 Vol.5, No.10, 1541-1547 (2013) Health http://dx.doi.org/10.4236/health.2013.510209 Preventable infant mortality: Spatial distribution and main causes in three Brazilian municipalities Rosana Rosseto de Oliveira1, Thais Aidar de Freitas Mathias2 1Graduate Nursing Program, State University of Maringá, Maringá, Brazil; rosanarosseto@gmail.com 2Nursing Department, Graduate Nursing Program, State University of Maringá, Maringá, Brazil; tafmathias@uem.br Received 29 May 2013; revised 28 June 2013; accepted 15 July 2013 Copyright © 2013 Rosana Rosseto de Oliveira, Thais Aidar de Freitas Mathias. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Objective: The objective was to identify spatial distribution patterns for preventable infant mor- tality and the main causes of death in three mu- nicipalities of Paraná state, Brazil. Design and Sample: Ecological study on infant mortality among residents of the municipalities of Mar- ingá, Sarandi and Paiçandu, between 2004 and 2008. Measures: Data were obtained from re- ports by the Infant Mortality Prevention Com- mittee, georeferenced in 19 Demographic Ex- pansion Areas and analyzed statistically using Local Moran’s Index. Results: Of the 284 deaths among children under one year of age, 68.7% were considered preventable, and higher per- cent ag es were found in outlying area s. The main causes were illnesses originated during the perinatal period (73.8%), exter nal c auses (11.3%) and diseases of the respiratory system (5.1%). Conclusion: It is necessary to implement ac- tions and policies on child and prenatal assis- t ance, in order to redu ce the inequality observed between the central and outlying areas of the region under study. Keywords: Infant Health; Mortality; Public Health; Population-Based Nursing 1. INTRODUCTION Infant mortality is an indicator of quality of life and health, reflects socioeconomic conditions and is also a parameter to evaluate the organization and quality of health services and obstetric and neonatal assistance [1]. Knowing the context in which child deaths occur is es- sential to evaluating local actions with regard to wo- men’s and children’s health, as well as to promoting measures against potentially preventable infant morbi- mortality [2]. Preventable causes of child mortality are defined as events, fully or partially preventable by effective actions from health services accessible at a given place and time. Thus, by using the full set of technology resources and updated health knowledge, these events should not occur. The causes of preventable death are sensitive to health care, but they also respond significantly to improve liv- ing conditions, access to goods and services, schooling and income [3]. The precursor of the debate on the term preventability was David Rutstein, who defined it as a sentinel event— something that should not occur, whether preventable illness, unexpected disability or death; its occurrence serves as a warning sign that the quality of therapy or promotion/prevention measures must be better analyzed [4]. A study performed in Brazil and other regions from 1997 to 2006 indicated a 37% reduction in the rate of infant mortality from preventable causes [3], demon- strating the positive impact of health services in improv- ing living conditions for the population. Nevertheless, infant mortality still reaches high rates—in 2011 it stood at 21.17 deaths per thousand live births, most of which were potentially preven table [5]. In the state of Paraná, a study using results of analyses on child deaths investi- gated by the Infant