 World Journal of AIDS, 2013, 3, 207-215 http://dx.doi.org/10.4236/wja.2013.33028 Published Online September 2013 (http://www.scirp.org/journal/wja) 207 Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent Aline Domingos Pinto Ruppert1, Alexandre de Matos Soeiro2*, Maria Carolina F. de Almeida2, Vera Luiza Capelozzi1, Carlos V. Serrano Jr.2 1Department of Pathology, University of São Paulo Medical School, São Paulo, Brazil; 2Heart Institute, University of São Paulo Medical School, São Paulo, Brazil. Email: *alexandre.soeiro@bol.com.br Received May 27th, 2013; revised June 27th, 2013; accepted July 27th, 2013 Copyright © 2013 Aline Domingos Pinto Ruppert et al. This is an open access article distributed under the Creative Commons At- tribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is prop- erly cited. ABSTRACT Objectives: This study considers 489 autopsies of HIV/AIDS patients who died from acute respiratory failure and de- scribes the demographic data, etiology, and histological pulmonary findings of HIV associated diseases, comparing re- sults before and after introduction of antiretroviral therapy. Methods: The following data were obtained: age, sex, and major associated diseases (found at the autopsy). Pulmonary histopathology was categorized as: diffuse alveolar da- mage; pulmonary edema; alveolar hemorrhage; and acute interstitial pneumonia. Odds ratio of the HIV/AIDS-associ- ated diseases developing a specific histopathological pattern was determined by logistic regression. Results: A total of 355 men were studied. The mean age was 37 years old. Bronchopneumonia presented in 43% and Pneumocystis jiro- veci pneumonia in 38% of patients. Pulmonary histopathology showed diffuse alveolar damage in 31% and acute inter- stitial pneumonia in 23%. The multivariate analysis showed a significant and positive association between diffuse al- veolar damage with disseminated tuberculosis, cirrhosis and sepsis; and acu te interstitial pneumonia with Pneu mocystis jiroveci pneumonia and cytomegalovirosis. After the introduction of antiretroviral therapy we observed an increase in the prevalence of bacterial bronchopneumonia, sepsis and cirrhosis; and a decrease in Pneumocystis jiroveci pneumonia and cytomegalovirosis. Conclusions: Coh erent to literature, this study showed a decrease of respiratory failure mortality associated with some opportunistic infections after antiretroviral therapy introduction. But an increased prevalence of sepsis, bronchopneumonia and sepsis was observed too. The most prevalent pulmonary histopathological pattern was diffuse alveolar damage, which suggested a positive association with disseminated tuberculosis, sepsis an d cirrhosis. Keywords: AIDS; Acute Respiratory Failure; Pathology 1. Introduction The lungs have been the most frequent organs involved with AIDS-associated diseases leading to death. Acute respiratory failure (ARF) is the leading reason for inten- sive care unit (ICU) admission and the main cause of death of HIV-infected patients, mainly because of severe infectious diseases, like broncopneumonia and Pneumo- cystis jirovecipneumonia (PJP ) [ 1-8]. Many studies report changes in the causes of ARF af- ter the introduction of combination antiretroviral therapy (ART) [3,6,9], with a great impact on therapeutic of HIV-infected patients. But there is little recent informa- tion about pulmonary pathology associated with these changes and HIV-related diseases at autopsies. Based on information above, we performed a retro- spective study about 489 autopsies of patients with HIV/ AIDS whose cause of death was ARF in order to better describe the demographic data and etiological and histo- logical pulmonary findings for different HIV/AIDS-asso- ciated pathologies comparing before and after introduc- tion of ART. *Corresponding a uthor. Copyright © 2013 SciRes. WJA  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 208 2. Material and Methods 2.1. Autopsies The present study was carried out at a tertiary complex center. From 1990 to 2008, 26,560 medical autopsies were performed. ARF was the main cause of death in 4710 (17.7%) of patients. From these, the diagnosis of HIV/ AIDS was made in 489 cases (10.4%), who were includ- ed in the study. We performed a systemic review including all micro- scopic and macroscopic diagnosis of death at autopsy, and all medical records of the patients included. All clinical and postmortem data from patients enroll- ed in this study were collected with legal permission, after informed consent was obtained from a family me m- ber and after the approval of the Internal Review Boards. We excluded patients younger than one year of age, those without ARF and/or without HIV/AIDS. We also obtained data regarding each patient’s age, sex, and major underlying associated diseases (as determined at autopsy). Pulmonary histopathological analyses were performed in all HIV-infected cases. After a complete review, the most prevalent histopathological findings were categori- zed as: 1) Diffuse alveolar damage (DAD): diffuse involve- ment and uniform temporal appearance of alveolar col- lapse, hyaline