Health
Vol.5 No.12(2013), Article ID:41087,6 pages DOI:10.4236/health.2013.512285
Sleep breathing disorders in female population of Dubai, UAE*
![]()
Sleep Disorders Center, Department of Medicine, Rashid Hospital, Dubai Health Authority, Dubai, United Arab Emirates; #Corresponding Author: HALHARIRI@DHA.GOV.AE
Copyright © 2013 Bassam Mahboub et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 12 October 2013; revised 18 November 2013; accepted 27 November 2013
Keywords: Obstructive Sleep Apnea; Snoring; Daytime Sleepiness; Prevalence Primary Care; Berlin Questionnaire; Dubai
ABSTRACT
PURPOSE: United Arab Emirates (UAE) is part of the GCC countries and ranks 18 on 2007 WHO list of the fattest countries with 68.3% of its citizens with an unhealthy weight. The WHO data in 2008 state that the prevalence of overweight in UAE is 71%, while it is 61% in the UK, 54% in Germany, and 45% in France. The increasing overweight and obesity in the UAE are closely related to high social-economic development. Accordingly, the medical authority has observed that the rates of hypertension and diabetes mellitus type 2 appear to be one of the highest rates worldwide. We presume that the increase prevalence of obesity in the UAE would be linked to the increase in prevalence of obstructive sleep apnea syndrome (OSAS). The purpose of this study is to estimate the prevalence of symptoms and risk of OSAS in women followed up in the primary health care (PHC) setting in Dubai and the relationship between obesity and sleep apnea in females in the UAE. DESIGN: Prospective observational community-based survey. SETTING: 20 primary health centers in Dubai. PARTICIPANTS: Consecutive female patients who were older than 14 years, regardless of the reason of their visit. METHODS: In this prospective survey, trained medical nurse administered the Berlin Questionnaire (which includes questions about self-reported snoring, witnessed apneas, daytime sleepiness, hypertension, and obesity) to a consecutive random sample of female patients in the age group older than 14 years, attending the PHC center in Dubai Health Authority, Dubai, UAE, from September 2011 to March 2012. Based on the questionnaire, individuals were classified into high-risk and low-risk groups for OSAS. RESULTS: Based on the responses and measurement of the Berlin Questionnaire of 704 female subjects studied, 137 respondents met the criteria for the high-risk scoring. This gives a prevalence rate of 19.5% while the remainders of the participants were classified as low risk. The overall mean age of the high risk for OSAS female respondents was 39.95 ± 11.73 years. The highest prevalence was noticed between age group 51 to 60 years. 70% of the high risk group patients had Body Mass Index (BMI) ≥30 kg/m2 and nearly 75% of the low risk group had BMI wang#Bracket##30 kg/m2 and the Mean BMI was 33.59 ± 6.44 kg/m2. CONCLUSIONS: One in five women in Dubai, UAE is at high risk of having OSAS. Awareness by the primary care medical community about this disorder in females should be increased so that the patients would benefit from proper evaluation and treatment of OSAS.
1. INTRODUCTION
Obstructive sleep apnea syndrome (OSAS) is a sleep disorder characterized by snoring, repetitive pauses of breathing which can last from at least 10 seconds to minutes leading to sleep fragmentation, excessive daytime sleepiness, fatigue, and impaired cognition. These symptoms may present for years without identification as the sufferer may become conditioned to these symptoms. The most common cause of OSAS is the partial or complete stoppage of the flow of air due to the relaxation of the muscles which surround the throat and tongue and vary greatly among individuals and may vary considerably among groups defined on the basis of age, sex, body habits, race, ethnicity and overweight.
General population-based studies have shown that the prevalence of OSAS in female is higher than the prevalence reported by clinic-based population studies. Examining the entire sleep apnea spectrum may decrease the difference in prevalence of OSAS between males and females to 1.5:1. Reasons for gender-related differences are not fully explained. Possible explanations include differences in upper airway anatomy, collapsibility and resistance and difference of hormonal influence on upper airways dilator muscle activity. Moreover, it was estimated that more than 90% of women with sleep apnea may be under diagnosed.
OSAS is a condition linked to high morbidity and mortality in both men and women. Thus it is crucial to increase the awareness of the medical community about the high prevalence of OSAS in women as the risk in women is increased with advanced age, the presence of obesity, irregularity of the menstrual cycle, and menopause. Pregnant women had a similar risk for OSAS as non-pregnant women, and, more importantly in those pregnant women with high risk for OSAS, the reporting of pregnancy complications was very high. Women at high risk for OSAS have greater morbidity than women at low risk [1].