Mortality Prevention Committees (IMPC) showed that 55% of deaths could have been avoided through adequate care during gestation, delivery and the neonatal period [6]. Despite its decline, infant mortality remains a health priority in developing countries given extensive regional inequalities, between and within cities, which justifies the analysis of infant mortality and its pr eventab ility on a regional approach. To that end, geoprocessing techniques utilize space as an analytical category and use thematic maps to describe different health phenomena—from the Copyright © 2013 SciRes. OPEN ACCESS 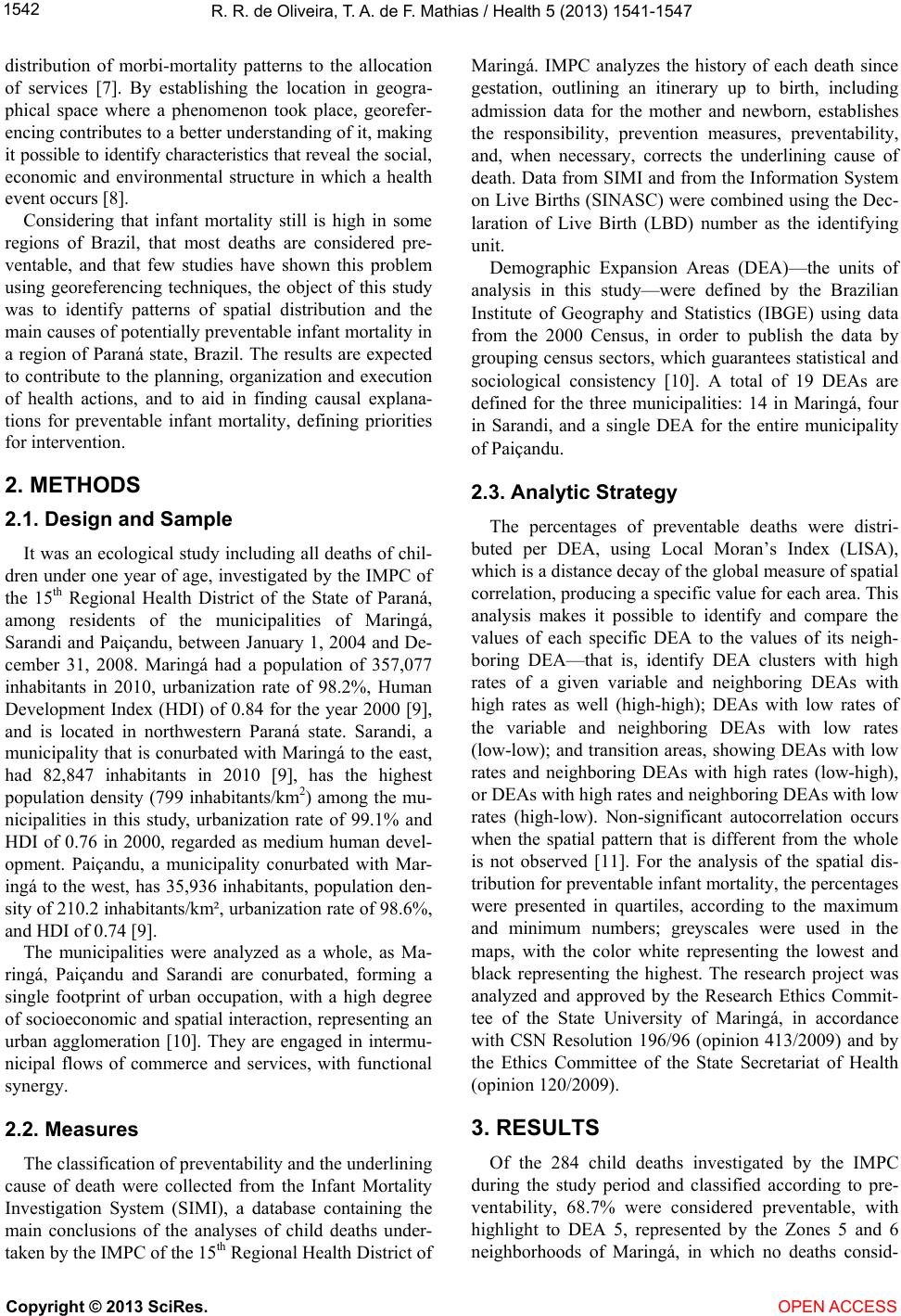 R. R. de Oliveira, T. A. de F. Mathias / Health 5 (2013) 1541-1547 1542 distribution of morbi-mortality patterns to the allocation of services [7]. By establishing the location in geogra- phical space where a phenomenon took place, georefer- encing contributes to a better understanding of it, making it possible to identif y characteristic s that rev ea l th e so ci al , economic and environmental structure in which a health event occurs [8]. Considering that infant mortality still is high in some regions of Brazil, that most deaths are considered pre- ventable, and that few studies have shown this problem using georeferencing techniques, the object of this study was to identify patterns of spatial distribution and the main causes of potentially p reventab le infant mortality in a region of Paraná state, Brazil. The results are expected to contribute to the planning, organization and execution of health actions, and to aid in finding causal explana- tions for preventable infant mortality, defining priorities for intervention. 2. METHODS 2.1. Design and Sample It was an ecological study including all deaths of chil- dren under one year of age, investigated by the IMPC of the 15th Regional Health District of the State of Paraná, among residents of the municipalities of Maringá, Sarandi and Paiçandu, between January 1, 2004 and De- cember 31, 2008. Maringá had a population of 357,077 inhabitants in 2010, urbanization rate of 98.2%, Human Development Index (HDI) of 0.84 for the year 2000 [9], and is located in northwestern Paraná state. Sarandi, a municipality that is conurbated with Maringá to the east, had 82,847 inhabitants in 2010 [9], has the highest population density (799 inhabitants/km2) among the mu- nicipalities in this study, urbanization rate of 99.1% and HDI of 0.76 in 2000, regarded as medium human devel- opment. Paiçandu, a municipality conurbated with Mar- ingá to the west, has 35,936 inhabitants, population den- sity of 210.2 inhabitants/km², urbanization rate of 98.6%, and HDI of 0.74 [9]. The municipalities were analyzed as a whole, as Ma- ringá, Paiçandu and Sarandi are conurbated, forming a single footprint of urban occupation, with a high degree of socioeconomic and spatial in teraction, representing an urban agglomeration [10]. They are engaged in intermu- nicipal flows of commerce and services, with functional synergy. 2.2. Measures The classification of prev entab ility an d th e un derlining cause of death were collected from the Infant Mortality Investigation System (SIMI), a database containing the main conclusions of the analyses of child deaths under- taken by the IMPC of the 15th Regional Health District of Maringá. IMPC analyzes the history of each death since gestation, outlining an itinerary up to birth, including admission data for the mother and newborn, establishes the responsibility, prevention measures, preventability, and, when necessary, corrects the