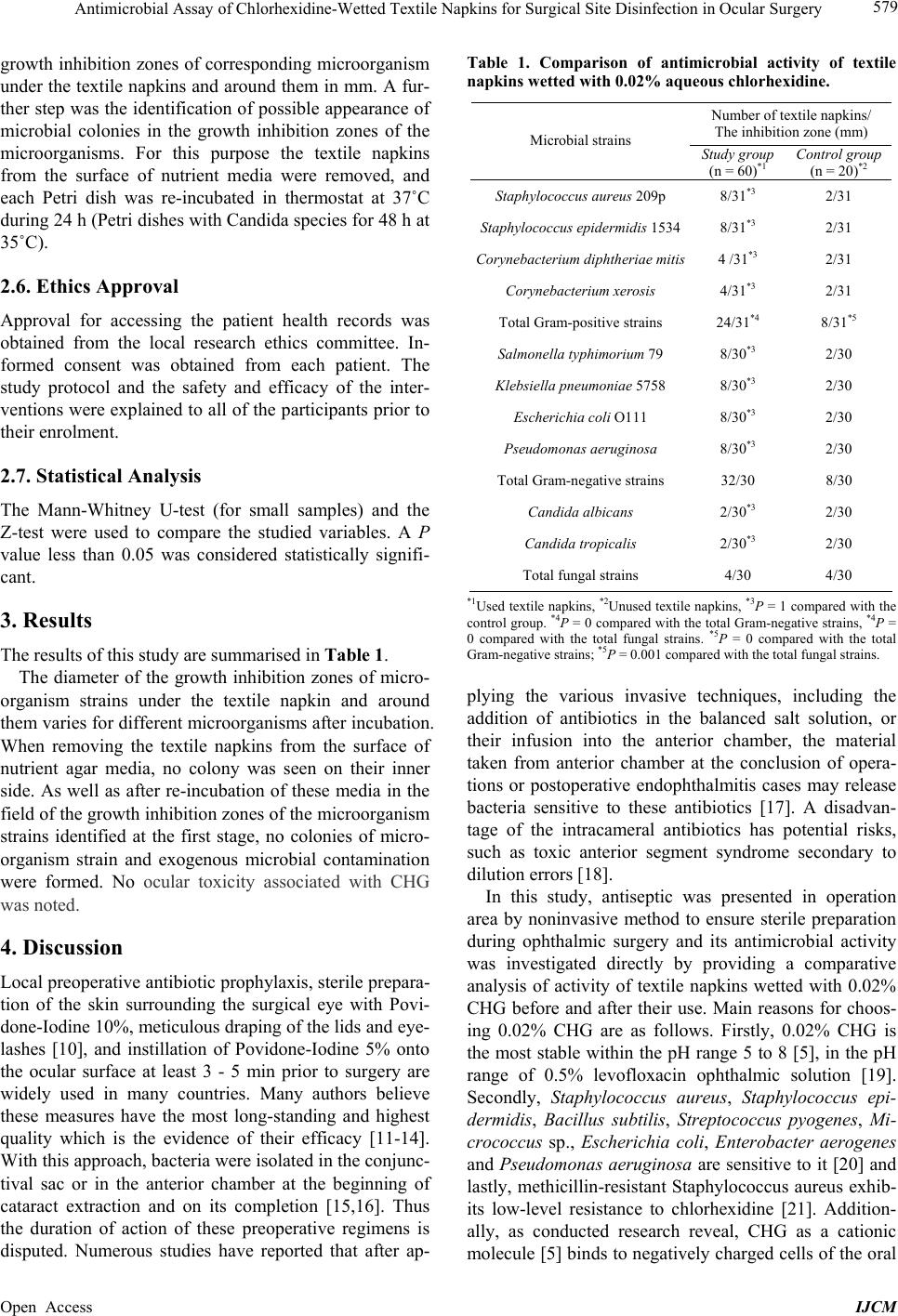
tionally, antimicrobial activity of both unused textile nap-
kins and used textile napkins, wetted with 0.02% CHG
against gram-positive bacteria is more than gram-nega-
tive (Table 1), that is comparable to certain reports [5,
20]. Since microbial flora under the textile napkins
mixed with flora of the conjunctival sac and the lid mar-
gin, the result of microbial culture from the conjunctival
sac after withdrawing the textile napkins on completion
of the surgery is disputed. Test strains colonies were not
seen after incubation of Petri dishes on the surface and
inner side of used textile napkins. Likewise in th e growth
inhibition zones after re-incubation, exogenous microor-
ganism colonies that could contaminate used textile nap-
kins during surgery were not seen.