Obesity is a growing health concern in the United Arab Emirates with health officials stating that it is one of the leading causes of preventable deaths in the United Arab Emirates and UAE ranks 18 on a 2007 list of fattest countries with 68.3% of its citizens with an unhealthy weight [2]. Obesity is 2.3-fold higher among UAE female at 14 years compared to international standards, and increased to 1.9 times at 18 years of age in female [3].
Until now, no data have been reported the relationship between obesity and sleep apnea in female population in Dubai. This study performed a standardized survey of primary care outpatients from different socio-economic ranges to measure the prevalence of symptoms of OSAS among female residents of Dubai (both UAE citizens and expatriates). This data will confirm to the local authority the importance of proper evaluation of OSAS by health workers to reduce burden of OSAS and expand the sleep service. The expansion of sleep service in this community is needed for appropriate counseling for the high risk cases of OSAS.
OSAS is a common medical condition with significant adverse medical and public health consequences. Primary care has a central role for recognizing cases of OSAS in the community [4]. Patients attending PHC clinics tend to have higher risk for OSAS because these patients often have chronic illnesses that are associated with OSAS. Population-based epidemiologic studies have uncovered the high prevalence and wide spectrum of severity of undiagnosed obstructive sleep apnea, and have consistently found that even mild obstructive sleep apnea is associated with significant morbidity and mortality causing an additional burden on the public health service and it is a potentially disabling condition. The community prevalence of symptoms and/or signs of OSAS varies by region and by country [5]. In the United States, the estimated 9% and 24% of women and men, respectively, aged 30 to 60 years have at least mild OSAS [6]. In other Western countries the overall prevalence of mild and moderate OSAS is estimated at 20% and 7%, respectively [4].
In New Delhi, a community-based study reported a prevalence of 14% for OSAS in middle-aged men [7]. In the Middle East, one study was done in Jordan and it showed that the high risk of OSAS was present in 106/554 (19.1%) of men and in 96/651 (14.7%) of women (P = 0042) [8]. No such data have been reported showing the relationship between obesity and sleep apnea in female population in Dubai.
The practice of sleep medicine in Dubai began in the last few years and it is a relatively new specialty in the medical community. Since its inception, the specialty has grown, and now it is important to assess the prevalence of this disease in this community, so we performed a standardized survey of primary care outpatients from a diverse socioeconomic range to measure the prevalence of symptoms of OSAS among female residents of Dubai (UAE citizens and Expatriate) and those data will confirm the local authority that public health initiatives with clinical support are warranted to reduce the burden of OSAS and proper evaluation for OSAS by the health care workers is urgently needed and expansion of sleep service in this community is needed for appropriate counseling for the high risk cases of OSAS.
2. PARTICIPANTS
The study was approved by the ethics committee in DHA and the Participants were selected from consecutive female patients who were >14 years of age, regardless of the reason for the visit to primary care centers in Dubai Health Authority (DHA) which is the main Dubai government department which governs healthcare, medical policy and strategy in Dubai, and monitors public and private hospitals, clinics, and medical centers in Dubai.
2.1. METHODS
We used Berlin questionnaire as a screening tool to identify subjects who are at high risk or low risk for OSAS by identifying snoring behavior, daytime sleepiness, obesity, and hypertension [9]. This was developed in April 1996 in Berlin, Germany. Berlin questionnaire is a simple instrument that has been extensively studied in primary care settings and has shown very high positive predictive value (89%) with a reasonable Sensitivity and specificity of 86% and 77% respectively [10].
Patients were also asked to provide information on age, weight, height, sex, and ethnicity and the information (specifically height and weight) was verified by qualified medical staff.
Respondents were classified into either high risk or lower risk for sleep apnea based on their responses in 3 symptom categories. To score “high” for OSAS, an individual’s questionnaire must have had positive scores in two of the three categories, or in all three. Those patients who denied having symptoms with such frequency, who did not report symptoms to permit risk assessment or who qualified in only one category were placed into a lower risk group [10,11]. Height was measured by using height meter, while a weighing scale was used for measuring the weight to the nearest kilogram. BMI was calculated using weight in kilograms over height in meters square (kg/m2). The patients were asked to complete the questionnaire in the office in the PHC center then it was sent to the local study group specialist, the questionnaire was offered in English languages (with Arabic translation form).
2.2. Statistical Analysis
Risk for OSAS groups was analyzed using Statistical Package for Social Sciences (SPSS). Multivariate analysis of factors associated with high risk for OSAS was conducted using binary logistic regression.