underlining cause of death. Data from SIMI and from the Information System on Live Births (SINASC) were combined using the Dec- laration of Live Birth (LBD) number as the identifying unit. Demographic Expansion Areas (DEA)—the units of analysis in this study—were defined by the Brazilian Institute of Geography and Statistics (IBGE) using data from the 2000 Census, in order to publish the data by grouping census sectors, which guarantees statistical and sociological consistency [10]. A total of 19 DEAs are defined for the three municipalities: 14 in Maringá, four in Sarandi, and a single DEA for the entire municipality of Paiçandu. 2.3. Analytic Strategy The percentages of preventable deaths were distri- buted per DEA, using Local Moran’s Index (LISA), which is a distance decay of the global measure of spatial correlation, producing a specific value for each area. This analysis makes it possible to identify and compare the values of each specific DEA to the values of its neigh- boring DEA—that is, identify DEA clusters with high rates of a given variable and neighboring DEAs with high rates as well (high-high); DEAs with low rates of the variable and neighboring DEAs with low rates (low-low); and transition areas, showing DEAs with low rates and neighboring DEAs with high rates (low-high), or DEAs with high rates and neighboring DEAs with low rates (high-low). Non-significant autocorrelation occurs when the spatial pattern that is different from the whole is not observed [11]. For the analysis of the spatial dis- tribution for preventable in fant mortality, the p ercentag es were presented in quartiles, according to the maximum and minimum numbers; greyscales were used in the maps, with the color white representing the lowest and black representing the highest. The research project was analyzed and approved by the Research Ethics Commit- tee of the State University of Maringá, in accordance with CSN Resolution 196/96 (opinion 413/2009) and by the Ethics Committee of the State Secretariat of Health (opinion 120/2009). 3. RESULTS Of the 284 child deaths investigated by the IMPC during the study period and classified according to pre- ventability, 68.7% were considered preventable, with highlight to DEA 5, represented by the Zones 5 and 6 neighborhoods of Maringá, in which no deaths consid- Copyright © 2013 SciRes. OPEN ACCESS  R. R. de Oliveira, T. A. de F. Mathias / Health 5 (2013) 1541-1547 Copyright © 2013 SciRes. OPEN ACCESS 1543 ered preventable took place (Table 1). Of the 195 deaths classified as preventable, 144 (73.8%) showed diseases originated in the perinatal pe- riod as the underlining cause of death, after investigation. As the second main underlining causes of death as ana- lyzed by the IMPC were external causes, with 22 cases (11.3%); in third place were diseases of the respiratory system, with 5.1% of deaths (Table 2). The spatial distribution of the percentages of preven- table deaths shows that, with the exception of the central region of Maringá (DEA 5) and a few surro un di n g nei gh- borhoods (DEA 4, 1, 2, 3, 6, 7, 8, 12 in Maringá and DEA 17 in Sarandi), most of the maps shows high rates of preventable deaths—between 63.6% and 84.6% (Fig- ure 1). Local Moran’s Index showed a concentration of areas with “high-high” correlation at DEA 18 in Sarandi, which features 70% of preventable child deaths; “low-low” correlation at DEAs 6 and 7, located in cen- tral areas of Maringá, with percentages of preventable child deaths of 54.5% an d 50%, respectively; “high-low” correlation at DEA 10 (area with 65.4% preventable child deaths); “low-high” correlation at DEA 17 in Sarandi (55.6% preventabl e deaths) (Figure 2). 