membranes, obliterative fibrosis, neo-septa formation, and moderately organizing fibrosis 2) Pulmonary edema (PE): accumulation of proteina- ceous fluid in the alveolar spaces, giving the appearance of a granular, pink coagulate within suc h spaces 3) Alveolar hemorrhage (AH): presence of blood in the alveolar spaces 4) Acute interstitial pneumonia (AIP): widened and edematous alveolar septa, usually accompanied by mono- nuclear inflammatory infiltrate of lymphocytes, histiocy- tes, plasma cells, and neutrophils. All lungs were analyzed by microscopy even when medical records indicated the patient’s diagnosis. For at least four weeks, the lungs were fixed in 10% formalin prepared in 0.9% saline. We studied a minimum of five sections per lung (total ten sections per person) regard- less of the presence or absence of morphologically de- monstrable lesions. Paraffin-embedded tissue sections were assessed following haematoxylin and eosin staining. In order to document the presence and distribution of the wide spectrum of infectious agents to which this popula- tion is suscep tible, we pr epared a variety of special stains (Periodic acid-Schiff test, immunohistochemistry analy- sis, fluorescence, Ziehl-Neelsen, Gram, Mucicarmine, and Gomori’smethenamine silver stain) for selected tissue sections. Bacterial bronchopneumonia (BBP) was defin- ed as the presence of cell consolidation with polymer- phonuclear leukocyte accumulation in bronchioles and adjacent alveoli. For the diagnosis of cytomegalovirus (CMV) and fungal pneumonia, histological evidence of lung involvement was required with or without tissue culture. Severe sepsis and/or septic shock were defined as sepsis with the addition of organ dysfunction or clini- cal diagnosis of arterial hypotension, which may or may not be responsible for the aggressive fluid resuscitation. Diagnosis of Mycobacterium tuberculosis infection and atypical mycobacterial infection was confirmed using fluorescence and Ziehl-Neelsen techniques, and Lowen- stein-Jensen culture. The proportion method and bioche- mistry were used for identification of all positive cul- tures. 2.2. Statistical Analysis Descriptive analyses of the data collected from 1990 to 2008 included median, minimum, and maximum values. The probability (odds ratio) that the major AIDS-associ- ated diseases would develop a specific histopathological pattern was determined by logistic regression. All the sta- tistical procedures were performed using SPSS v10.0 sta- tistical software. Statistical significance was set at 5% (p value). We calculated prevalences related to demographic and etiologic data from two different periods, too: 1) First period (from 1990 to 2000)—period before an- tiretroviral therapy advent and transition of initial appli- cation to population (n = 319 patients). 2) Second period (from 2001 to 2008)—period after effective antiretroviral therapy advent, when the ART was well established (n = 170 patients). 3. Results 3.1. Total Period of Study (1990 to 2008) Demographic data from 1990 to 2008 are listed in Table 1. A total of 355 (72.6%) men and 134 (27.4%) women Table 1. Demographic analysis by gender and age taken from autopsies of patients with HIV/AIDS whose cause of death was IRA between the years 1990 and 2008. Sex Age Male Female Total 1 a 20 15 7 22 21 a 49 299 110 409 50 a 70 38 17 55 >70 3 0 3 Total 355 134 489 Copyright © 2013 SciRes. WJA  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent Copyright © 2013 SciRes. WJA 209 were included in the study. The age at the time of death was 21 to 50 years (409 patients) for most cases. Median age was 37. We observed a single HIV/AIDS-associated disease in 174 (35.6%) cases, two diseases in 158 (32.3%) cases, three diseases in 81 (16.6%) cases, and four diseases in 29 (5.9%) cases. No HIV/AIDS-associated diseases were detected in 47 patient s (9. 6% ) . The HIV/AIDS-associated diseases in patients with ARF are shown in Table 2. Between 1990 and 2008, BBP was present in 43.3% of patients (212 cases) and was the most frequent pulmonary complication found at the time of autopsy. In the same period, the pulmonary histopathological analysis showed DAD in 31.1% of patients (152 patients), The pulmonary histopathological findings observed in different HIV/AIDS-associated diseases are shown in Table 2. Table 2. Etiological diagnosis and histopathological pulmonary findings observed in lung autopsies of HIV-infected patients who presented IRA as cause of death, between 1990 and 2008. Associated Diseases DAD PE AH AIP Total Bacterial bronchopneumonia 58 23 24 33 212 Pneumocistisjiroveci pneumonia 56 3 14 82 186 Sepsis and/or septic shock 105 6 22 30 194 Cytomegalovirosis 33 1 13 48 103 Disseminated tu b erculosis 39 4 3 10 78 Toxoplasmosis 31 8 13 10 94 Pulmonary tuberculosis 36 5 10 9 87 Atypical mycobacterium tuberculosis 22 6 2 6 45 Kaposi sarcoma 19 2 6 11 52 Pulmonarythromboembolism 22 10 0 9 58 Neurocriptococcosis 6 2 0 8 17 Non-Hodkinlimphoma 5 6 3 3 17 Bacterialmeningitis 3 0 9 0 19 Limphoma 7 0 0 5 12 Histoplasmosis 7 0 4 0 11 Livercirrhosis 16 9 1 5 38 Schistossomosis 8 0 0 0 8 Acuteperitonitis 4 0 0 3 7 Bacterialendocarditis 4 0 0 0 4 Pulmonarycriptococcosis 3 3 1 0 10 Neurocisticercosis 2 2 0 4 8 Chronicpneumopathy 0 3 0 0 3 Pielonefritis 0 0 2 4 6 Disseminated neoplasy 2 0 0 2 4 Neuropathy 2 0 0 0 2 Duodenal ulcer 4 0 0 4 8 Acute Renal Failure 12 0 0 3 15 Chronicpancreatitis 4 3 7 3 17 Deepvenousthrombosis 4 0 0 0 4 Aspergilosis 0 0 0 0 1 *DAD = diffuse alveolar damage; PE = pulmonary edema; AIP = acute interstitial pneumonia; HA = alveolar hemorrhage.  