3. RESULTS
Demographics and frequency distribution of age 704 female respondents were included in this analysis based on the responses and measurement of the Berlin Questionnaire of these subjects. The age range of female respondents was from 14 to 75 years. The overall mean age of was 35.87 ± 12.19 years ( range 14 - 75 years ) and the mean BMI was 28.53 ± 6.49 kg/m2 (range 13.85 - 57.04 kg/m2). Nearly 77% respondents were between the ages of 21 to 50 years. Attached Table 1 summarizes the distribution of age & BMI per age groups for all respondents.
Prevalence of risk of OSAS: Out of 704 respondents, 19.5% (n = 137) respondents met the criteria for the high-risk of OSAS revealing a prevalence rate of 19.5%, while the remainders of the participants (80.5% n = 567) were classified as low risk.
In the high risk group patients, the overall mean age was 39.95 ± 11.73 years and the overall mean BMI was 33.59 ± 6.44 kg/m2. Attached Table 2 summarizes the distribution of age & BMI per age groups for the high risk of sleep apnea.
When looking from the nationality perspective, we found that the 22.0% of local UAE female patients were categorized as high risk of OSAS (c/f 13% for the expatriates females), while the proportion of female patients in low risk for OSAS was 78.0% for local UAE female patients (c/f 87% for the expatriates females). Attached Table 3 summarizes the risk of sleep apnea among local and non local participants and Figure 1 summarizes the prevalence of high-risk Berlin Questionnaire scores by age for males (blue) and females (red).
4. DISCUSSION
Present study is the only study from Dubai, UAE with large data set providing information on snoring, sleepi
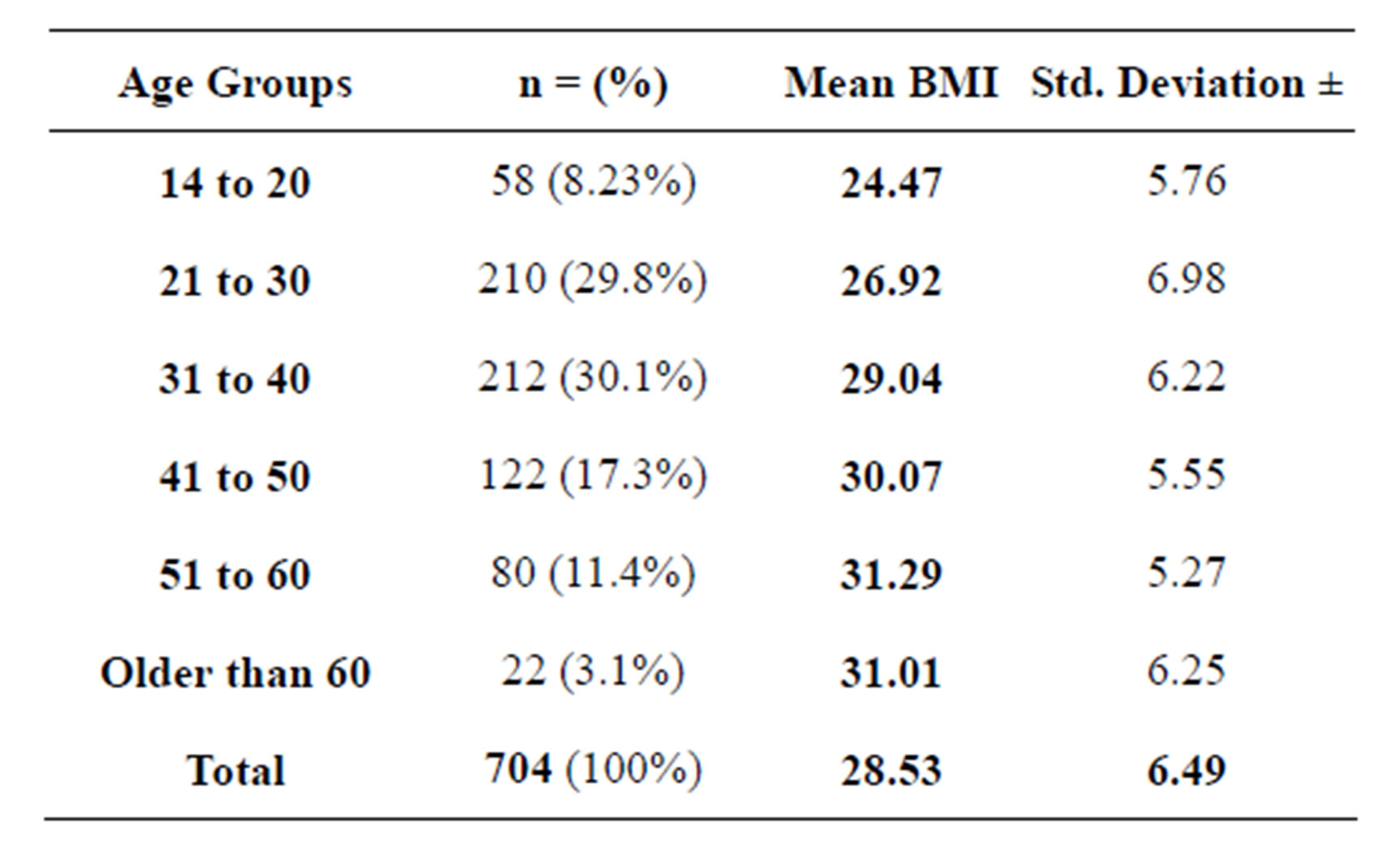
Table 1. All respondents—frequency distribution of age & BMI summaries as per age groups.