4. DISCUSSION The results of this research show that most child deaths that occurred in the municipalities under study (68.7%) were considered preventable; this means it is essential to seek improvements in prenatal, delivery and newborn assistance, ensuring access by mother and newborn to quality services in a timely manner. The re- sults agree with the findings of a study of municipalities within the 15th Regional Health District of the State of Paraná, between 2000 and 2006, in which 70.1% of ana- lyzed deaths were considered preventable [2]. In that regard, health and nursing teams must develop actions that meet the challenges created by the conditions of morbi-mortality from preventable causes. The three municipalities in this study, alth oug h located in the interior of Paraná state, are part of a Metropolitan Area officially recognized by state law 83/98, currently consisting of 13 municipalities [10]. Social indicators and the reality of healthcare in the municipalities under study are quite similar to conditions found in the ou tlying areas of large urban centers, where less favorable socio- economic conditions are found, such as low income and schooling. This can be confirmed by observing that the Table 1. Infant mortality by DEA preventability potential. Maringá, Sarandi and Paiçandu, 2004 to 2008. Preventable Non-preventable DEA Neighborhood N % n % Total 1 Maringá Vila Morangueira 4 57.1 3 42.9 7 2 Maringá Jd. Alvorada 9 60.0 6 40.0 15 3 Maringá Zon a 7 3 60.0 2 40.0 5 4 Maringá Zona 8-Vila St.Antonio 2 33.3 4 66.7 6 5 Maringá Zona 5 and 6 - - 5 100.0 5 6 Maringá Zon a 1, 2 , 3, 4 6 54.5 5 45.5 1 1 7 Maringá A v. Mandacaru 3 50.0 3 50.0 6 8 Maringá Contorno Norte 8 61.5 5 31.3 13 9 M aringá Conjunto Requião 16 84.2 3 15. 8 19 10 Maringá Cidade Alta 17 68.0 8 32.0 25 11 Maringá Liberdade-Aeroporto 16 76.2 5 23. 8 21 12 Maringá Jd. Imperial-Pq Grv. 12 63.2 7 36.8 19 13 Maringá Zona Industrial 6 75.0 2 25.0 8 14 Maringá Olímpico 19 76.0 6 24.0 25 15 Paiçandu 19 73.1 7 26.9 26 16 Sarandi Centro 14 77. 8 4 22.2 18 17 Sarandi Jd. Independência 5 55.6 4 44.4 9 18 S a randi Parque Alvamar 14 70.0 6 30.0 20 19 Sa randi Linha do Trem 22 84.6 4 15.4 26 Total 195 68.7 89 31.3 284 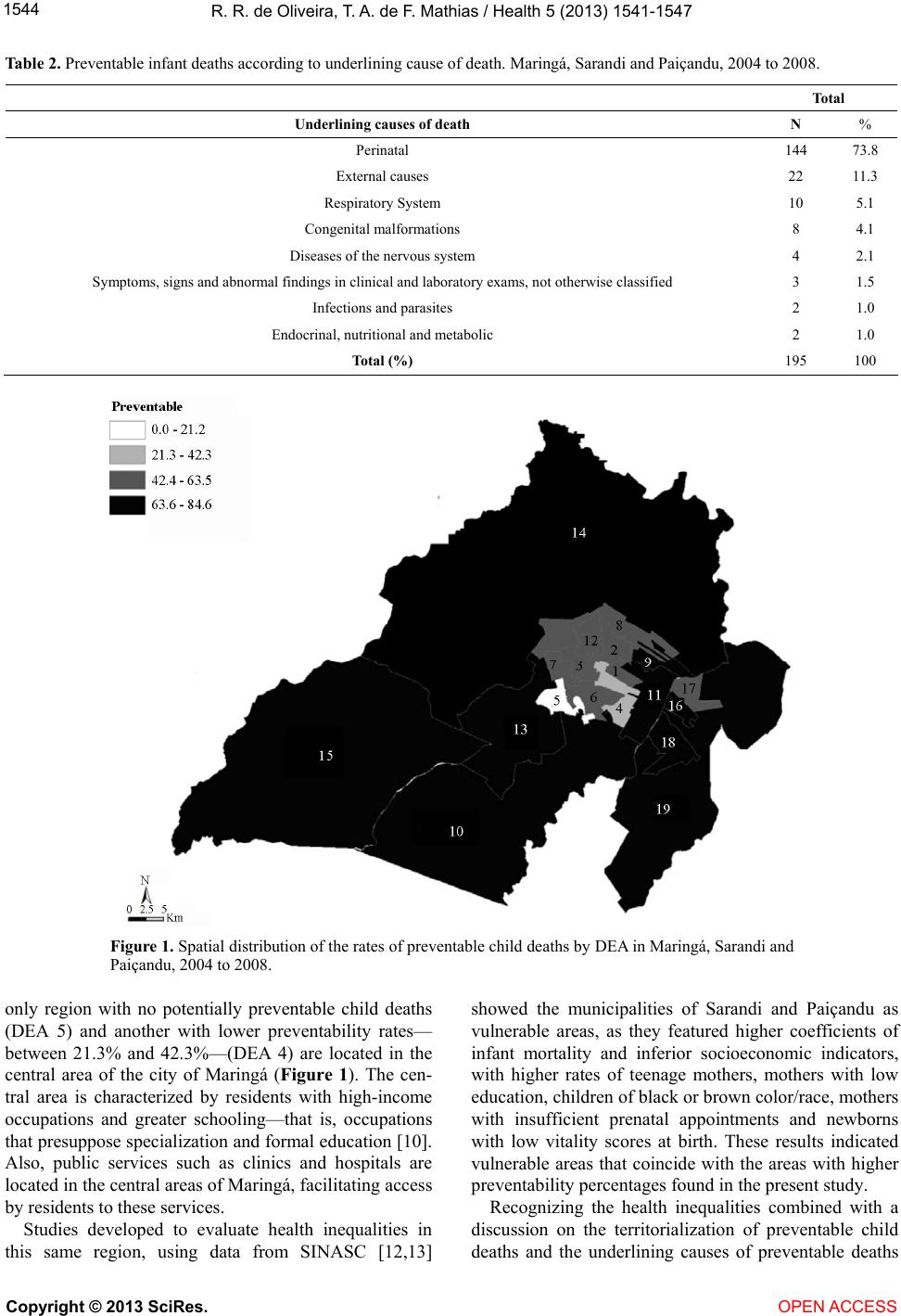 R. R. de Oliveira, T. A. de F. Mathias / Health 5 (2013) 1541-1547 1544 Table 2. Preventable infant deaths according to underlining cause of death. Maringá, Sarandi and Paiçandu, 2004 to 2008. Total Underlining causes of death N % Perinatal 144 73.8 External causes 22 11.3 Respiratory System 10 5.1 Congenital malformations 8 4.1 Diseases of the nervous system 4 2.1 Symptoms, signs and abnormal findings in clinical and laboratory exams, not otherwise classified 3 1.5 Infections and parasite s 2 1.0 Endocrinal, nutritional and metabolic 2 1.0 Total (%) 195 100 Figure 1. Spatial distribution of the rates of preventable child deaths by DEA in Maringá, Sarandi and Paiçandu, 2004 to 2008. only region with no potentially preventable child deaths (DEA 5) and another with lower preventability rates— between 21.3% and 42.3%—(DEA 4) are located in the central area of the city of Maringá (Figure 1). The cen- tral area is characterized by residents with high-income occupations and greater schooling—that is, occupations that presuppose specialization and formal education [10]. Also, public services such as clinics and hospitals are located in the central areas of Maringá, facilitating access by residents to