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 210 Multivariate analysis with association between HIV/ AIDS-associated diseases and histologic patterns is avail- able in Table 3. 3.2. Comparing before and after ART’ Periods Demographic data from these periods can be verified in Table 4. In the first period we observed a prevalence of 21% women and 79% men, whereas in the second period these numbers were, respectively, 32% and 68%. BBP was the most prevalent HIV/AIDS-associated di- sease in both periods, as we can observe comparatively in Table 5. We observed the inversion in prevalence of AIP and DAD, in the first period AIP was more prevalent, and in the second, DAD was, as exposed in Table 6. 4. Discussion This is the biggest study in au topsies that include s demo- graphic data, etiologic diagnose and respective pulmo- nary histopathological records from HIV/AIDS patients, whose cause of death was ARF. Between 1990 and 2008, diagnose of HIV/AIDS was made in 489 autopsies. As comented, BBP was present in 43.3% and Pneumocystis jiroveci pneumonia in 38.0% of patients. The pulmonary histopathological patterns were, in descending order: DAD in 31.1% of patients, AIP in 23.5%, PE in 9.4%, e AH in 9.0% of patients. The multivariate analysis show- ed significant an d positive association b etween DAD and: disseminated tuberculosis, liver cirrhosis e sepsis and/or septic shock; and between AIP and: Pneumocystis jirove- ci pneumonia and cytomegalovirosis. From the first descriptions of HIV/AIDS, the lung has been the site most often affected by the disease and its complications. Pulmonary involvement has been reported in 80% - 94% of patients with HIV/AIDS-associated di- seases [10]. Despite recent technological advances in dia- gnosis, the autopsy has remained an important comple- mentary tool for the identification and understanding of diseases in patients with HIV/AIDS [11]. Recent autopsy studies have shown important differences between autop- sy findings and the clinical diagnosis antemortem in this group of patients [10- 12]. In the present study, we observed a high prevalence (17.7%) of patients with HIV/AIDS who also had ARF as the cause of death. Most analyzed patients were males (72.6%) and the mean age was 37 years, similar with da- ta from studies in other countries [10-14]. An autopsy study of patients with HIV/AIDS, per- formed in the United States, Afessa et al. showed the presence of two or more associated diagnoses in 52% of the cases studied, [11] what is consistent to the result of Table 3. Multivariate analysis with major diseases found in autopsies of patients with HIV/AIDS, and the ir rel ationships with their respective lung histopathology. Pulmonary Histopathological Patterns DAD PE AH AIP Associated Diseases p** OR CI 95% p** ORCI 95% p** ORCI 95% p** OR CI 95% Bacterial bronchopneumonia NS 0.686 0.561 - 1.837NS1.2930.708 - 2.361NS1.6530.887 - 3.081 0.001 0 .443 0.282 - 0.696 Pneumocistisjiroveci pneumonia NS 0.753 0.451 - 1.2550.0050.1770. 042 - 0.745NS0.6720.275 - 1.642 0.01 4.904 3.016 - 7.972 Sepsis and/or septic shoc k 0.015 2.987 1.83 - 4.875NS0.3250.098 - 1.074NS1.1570.517 - 2.593 NS 0.588 0.312 - 1.109 Cytomegalovirosis NS 0.888 0.452 - 1.744NS0.1980.027 - 1.468NS1.3040.487 - 3.497 0.02 3.631 1.938 - 6.8 Disseminated tuberculosis 0.048 1.942 1.024 - 3.684NS0.7080. 21 - 2.368NS0.7650.227 - 2.586 0.023 0.321 0.112 - 0.918 Toxoplasmosis NS 1.028 0.517 - 2.044NS1.0230.348 - 3.008NS1.4640.543 - 3.945 NS 0.429 0.164 - 1.121 Pulmonary tuberculosis NS 1.641 0.821 - 3.278NS0.5360.125 - 2.305NS1.2970.437 - 3.853 NS 0.387 0.134 - 1.12 Aypical micobacteriosis NS 1.563 0.653 - 3.738NS2.2020.713 - 6.801NS0.4720.062 - 3.594 NS 0.315 0.073 - 1.369 Kaposi sarcoma NS 1.277 0.524 - 3.111NS0.4380.058 - 3.331NS1.6480.468 - 5.806 NS 0.717 0.238 - 2.162 Pulmonary Thromboembolism NS 1.188 0.493 - 2.865NS2.8170.996 - 7.973NS0.9490.928 - 0.969 NS 0.677 0.226 - 2.032 Limphoma NS 3.36 0.56 - 20.317NS0.9890.979 - 0.9990.0467. 0482.145 - 43.37 NS 2.201 0.363 - 13.33 Livercirrhosis 0.042 3.053 1.041 - 8.957NS1.60.347 - 7.375NS0.9690.953 - 0.985 NS 0.537 0.118 - 2.435 Schstossomosis NS 1.02 0.997 - 1.043NS0.9930.986 - 1.001NS0.9930.986 - 1.001 NS 1.64 0.147 - 18.26 *DAD = diffuse alveolar damage; PE = pulmonary edema; AIP = acute interstitial pneumonia; AH = alveolar hemorrhage; OR = odds ratio; CI = confidence interval; NS = not significant; **significant at p < 0.05. Copyright © 2013 SciRes. WJA  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 211 Table 4. Demographic comparative analysis of age in before and after anti-retroviral advent found in autopsies of pa- tients with HIV/AIDS whose cause of death was IRA. 1990-2000 2001-2008 Age n (%) n (%) 1a 20 18 5.64% 4 2.35% 21 a 49 277 86.83% 132 77.65% 50 a 70 22 6.90% 33 19.41% >70 2 0.01% 1 0.01% *n = number of cases. 