5. Conclusion
The antimicrobial activity assay of CHG-wetted textile
napkins indicates a persistent antimicrobial effect of a
residue of CHG in the textile napkins during phacoe-
mulsification cataract extraction. Intraoperatively, the
isolation of the lid edg es with 0.02% CHG-wetted textile
napkins in combination with a preoperative antibacterial
prophylaxis for instance 0.5% levofloxacin ophthalmic
solution reliably prevents microbial surface contamina-
tion during ophthalmic surgery.
6. Acknowledgements
The author appreciates Ms. Sepideh Elahi of INOVA
Fairfax Hospital, VA, USA for assistance with statistical
analysis. This paper was derived from the author’s doc-
toral dissertation.
REFERENCES
[1] G. A. Peyman, J. T. Paque and H. I. Meisels, “Post-
operative Endophthalmitis: A Comparison of Methods for
Treatment and Prophylaxis with Gentamicin,” Ophthal-
mic Surgery, Vol. 6, No. 1, 1975, pp. 45-55.
[2] A. Pathengay, M. Khera, T. Das, S. Sharma, D. Miller
and H. W. Flynn Jr., “Acute Postoperative Endophthal-
mitis Following Cataract Surgery: A Review,” Asia-Pa-
cific Journal of Ophthalmology, Vol. 1, No. 1, 2012, pp.
35-42. http://dx.doi.org/10.1097/APO.0b013e31823e574b
[3] C. B. Walker and C. M. Claoue, “Incidence of Conjunc-
tival Colonisation by Bacteria Capable of Causing Post-
Operative Endophthalmitis,” Journal of the Royal Society
of Medici ne, Vol. 79, No. 9, 1986, pp. 520-521.
[4] M. G. Speaker, F. A. Milch, M. K. Shah, W. Eisner and B.
N. Kreiswirth, “Role of External Bacterial Flora in the
Pathogenesis of Acute Postoperative Endophthalmitis,”
Ophthalmology, Vol. 98, No. 5, 1991, pp. 639-649.
http://dx.doi.org/10.1016/S0161-6420(91)32239-5
[5] G. W. Denton, “Chlorhexidine,” In: S. S. Block, Ed.,
Disinfection, Sterilization, and Preservation, 5th Edition.
Lippincot Williams & Wilkins, Philadelphia, 2001, pp.
321-336.
[6] N. M. Sergienko, Y. N. Kondratenko, N. V. Chumak and
A. Daneshmand, “Results of Prophylaxis of Bacterial
Endophthalmitis in Cataract Surgery,” Proceedings of
The Joint Congress of SOE/AAO, Geneva, June 2011, p.
51.
[7] K. Green, V. Livingston, K. Browman and D. S. Hull,
“Chlorhexidine Effects on Corneal Epithelium and Endo-
thelium,” Archives of Ophthalmology, Vol. 98, No. 7,
1980, pp. 1273-1278.
http://dx.doi.org/10.1001/archopht.1980.01020040125020
[8] N. L. Burstein, “Preservative Cytotoxic Threshold for
Benzalkonium Chloride and Chlorhexidine Digluconate
in Cat and Rabit Corneas,” Journal Investigative Oph-
thalmology & Visual Science, Vol. 19, No. 3, 1980, pp.
308-313.
[9] A. W. Bauer, W. M. Kirby, J. C. Sherris and M. Turck,
“Antibiotic Susceptibility Testing by Standardized Single
Disc Method,” American Journal of Clinical Pathology,
Vol. 45, No. 4, 1966, pp. 493-496.
[10] L. D. Perry and C. Skaggs, “Preoperative Topical Anti-
biotics and Lash Trimming in Cataract Surgery,” Oph-
thalmic Surgery, Vol. 8, No. 5, 1977, pp. 44-48.
[11] S. J. Isenberg, L. Apt, R. Yoshimori, C. Pham and N. K.
Lam, “Efficacy of Topical Povidone-Iodine during the
First Week after Ophthalmic Surgery,” American Journal
of Ophhalmology, Vol. 124, No. 1, 1997, pp. 31-35.
[12] T. J. Liesegang, “Use of Antimicrobials to Prevent Post-
operative Infection in Patients with Cataracts,” Current
Opinion in Ophthalmology, Vol. 12, No. 1, 2001, pp. 68-
74.
http://dx.doi.org/10.1097/00055735-200102000-00012
[13] T. A. Ciulla, M. B. Starr and S. Masket, “Bacterial Endo-
phthalmitis Prophylaxis for Cataract Surgery: An Evi-
dence-Based Update,” Ophthalmology, Vol. 109, No. 1,
2002, pp. 13-24.
Open Access IJCM