these services. Studies developed to evaluate health inequalities in this same region, using data from SINASC [12,13] showed the municipalities of Sarandi and Paiçandu as vulnerable areas, as they featured higher coefficients of infant mortality and inferior socioeconomic indicators, with higher rates of teenage mothers, mothers with low education, children of black or brown color/race, mothers with insufficient prenatal appointments and newborns with low vitality scores at birth. These results indicated vulnerable areas that coincide with the areas with higher preventability percentages found in the present study. Recognizing the health inequalities combined with a discussion on the territorialization of preventable child deaths and the underlining causes of preventable deaths Copyright © 2013 SciRes. OPEN ACCESS  R. R. de Oliveira, T. A. de F. Mathias / Health 5 (2013) 1541-1547 1545 Figure 2. Spatial distribution of the percentages of preventable child deaths by Local Moran’s Index (LISA) and DEA in Maringá, Sarandi and Paiçandu, 2004 to 2008. in the municipalities of this study can contribute to an understanding of infant mortality, limits an d possibilities of health actions [14], and can provide health profession- als with awareness of the existing inequality among the different regions of the municipalities. Although the studied municipalities have lower infant mortality coefficients when compared to other munici- palities in different regions of Brazil (9.5, 14.3 and 11.3 deaths per thousand live births in Maringá, Sarandi and Paiçandu, respectively, between 2004 and 2008), ade- quate prenatal measures and care measures during deliv- ery and neonatal stages, such as improving service and organization and arranging services in networks, would represent 195 child deaths that could be prevented during the study period, as these deaths were classified as pre- ventable according to an analysis by the IMPC. With regard to the underlining causes, there were a high percentage of deaths resulting from conditions originating during the perinatal period, from diseases of the respiratory system and from external causes, which combined for 90.2% of deaths. Thes e re sults reve aled the potential preven tability of these deaths, as perinatal cau s- es represent fully or partially “preventable deaths” if adequate care measures were implemented for the mo- ther during gestation and delivery, and to the newborn [15]. It is known that childhood is a particularly vulnerable life stage, in which biological determinants of morbi- mortality are strongly linked to external conditions— either socioeconomic or environmental (housing, diet, sanitation, hygiene and family relations)—or to the availability of health services [16]. We must also con- sider the influence of public health measures; even if low-cost or easily implementable, these measures are responsible for a considerable reduction in infant mortal- ity [17]. Therefore, partnerships with other sectors of society—such as the Children’s Ministry, for instance— demonstrate that integration must be considered between all social levels and public/private partnerships in order to solve problems that transcend the field of clinical practice, as in the case of social inequalities [18]. In the present work, the analysis of preventable child deaths showed areas with “high-high” correlation at DEA 18, in the Sarandi region, meaning that it is an area with a high rate of preventable deaths surrounded by other re- gions with high percentages as well. “Low-low” correla- tions in the central