55% we found. Hence, an important association between different pulmonary diseases in patients with HIV/AIDS and ARF was established, which could indicate the ne- cessity of a different therapeutic strategy for these pa- tients. Comparing our results about the period of 2001 to 2008 with the period between 1990 and 2000, we ob- serve some changes on HIV/AIDS’ infection profile. First, there was a decrease of incidence of HIV-infected patients at autopsies, probably due to better efficacy and distribution of antiretroviral therapy, and recent techno- logical advances in diagnosis. Although age between 21 and 40 years old remained the most affected by ARF as cause of death, there was a decrease in patients younger than 20 years old and an important increase in prevalence of patients older than 41 years old, confirming the aging of HIV/AIDS infected patients after the introduction of ART. Besides this, it seems to happen the feminization process of HIV infection, with an increase of prevalence rates of infected women from 21%, in the first period, to 27.4% in the second one. There was an important increase of incidence of BBP (from 36% in the fist period to 47% in the second), sepsis and/or septic shock (from 14% to 22%), liver cirrhosis (from 1.2% to 13.5%). We observed a substantial de- crease in prevalence rates of Pneumocystis jiroveci pneu- monia (from 27% to 10%), cytomegalovirosis (from 13.2% to 5.8%), neurocriptococcosis (from 2.8% to 0%) and atypical mycobacteriosis (from 6% to 3.5%). The other diseases kept constant their prevalences in both pe- riods, with negligible fluctuations. BBP was the most often pulmonary disease found at autopsies in both decades, and was present in 43.3% of patients (212 cases). Patients with HIV are at increased risk for BBP [13,15,16]. Studies have reported greater than 17 times the incidence of bacterial pneumon ia in HIV- infected patients compared to the general population [17]. Effects of HIV infection that predispose patients to lung infections include depletion of alveolar CD4 T cells, im- pairment of humoral immunity, and functional alterations of granulocytes and alveolar macrophages [18,19]. BBP may also be responsible for more than half of all cases of respiratory failure requiring ICU admission in HIV-in- fected patients [6]. In our study, we observed an increase in prevalence of BBP in the second period, after ART. The impact of HAART on the development of bacterial pneumonia requiring ICU admission is not entirely clear. Some studies have shown no major changes in the pro- portion of HIV-infected patients admitted to the ICU for bacterial pneumonia [20]. Other studies, however, indi- cate the increase in the incidence and mortality by b acte- rial infections in the second period [21]. The mortality rates of HIV-infected patients with BBP reached 20% in some estudos [13]. From 1990 to 2008, sepsis/sep tic shock was present in 40.0% of patients with HIV/AIDS. In the literature, the rates of hospitalization in intensive care units for sepsis and/or septic shock in patients infected with HIV range from 11% to 23% [8,22-24]. At the early decades of HIV, sepsis was responsible fo r over than 15% of sero positive cases admitted in intensive therapy [25]. After introduc- tion of ART, there was a trend of increasing incidence and mortality due to sepse [3,20], representing 45% of hospitalizations [21]. These data are consonant with our study, which showed an increase in cases of sepsis in the post HAART. Patients with septic shock may have dys- function of the adrenal glands. In HIV-infected patients, the direct activity of HIV in the adrenal glands, related opportunistic diseases that affect them, and the medica- tions used to treat these patients may contribute to the failure adrenal [25,28]. Therefore, physiological parame- ters and personalized therapies for HIV-infected patients with sepsis/septic shock, need to be investigated [25-28]. After ART advent, a decrease in incidence of Pneumo- cystis jiroveci pneumonia has been a worldwide pheno- menon. In literature, the incidence of Pneumocystis jiro- veci pneumonia in HIV-infected patients is 7% to 24% [4,6,8,22,24,29,30]. Similar to literature, our study show- ed a decrease of prevalence rates from 27% to 10% in the period after ART. During the earliest days of the AIDS epidemic, PJP resulting in respiratory failure was an al- most universally fatal illness [5]. While there have been considerable advances in the care of HIV-infected pa- tients over the last years, PJP, although its decrease, re- mains one of the most common etiologies for respiratory failure requiring ICU admission in HIV-infected patients, and its mortality remains high [4,8,22,30-32]. Several recent studies have shown that between one quarter and one third of all ICU admission s of HIV infec- ted patients are due to Pneumocystis jiroveci pneumonia [6,8,32]. Pulmonary tuberculosis was found in 17.8% of the cases in the whole period of our study. Autopsy studies have found the presence of Mycobacterium tuberculosis Copyright © 2013 SciRes. WJA 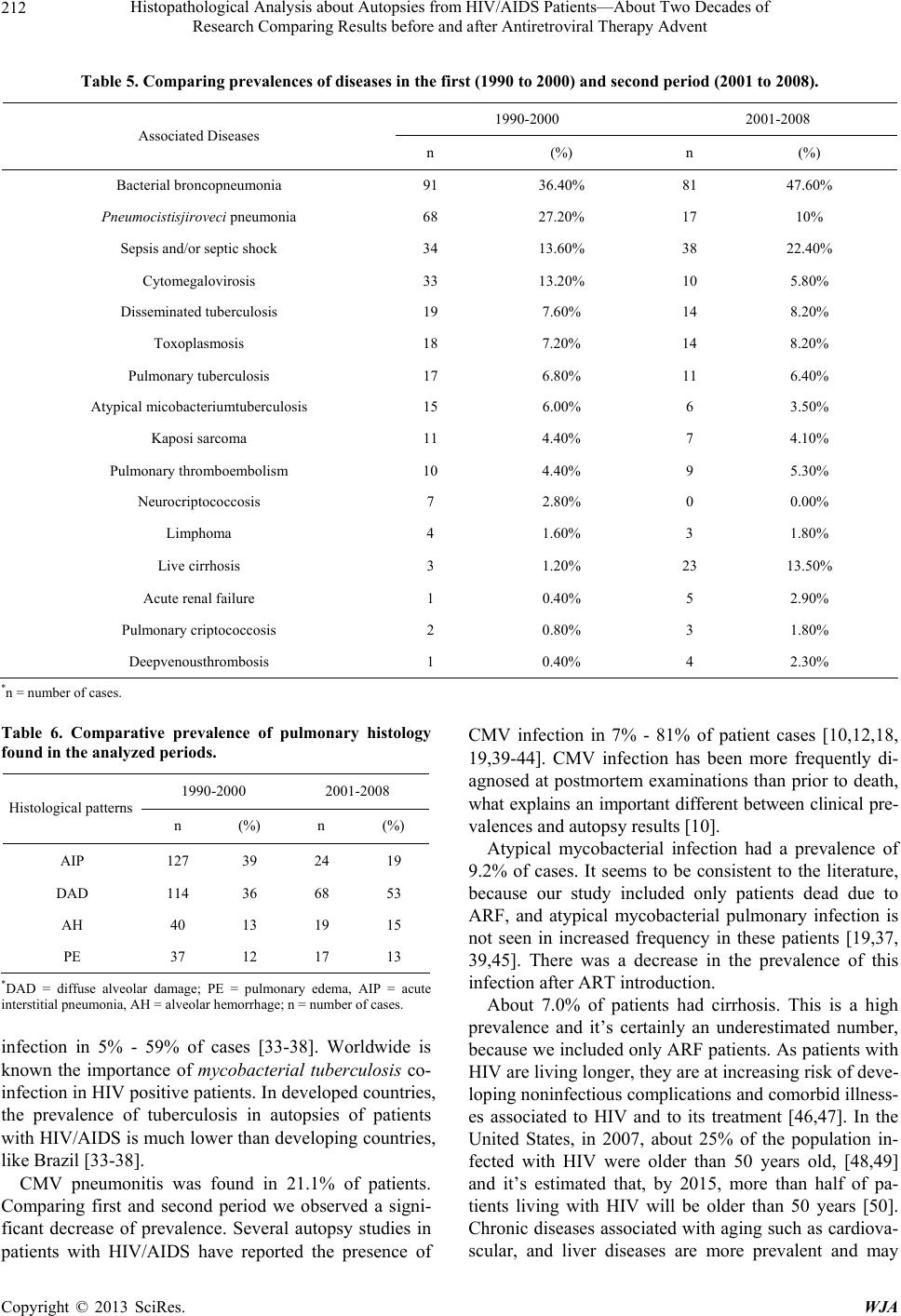 Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 212 Table 5. Comparing prevalences of diseases in the first (1990 to 2000) and second period (2001 to 2008). 