areas of Maringá showed homoge- nous area in that region, with lower percentages of child death preventability. “High-low” correlations in the out- lying areas of Maringá showed an area that needs to be better evaluated, as it showed percentages that contrast with the results found in the neighboring DEAs of that municipality. The “low-high” correlation for the central area of Copyright © 2013 SciRes. OPEN ACCESS  R. R. de Oliveira, T. A. de F. Mathias / Health 5 (2013) 1541-1547 1546 Sarandi shows that even within that municipality, there is a pattern characterized by a nucleus-periphery distribu- tion, with better health indicators for residents of the city’s central areas. The results indicate that although all three municipalities show DEAs with high percentages of preventable infant mortality, Sarandi has the highest values. That observation can be partially explained by the spatial occupation of Sarandi, which has been char- acterized by people who wish to live in Maringá but move to neighboring municipalities in search of more affordable housing, yet maintain their employment, un- deremployment, studies, shopping and leisure in the other municipality [10]. Therefore, conditions acknowl- edged as risks to the mother and newborn—which can be prevented and intervened by the health sector—com- bined with unfavorable socioeconomic conditions such as low family income and low education—can charac- terize iniquity. Knowing these factors, the responsibility of managers, health professionals and services is directly linked to preventable child deaths [19,20]. The results of this study may show biases characteris- tic of research studies that use secondary databases, ei- ther in quantity or quality of data, as the information is subject to data accuracy and thoroughness, which do not invalidate their use. Information systems with the data routinely collected in health services constitute valuable sources of information, the results of which can contrib- ute to improved quality and coverage of this information when analyzed. However, we must emphasize the im- portance of participation and responsibility of munici- palities for producing, organizing and feeding the data- bases. It is necessary to eliminate errors in records in order to obtain reliable data, including address informa- tion—essential in studies that use georeferenced carto- graphic parameters [21,22]. In addition to collecting and forwarding the data, th e municipalities must monitor and evaluate the quality of the data in health information systems, by continuously training the agents responsible for that activity [21]. By using geoprocessing techniques, this analysis adds information on preventable infant mortality, given that the location of the event in geographic space was possi- ble using thematic maps. Using homogenous areas, such as DEAs, to monitor health events can contribute so that managers can evaluate each area differently. The results showed that for the municipalities under analysis, outly- ing DEAs feature the highest rates of preventable child deaths. This conclusion leads to the consideration that these populations are more susceptible to hardship in accessing medical technologies and adequate health ser- vices, which would be enough to prevent infant morbi- mortality. Another contribution of this study to the territorial- based analysis of the distribution of potentially prevent- able deaths and their underlying causes is the use of data generated from the death investigation analyses by the IMPCs working in the Regional Health Districts