1990-2000 2001-2008 Associated Diseases n (%) n (%) Bacterial broncopneumonia 91 36.40% 81 47.60% Pneumocistisjiroveci pneumonia 68 27.20% 17 10% Sepsis and/or septic shock 34 13.60% 38 22.40% Cytomegalovirosis 33 13.20% 10 5.80% Disseminated tube rculosis 19 7.60% 14 8.20% Toxoplasmosis 18 7.20% 14 8.20% Pulmonary tuberculosis 17 6.80% 11 6.40% Atypical micobacteriumtuberculosis 15 6.00% 6 3.50% Kaposi sarcoma 11 4.40% 7 4.10% Pulmonary thromboembolism 10 4.40% 9 5.30% Neurocriptococcosis 7 2.80% 0 0.00% Limphoma 4 1.60% 3 1.80% Live cirrhosis 3 1.20% 23 13.50% Acute renal fail ure 1 0.40% 5 2.90% Pulmonary criptococcosis 2 0.80% 3 1.80% Deepvenousthrombosis 1 0.40% 4 2.30% *n = number of cases. Table 6. Comparative prevalence of pulmonary histology found in the analyzed periods. 1990-2000 2001-2008 Histological patterns n (%) n (%) AIP 127 39 24 19 DAD 114 36 68 53 AH 40 13 19 15 PE 37 12 17 13 *DAD = diffuse alveolar damage; PE = pulmonary edema, AIP = acute interstitial pneumonia, AH = alveolar hemorrhage; n = number of cases. infection in 5% - 59% of cases [33-38]. Worldwide is known the importance of mycobacterial tuberculosis co- infection in HIV positive patients. In developed coun tries, the prevalence of tuberculosis in autopsies of patients with HIV/AIDS is much lower than developing countries, like Brazil [33-38]. CMV pneumonitis was found in 21.1% of patients. Comparing first and second period we observed a signi- ficant decrease of prevalence. Several autopsy studies in patients with HIV/AIDS have reported the presence of CMV infection in 7% - 81% of patient cases [10,12,18, 19,39-44]. CMV infection has been more frequently di- agnosed at postmortem examinations than prior to death, what explains an important different between clinical pre- valences and autopsy results [10]. Atypical mycobacterial infection had a prevalence of 9.2% of cases. It seems to be consistent to the literature, because our study included only patients dead due to ARF, and atypical mycobacterial pulmonary infection is not seen in increased frequency in these patients [19,37, 39,45]. There was a decrease in the prevalence of this infection after ART introduction. About 7.0% of patients had cirrhosis. This is a high prevalence and it’s certainly an underestimated number, because we included only ARF patients. As patients with HIV are living longer, they are at increasing risk of deve- loping non infectious complic ations and comorb id illn ess- es associated to HIV and to its treatment [46,47]. In the United States, in 2007, about 25% of the population in- fected with HIV were older than 50 years old, [48,49] and it’s estimated that, by 2015, more than half of pa- tients living with HIV will be older than 50 years [50]. Chronic diseases associated with aging such as cardiova- scular, and liver diseases are more prevalent and may Copyright © 2013 SciRes. WJA 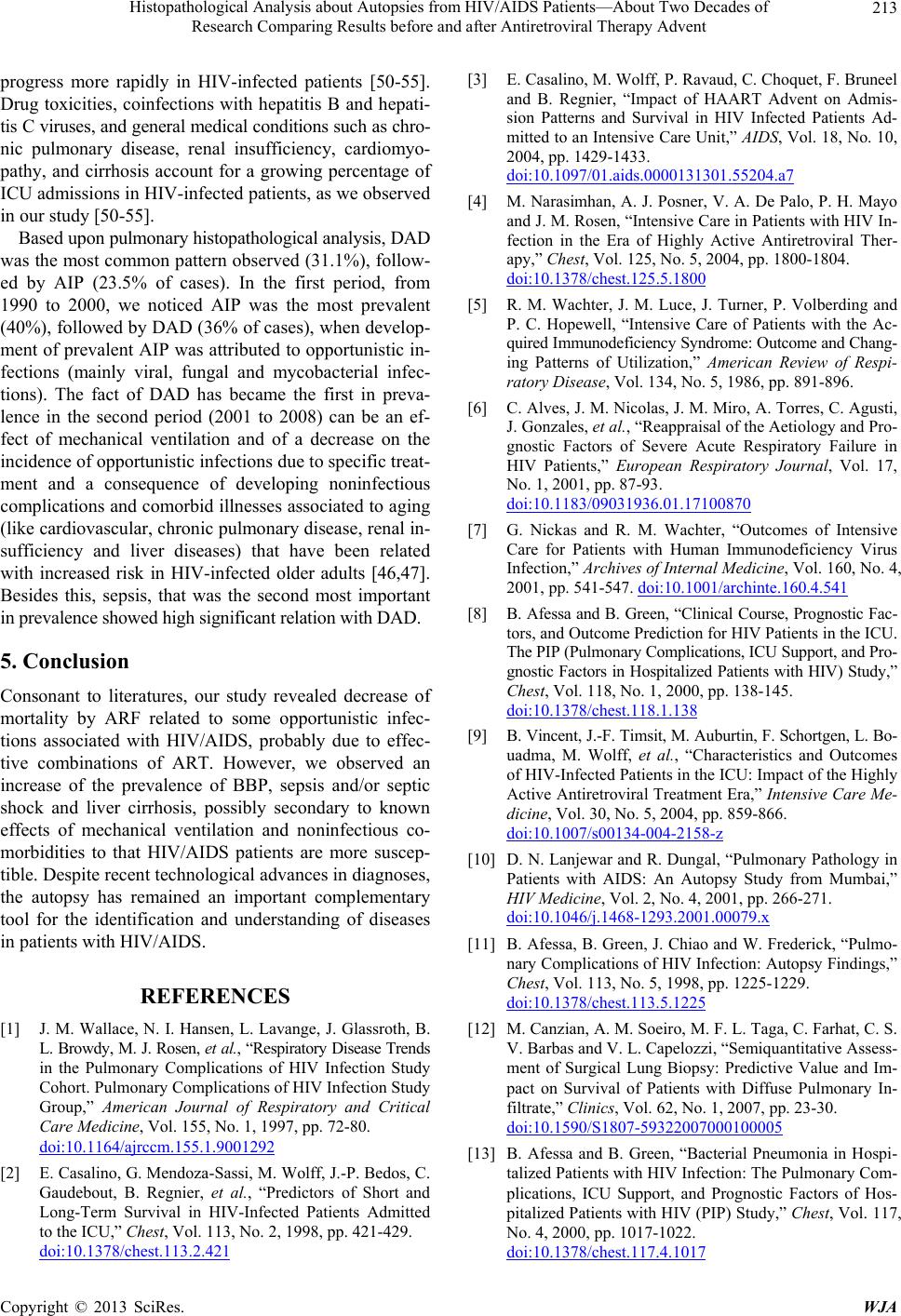 Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 213 progress more rapidly in HIV-infected patients [50-55]. Drug toxicities, coinfections with hepatitis B and hepati- tis C viruses, and general medical conditions such as chro- nic pulmonary disease, renal insufficiency, cardiomyo- pathy, and cirrhosis account for a growing percentage of ICU admissions in HIV-infected patients, as we observed in our study [50-55]. Based upon pulmonary histopathological analysis, DAD was the most common pattern observed (31.1%), follow- ed by AIP (23.5% of cases). In the first period, from 1990 to 2000, we noticed AIP was the most prevalent (40%), followed by DAD (36% of cases), when develop- ment of prevalent AIP was attributed to opportunistic in- fections (mainly viral, fungal and mycobacterial infec- tions). The fact of DAD has became the first in preva- lence in the second period (2001 to 2008) can be an ef- fect of mechanical ventilation and of a decrease on the incidence of opportunistic infections due to specific treat- ment and a consequence of developing noninfectious complications and comorbid illnesses asso ciated to aging (like cardiovascular, chronic pulmonary disease, renal in- sufficiency and liver diseases) that have been related with increased risk in HIV-infected older adults [46,47]. Besides this, sepsis, that was the second most important in prevalence showed high significant relation with DAD. 5. Conclusion Consonant to literatures, our study revealed decrease of mortality by ARF related to some opportunistic infec- tions associated with HIV/AIDS, probably due to effec- tive combinations of ART. However, we observed an increase of the prevalence of BBP, sepsis and/or septic shock and liver cirrhosis, possibly secondary to known effects of mechanical ventilation and noninfectious co- morbidities to that HIV/AIDS patients are more suscep- tible. Despite recent technological advances in diagnoses, the autopsy has remained an important complementary tool for the identification and understanding of diseases in patients with HIV/AIDS. REFERENCES [1] J. M. Wallace, N. I. Hansen, L. Lavange, J. Glassroth, B. L. Browdy , M. J. Rosen, et al., “Respiratory Disease Trends in the Pulmonary Complications of HIV Infection Study Cohort. Pulmonary Complications of HIV Infection Study Group,” American Journal of Respiratory and Critical Care Medicine, Vol. 155, No. 1, 1997, pp. 72-80. doi:10.1164/ajrccm.155.1.9001292 [2] E. Casalino, G. Mendoza-Sassi, M. Wolff, J.-P. Bedos, C. Gaudebout, B. Regnier, et al., “Predictors of Short and Long-Term Survival in HIV-Infected Patients Admitted to the ICU,” Chest, Vol. 113, No. 2, 1998, pp. 421-429. doi:10.1378/chest.113.2.421 [3] E. Casalino, M. Wolff, P. Ravaud, C. Choquet, F. Bruneel and B. Regnier, “Impact of HAART Advent on Admis- sion Patterns and Survival in HIV Infected Patients Ad- mitted to an Intensive Care Unit,” AIDS, Vol. 18, No. 10, 2004, pp. 1429-1433. doi:10.1097/01.aids.0000131301.55204.a7 [4] M. Narasimhan, A. J. Posne r, V. A. De Palo, P. H. Mayo and J. M. Rosen, “Intensive Care in Patients with HIV In- fection in the Era of Highly Active Antiretroviral Ther- apy,” Chest, Vol. 125, No. 5, 2004, pp. 1800-1804. doi:10.1378/chest.125.5.1800 [5] R. M. Wachter, J. M. Luce, J. Turner, P. Volberding and P. C. Hopewell, “Intensive Care of Patients with the Ac- quired Immunodeficiency Syndrome: Outcome and Chang- ing Patterns of Utilization,” American Review of Respi- ratory Disease, Vol. 134, No. 5, 1986, pp. 891-896. [6] C. Alves, J. M. Nicolas, J. M. Miro, A. Torres, C. Agusti, J. Gonzales, et al., “Reappraisal of the Aetiology and Pro- gnostic Factors of Severe Acute Respiratory Failure in HIV Patients,” European Respiratory Journal, Vol. 17, No. 1, 2001, pp. 87-93. doi:10.1183/09031936.01.17100870 [7] G. Nickas and R. M. Wachter, “Outcomes of Intensive Care for Patients with Human Immunodeficiency Virus Infection,” Archives of Internal Medicine, Vol. 160, No. 4, 2001, pp. 541-547. doi:10.1001/archinte.160.4.541 [8] B. Afessa and B. Green, “Clinical Course, Progno stic Fac- tors, and Outcome Prediction for HIV Patients in the ICU. The PIP (Pulmonary Complications, ICU Support, a nd Pro- gnostic Factors in Hospitalized Patients with HIV) Study,” Chest, Vol. 118, No. 1, 2000, pp. 138-145. doi:10.1378/chest.118.1.138 [9] B. Vincent, J.-F. Timsit, M. Auburtin, F. Schortge n, L. Bo- uadma, M. Wolff, et al., “Characteristics and Outcomes of HIV-Infected Patients in the ICU: Impact of the Highly Active Antiretroviral Treatment Era,” Intensive Care Me- dicine, Vol. 30, No. 5, 2004, pp. 859-866. doi:10.1007/s00134-004-2158-z [10] D. N. Lanjewar and R. Dungal, “Pulmonary Pathology in Patients with AIDS: An Autopsy Study from Mumbai,” HIV Medicine, Vol. 2, No. 4, 2001, pp. 266-271. doi:10.1046/j.1468-1293.2001.00079.x [11] B. Afessa, B. Green, J. Chiao and W. Frederick, “Pulmo- nary Complications of HIV Infection: Autopsy Findings,” Chest, Vol. 113, No. 5, 1998, pp. 1225-1229. doi:10.1378/chest.113.5.1225 [12] M. Canzian, A. M. Soeiro, M. F. L. Taga, C. Farhat, C. S. V. Barbas and V. L. Capelozzi, “Semiquantitative Assess- ment of Surgical Lung Biopsy: Predictive Value and Im- pact on Survival of Patients with Diffuse Pulmonary In- filtrate,” Clinics, Vol. 62, No. 1, 2007, pp. 23-30. doi:10.1590/S1807-59322007000100005 [13] B. Afessa and B. Green, “Bacterial Pneumonia in Hospi- talized Patients with HIV Infection: The Pulmonary Com- plications, ICU Support, and Prognostic Factors of Hos- pitalized Patients with HIV (PIP) Study,” Chest, Vol. 117, No. 4, 2000, pp. 1017-1022. doi:10.1378/chest.117.4.1017 Copyright © 2013 SciRes. WJA  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent 214 [14] A. M. Soeiro, A. L. D. Hovnanian, E. R. Parra, M. Canzi- an and V. L. Capelozzi, “Post-Mortem Histological Pul- monary Analysis in Patients with HIV/AIDS,” Clinics, Vol. 63, No. 4, 2008, pp. 497-502. doi:10.1590/S1807-59322008000400014 [15] R. E. Hirschtic k, J. Glassroth, M. C. Jordan, et al. , “Bacte- rial Pneumonia in Persons Infected with the Human Im- munodeficiency Virus. Pulmonary Complications of HIV Infection Study Group,” The New England Journal of Medicine, Vol. 333, No. 13, 1995, pp. 845-851. doi:10.1056/NEJM199509283331305 [16] B. Polsky, J. W. Gold, E. Whimbey, et al., “Bacterial Pne- umonia in Patients with the Acquired Immunodeficiency Syndrome,” Annals of Internal Medicine, Vol. 104, No. 1, 1986, pp. 38-41. doi:10.7326/0003-4819-104-1-38 [17] D. J. Witt, D. E. Craven and W. R. McCabe, “Bacterial In- fections in Adult Patients with the Acquired Immune De- ficiency Syndrome (AIDS) and AIDS-Related Complex,” American Journal of Medicine, Vol. 82, No. 5, 1987, pp. 900-906. doi:10.1016/0002-9343(87)90150-1 [18] K. Ohtomo, S. Wang, A. Masunaga and I. Sugawara, “Se- condary Infections of AIDS Autopsy Cases in Japan with Special Emphasis on Mycobacterium Avium-Intracellu- lare Complex Infection,” The Tohoku Journal of Experi- mental Medicine, Vol. 192, No. 