of the State of Paraná. The analysis of child death prevent- ability can assist in identifying the areas with the high est probability of success or failure in preventing these deaths, in addition to indicating the performance of the healthcare system and the population’s behavior when seeking healthcare. This methodology of study can be reproduced in other localities at different desired units of analysis. The present study used homogenous areas as standardized by IBGE according to the National Census, which guarantees the quality of the methodology. It is worth underlining that even though DEAs repre- sent smaller areas within a municipality, with more ho- mogenous characteristics, they can still hide different situations and realities to b e explored. It is important to highlight the limits of interpretation of the results of this study, in that the information is sub- ject to the thoroughness and accuracy of the data regard- ing the addresses of the mothers of each newborn. This may compromise the analysis and monitoring of pre- ventable infant mortality in the geographic realm. Other studies are still required in order to better know the population residing in the regions with the highest rates of preventability, evaluating the conditions of ac- cess to health services, quality of service, as well as ref- erence and counter-reference services in caring for wo- men during gestation and delivery and for newborns. Lastly, the debate on the responsibility for preventab le child death must be taken to health services and incorpo - rated in the work routine, as the occurrence of prevent- able child death may indicate the need for revision and suitability of health assistance to the population in their numerous health needs, beyond those related to mother and child. REFERENCES [1] Ministry of Health (BR) (2009) Departamento de ações programáticas estratégicas. Manual de vigilância do óbito infantil e fet al e do comitê de prevenção do óbito infantil e fetal. MS, Brasília. [2] Mathias, T.A.F., Assunção, A.M. and Silva, G.F. (2008) Infant deaths investigated by the Prevention Committee of Infant Mortality in region of Paraná state. Revista da Escola de Enfermagem, 42, 445-453. http://dx.doi.org/10.1590/S0080-62342008000300005 [3] Malta, D.C., Duarte, E.C., Escalante, J.J., Almeida, M.F., Sardinha, L.M.V., Macário, E.M., et al. (2010) Avoidable causes of infant mortality in Brazil, 1997-2006: Contribu- tions to performance evaluation of the Unified National Health System. Cadernos de Saúde Pública, 26, 481-491. http://dx.doi.org/10.1590/S0102-311X2010000300006 [4] Rutstein, D.D., Bereberg, W., Chalmers, T.C., Child, C.G., Copyright © 2013 SciRes. OPEN ACCESS  R. R. de Oliveira, T. A. de F. Mathias / Health 5 (201 3) 1541-1547 Copyright © 2013 SciRes. OPEN ACCESS 1547 Fishman, A.P., Perrin, E.B., et al. (1976) Measuring the quality of medical care: A clinical method. The New England Journal of Medicine, 294, 582-588. http://dx.doi.org/10.1056/NEJM197603112941104 [5] Ministry of Health (BR) (2011) Departamento de infor- mática do SUS. DATASUS, MS, Brasília. [6] Vianna, R.C.X.F., Moro, C.M.C.B., Moysés, S.J., Car- valho, D. and Nievola, J.C. (2010) Data mining and cha- racteristics of infant mortality. Cadernos de Saúde Pública, 26, 535-542. http://dx.doi.org/10.1590/S0102-311X2010000300011 [7] Barcellos, C., Ramalho, W.M., Gracie, R., Magalhães, M.A.F.M., Fontes, M.P. and Skaba, D. (2008) Geocoding health data in sub-municipal scale: Some Brazilian ex- periences. Epidemiologia e Serviços de Saúde, 17, 59-70. [8] Hau, L.C., Nascimento, L.F.C. and