2, 2000, pp. 99-109. doi:10.1620/tjem.192.99 [19] R. McKenzie, W. D. Travis, S. A. Dolan, S. Pittaluga, I. M. Feuerstein, J. Shelhamer, et al., “The Causes of Death in Patients with Human Immunodeficiency Virus Infec- tion: A Clinical and Pathologic Study with Emphasis on the Role of Pulmonary Diseases,” Medicine (Baltimore), Vol. 70, No. 5, 1991, pp. 326-343. doi:10.1097/00005792-199109000-00004 [20] R. Nuesch, N. Geigy, E. Schaedler and M. Battegay, “Ef- fect of Highly Active Antiretroviral Therapy on Hospita- lization Characteristics of HIV-Infected Patients,” Euro- pean Journal of Clinical Microbiology & Infectious Dis- eases, Vol. 21, No. 9, 2002, pp. 684-687. doi:10.1007/s10096-002-0792-3 [21] A. L. Rosenb erg, M. G. S eneff , L. Ati yeh, R. Wag ner, L. Bo- janowski and J. E. Zimmerman, “The Importance of Bac- terial Sepsis in Intensive Care Unit Patients with Acquir- ed Immunodeficiency Syndrome: Implications for Future Care in the Age of Increasing Antiretroviral Resistance,” Critical Care Medicine, Vol. 29, No. 3, 2001, pp. 548- 556. doi:10.1097/00003246-200103000-00013 [22] A. Morris, J. Creasman, J. Turner, J. M. Luce, R. M. Wa- chter and L. Huang, “Intensive Care of Human Immuno- deficiency Virus-Infected Patients during the Era of Hi- ghly Active Antiretroviral Therapy,” American Journal of Respiratory and Critical Care Medicine, Vol. 166, No. 3, 2002, pp. 262-267. doi:10.1164/rccm.2111025 [23] H. Khouli, A. Afrasiabi, M. Shibli, R. Hajal, C. R. Barrett and P. Homel, “Outcome of Critically Ill Human Immu- nodeficiency Virus-Infected Patients in the Era of Highly Active Antiretroviral Therapy,” Journal of Intensive Care Medicine, Vol. 20, No. 6, 2005, pp. 327-333. doi:10.1177/0885066605281087 [24] K. Powell, J. L. Davis, A. M. Morris, A. Chi, M. R. Ben- sley and L. Huang, “Survival for Patients with HIV Ad- mitted to the ICU Continues to Improve in the Current Era of Combination Antiretroviral Therapy,” Chest, Vol. 135, No. 1, 2009, pp. 11-17. doi:10.1378/chest.08-0980 [25] B. J. Glasgow, K. D. Steinsapir, K. Anders and L. J. Lay- field, “Adrenal Pathology in the Acquired Immune Defi- ciency Syndrome,” American Journal of Clinical Patho- logy, Vol. 84, No. 5, 1985, pp. 594-597. [26] U. Pulakhandam and H. P. Dincsoy, “Cytomegalovirala- drenalitis and Adrenal Insufficiency in AIDS,” American Journal of Clinical Pathology, Vol. 93, No. 5, 1990, pp. 651-656. [27] K. Welch, W. Finkbeiner, C. E. Alpers, et al., “Autopsy Findings in the Acquired Immune Deficiency Syndrome,” JAMA, Vol. 252, No. 9, 1984, pp. 1152-1159. doi:10.1001/jama.1984.03350090028018 [28] N. Sonino, “The Use of Ketoconazole as an Inhibitor of Steroid Production,” The New England Journal of Medi- cine, Vol. 317, No. 13, 1987, pp. 812-818. doi:10.1056/NEJM198709243171307 [29] A. Torres, M. El-Ebiary, R. Marrades, et al., “Aetiology and Prognostic Factors of Patients with AIDS Presenting Life Threatening Acute Respiratory Failure,” European Respiratory Journal, Vol. 8, No. 11, 1995, pp. 1922-1928. doi:10.1183/09031936.95.08111922 [30] M. J. Rosen, K. Cla yton, R. F. Schneider, et al., “Intensive Care of Patients with HIV Infection: Utilization, Critical Illnesses, and Outcomes. Pulmonary Complications of HIV Infection Study Group,” American Journal of Respiratory and Critical Care Medicine, Vol. 155, No. 1, 1997, pp. 67-71. doi:10.1164/ajrccm.155.1.9001291 [31] N. G. Mansharamani, R. Garland, D. Delaney and H. Ko- ziel, “Management and Outcome Patterns for Adult Pneu- mocystis Carinii Pneumonia, 198 5 to 1995: Comparison of HIV-Associated Cases to Other Immunocompromised States,” Chest, Vol. 118, No. 3, 2000, pp. 704-711. doi:10.1378/chest.118.3.704 [32] R. F. Miller, E. Allen, A. Copas, M. Singer and S. G. Ed- wards, “Improved Survival for HIV Infected Patients with Severe Pneumocystis Jirovecii Pneumonia Is Independent of Highly Active Antiretroviral Therapy,” Thorax, Vol. 61, No. 8, 2006, pp. 716-721. doi:10.1136/thx.2005.055905 [33] J. K. Gill, L. Greene, R. Miller, et al., “ICU Admission in Pa- tients Infected with the Human Immunodeficiency Virus: A Multicentre Survey,” Anaesthesia, Vol. 54, No. 8, 1999, pp. 727-732. doi:10.1046/j.1365-2044.1999.00903.x [34] R. Chakraborty , A. Pulve r, L. S. Pulver, R. Muso ke, T. Pa - lakudy, A. D’Agostino, et al., “The Post-Mortem Pathol- ogy of HIV-1-Infected African Children,” Annals of Tro- pical Paediatrics, Vol. 22, No. 2, 2002, pp. 125-131. doi:10.1179/027249302125000841 [35] F. S. Rana, M. P. Hawken, C. Mwachari, S. M. Bhatt, F. Ab- dullah, L. W. Ng’ang’a, et al., “Autopsy Study of HIV-1- Positive and HIV-1-Negative Adult Medical Patients in Nairobi, Kenya,” Journal of Acquired Immune Deficiency Syndromes, Vol. 24, No. 1, 2000, pp. 23-29. [36] N. A. Ansari, A. H. Kombe, T. A. Kenyon, N. M. Hone, J. Copyright © 2013 SciRes. WJA  Histopathological Analysis about Autopsies from HIV/AIDS Patients—About Two Decades of Research Comparing Results before and after Antiretroviral Therapy Advent Copyright © 2013 SciRes. WJA 215 W. Tappero, S. T. Nyirenda, et al., “Pathology and Causes of Death in a Group of 128 Predominantly HIV-Positive Patients