Tomazini, J.E. (2009) Geoprocessing to identify the pattern of birth profile in Vale do Paraíba. Revista Brasileira de Ginecologia e Ob- stetrícia, 31, 171-176. [9] Ipardes (201 1) Caderno est atís tico. Municí pio d e M a r ingá. http://www.ipardes.gov.br/modules/conteudo/conteudo.ph p?conteudo=5 [10] Santana, R.G., Udo, M.C.T., Previdelli, I.T.S. and Rodri- gues, A.L. (2010) Análise da ocupação residencial na Região Metropolitana de Maringá: A construção e apli- cação de uma tipologia. In: Rodrigues, A.L., Tonella, C. and Organizadores, Eds., Retratos da Região Metropoli- tana de Maringá: Subsídios para a Elaboração de Polí- ticas Públicas Participativas. Eduem, Maringá, 17-39. [11] Anselin, L. (1994) Local indicators of spatial association —LISA. Regional Research Institute, West Virginia Uni- versity, Virginia. [12] Predebon, K.M., Mathias, T.A.F., Aidar, T. and Rodrigues, A.L. (2010) Socio-spatial inequality expressed by indica- tors from the Information System on Live Births (SI- NASC). Cadernos de Saúde Pública, 26, 1583-1594. http://dx.doi.org/10.1590/S0102-311X2010000800012 [13] Oliveira, R.R., Costa, J.R. and Mathias, T.A.F. (2012) Spatial distribution and autocorrelation of infant mortality for three cities in Paraná state, Brazil. Geospatial Health, 6, 257-262. [14] Ventura, R.N., Oliveira, E.M., Silva, E.M., Silva, N.N. and Puccini, R.F. (2008) Living conditions and infant mortality in the municipality of Embu, São Paulo, Brazil. Revista Paulista de Pediatria, 26, 251-257. http://dx.doi.org/10.1590/S0103-05822008000300009 [15] Malta, D.C. and Duarte, E.C. (2007) Causes of avoidable mortality through effective healthcare services: A review of the literature. Ciência & Saúde Coletiva, 3, 765-776. http://dx.doi.org/10.1590/S1413-81232007000300027 [16] Victora, C.G., Aquino, E.M.L., Leal, M.C., Monteiro, C.A., Barros, F.C. and Szwarcwald, C.L. (2011) Saúde de mães e crianças no Brasil: Progressos e desafios. The Lancet, 6736, 32-46. [17] Silva, L.R., Christoffel, M.M. and Souza, K.V. (2005) History, conquests and perspectives of the woman and child care. Texto C on te xt o-Enferm, 14, 585-593. http://dx.doi.org/10.1590/S0104-07072005000400016 [18] Silva, A.C.M.A., Villar, M.A.M., Wuillaume, S.M. and Cardoso, M.H.C.A. (2009) Opinions by physicians from the Family Health Program on four health care priorities proposed by the agenda for commitment to comprehend- sive child health and reduction of infant mortality. Cad- ernos de Saúde Pública, 25, 349-358. http://dx.doi.org/10.1590/S0102-311X2009000200013 [19] Vilela, M.B.R., Bonfim, C. and Medeiros, Z. (2008) In- fant mortality due to infectious and parasitic diseases: A reflection of the social inequalities in a municipality in the Northeast Region of Brazil. Revista Brasileira de Saúde Materno Infantil, 8, 445-461. [20] Barros, F.C. and Victora, C.G. (2008) Maternal-child health in Pelotas, Rio Grande do Sul State, Brazil: Major conclusions from comparisons of the 1982, 1993, and 2004 bi rth cohorts. Cadernos de Saúde Pública, 24, S461- S467. http://dx.doi.org/10.1590/S0102-311X2008001500012 [21] Moilmaz, S.A.S., Garbin, C.A.S., Garbin, A.J.I., Zina, L.G., Yarid, S.D. and Francisco, K.M.S. (2010) Prenatal information system: Critical analysis of register in a mu- nicipality of São Paulo State. Revista Brasileira de Enfer- magem, 63, 385-390. [22] Grady, S.C. and Enander, H. (2009) Geographic analysis of low birthweight and infant mortality in Michigan using automated zoning methodology. International Journal of Health Geographics, 18, 8-10.
|