in Botswana, 1997-1 998,” The International Jour- nal of Tuberculosis and Lung Disease, Vol. 6, No. 1, 2002, pp. 55-63. [37] A. d’Arminio Monforte, L. Vago, A. Gori, S. Antinori, F. Franzetti, C. M. Antonacci, et al., “Clinical Diagnosis of Mycobacterial Diseases versus Autopsy Findings in 350 Patients with AIDS,” European Journal of Clinical Mi- crobiology and Infectious Diseases, Vol. 15, No. 6, 1996, pp. 453-458. doi:10.1007/BF01691311 [38] M. N. Dhatz, K. Domoua, G. Coulibaly, F. Traore, J. B. Konan, A. Beaumel, et al., “Pulmonary Diseases and Ret- rovirus Infections. A Pathological Study in 70 Cases,” Revue de Pneumologie Clinique, Vol. 49, No. 5, 1993, pp. 211-215. [39] P. M. Cury, C. F. Pulido, V. M. Furtado a nd F. M. Palma, “Autopsy Findings in AIDS Patients from a Reference Hospital in Brazil: Analysis of 92 Cases,” Pathology- Research and Practice, Vol. 199, No. 12, 2003, pp. 811- 814. doi:10.1078/0344-0338-00500 [40] H. J. Tang, Y. C. Liu, M. Y. Yen, Y. S. Chen, S. R. Wann, H. H. Lin, et al., “Opportunistic Infections in Adults with Acquired Immunodeficiency Syndrome: A Comparison of Clinical and Autopsy Findings,” Journal of Microbio- logy, Immunology, and Infection, Vol. 39, No. 4, 2006, pp. 310-315. [41] D. Eza, G. Cerrillo, D. A. Moore, C. Castro, E. Ticona, D. Morales et al., “Postmortem Findings and Opportunistic Infections in HIV-Positive Patients from a Public Hospi- tal in Peru,” Pathology, Research and Practice, Vol. 202, No. 11, 2006, pp. 767-775. [42] J. G. Netto, D. C. Collarile, A. F. Borges, M. L. Bianca- lana and H. N. Stefano, “Necroscopic Findings in Patients with Acquired Immunodeficiency Syndrome,” Revista Paulista de Medicina, Vol. 108, No. 5, 1990, pp. 205- 212. [43] E. C. Klatt and D. Shibata, “Cytomegalovirus Infection in the Acquired Immunodeficiency Syndrome. Clinical and Autopsy Findings,” Archives of Pathology & Laboratory Medicine, Vol. 112, No. 5, 1988, pp. 540-544. [44] J. M. Wallace and J. Hannah, “Cytomegalovirus Pneumo- nitis in Patients with AIDS. Findings in an Autopsy Se- ries,” Chest, Vol. 92, No. 2, 1987, pp. 198-203. doi:10.1378/chest.92.2.198 [45] P. Saleeb and K. N. Olivier, “Pulmonary Nontuberculous Mycobacterial Disease: New Insights into Risk Factors for Susceptibility, Epidemiology, and Approaches to Management in Immunocompetent and Immunocompro- mised Patients,” Current Infectious Disease Reports, Vol. 12, No. 3, 2010, pp. 198-203. doi:10.1007/s11908-010-0103-6 [46] N. F. Crum, R. H. Riffenburgh, S. Wegner, et al., “Com- parisons of Causes of Death and Mortality Rates among HIV-Infected Persons: Analysis of the Pre-, Early, and Late HAART (Highly Active Antiretroviral Therapy) Eras,” Journal of Acquired Immune Deficiency Syn- dromes, Vol. 41, No. 2, 2006, pp. 194-200. doi:10.1097/01.qai.0000179459.31562.16 [47] R. S. Braithwaite, A. C. Justice, C. C. Chang, et al., “Es- timating the Proportion of Patients Infected with HIV Who Will Die of Comorbid Diseases,” The American Journal of Medicine, Vol. 118, No. 8, 2005, pp. 890-898. doi:10.1016/j.amjmed.2004.12.034 [48] K. A. Mack and M. G. Ory, “AIDS and Older Americans at the End of the Twentieth Century,” Journal of Acquir- ed Immune Deficiency Syndromes, Vol. 33, No. S2, 2003, pp. S68-S75. doi:10.1097/00126334-200306012-00003 [49] E. A. Operskalski, J. W. Mosley, M. P. Busch and D. O. Stram, “Influences of Age, Viral Load, and CD4+ Count on the Rate of Progression of HIV-1 Infection to AIDS,” Journal of Acquired Immune Deficiency Syndromes & Human Retrovirology, Vol. 15, No. 3, 1997, pp. 243-244. doi:10.1097/00042560-199707010-00009 [50] R. B. Effros, C. V. Fletcher, K. Gebo, et al., “Aging and Infectious Diseases: Workshop on HIV Infection and Aging: What Is Known and Future Research Directions,” Clinical Infectious Diseases, Vol. 47, No. 4, 2008, pp. 542-553. doi:10.1086/590150 [51] K. Crothers, A. A. Butt, C. L. Gibert, M. C. Rodriguez- Barradas, S. Crystal and A. C. Justice, “Increased COPD among HIV-Positive Compared to HIV-Negative Veter- ans,” Chest, Vol. 130, No. 5, 2006, pp. 1326-1333. doi:10.1378/chest.130.5.1326 [52] J. L. Goulet, S. L. Fultz, K. A. McGinnis and A. C. Jus- tice, “Relative Prevalence of Comorbidities and Treat- ment Contraindications in HIV-Mono-Infected and HIV/HCV-Co-Infected Veterans,” AIDS, Vol. 19, Suppl. 3, 2005, pp. S99-S105. doi:10.1097/01.aids.0000192077.11067.e5 [53] H. K. Monga, M. C. Rodriguez-Barradas, K. Breaux, et al., “Hepatitis C Virus Infection-Related Morbidity and Mor- tality among Patients with Human Immunodeficiency Vi- rus Infection,” Clinical Infectious Diseases, Vol. 33, No. 2, 2001, pp. 240-247. doi:10.1086/321819 [54] F. Bonnet, P. Morlat, G. Chene, et al., “Causes of Death among HIV-Infected Patients in the Era of Highly Active Antiretroviral Therapy, Bordeaux, France, 1998-1999,” HIV Medicine, Vol. 3, No. 3, 2002, pp. 195-199. doi:10.1046/j.1468-1293.2002.00117.x [55] N. Friis-Moller, C. A. Sabin, R. Weber, et al., “Combina- tion Antiretroviral Therapy and the Risk of Myocardial Infarction,” The New England Journal of Medicine, Vol. 349, No. 21, 2003, pp. 1993-2003. doi:10.1056/NEJMoa030218
|