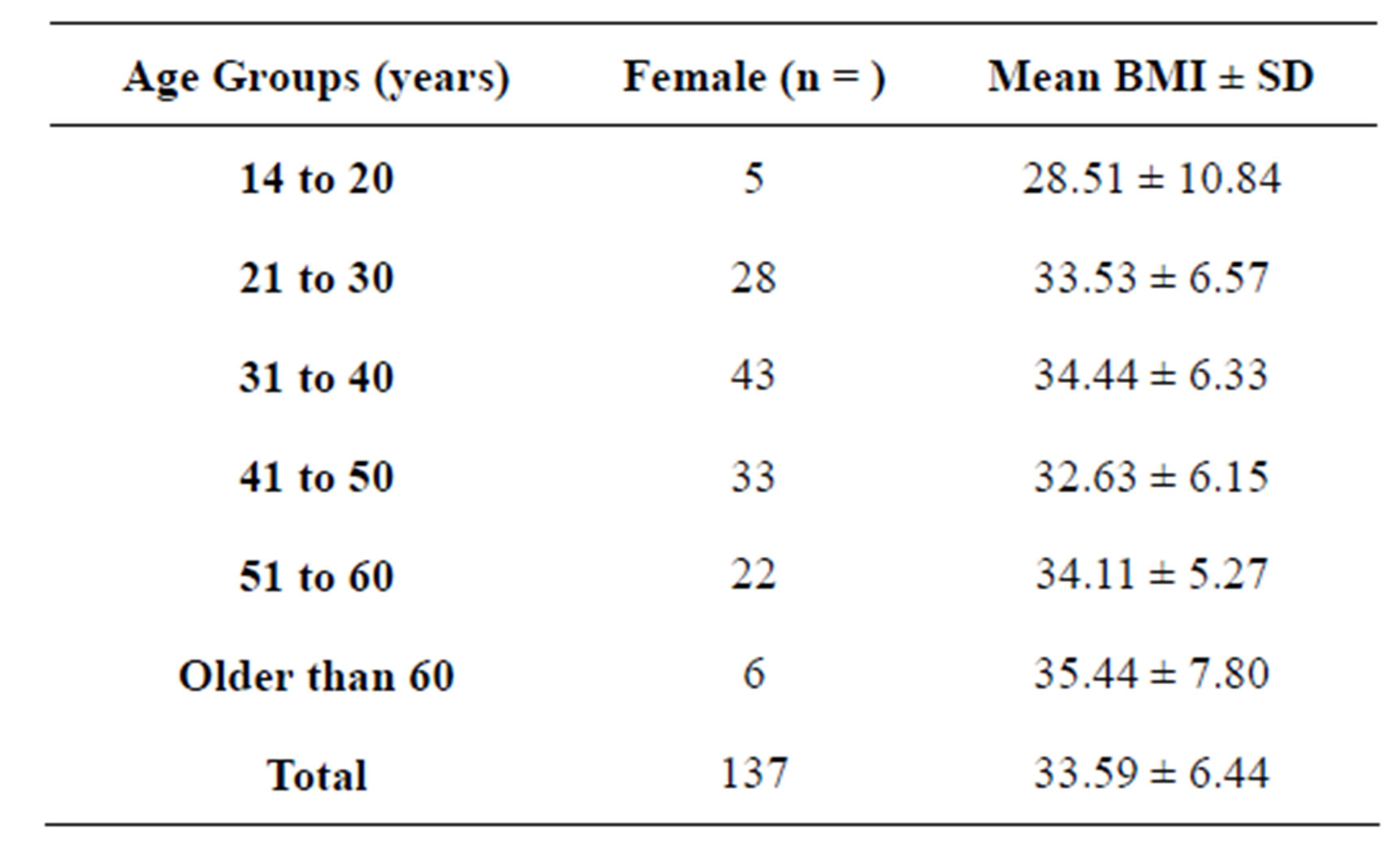
Table 2. All high risk respondents—frequency distribution of age & BMI summaries as per age groups.
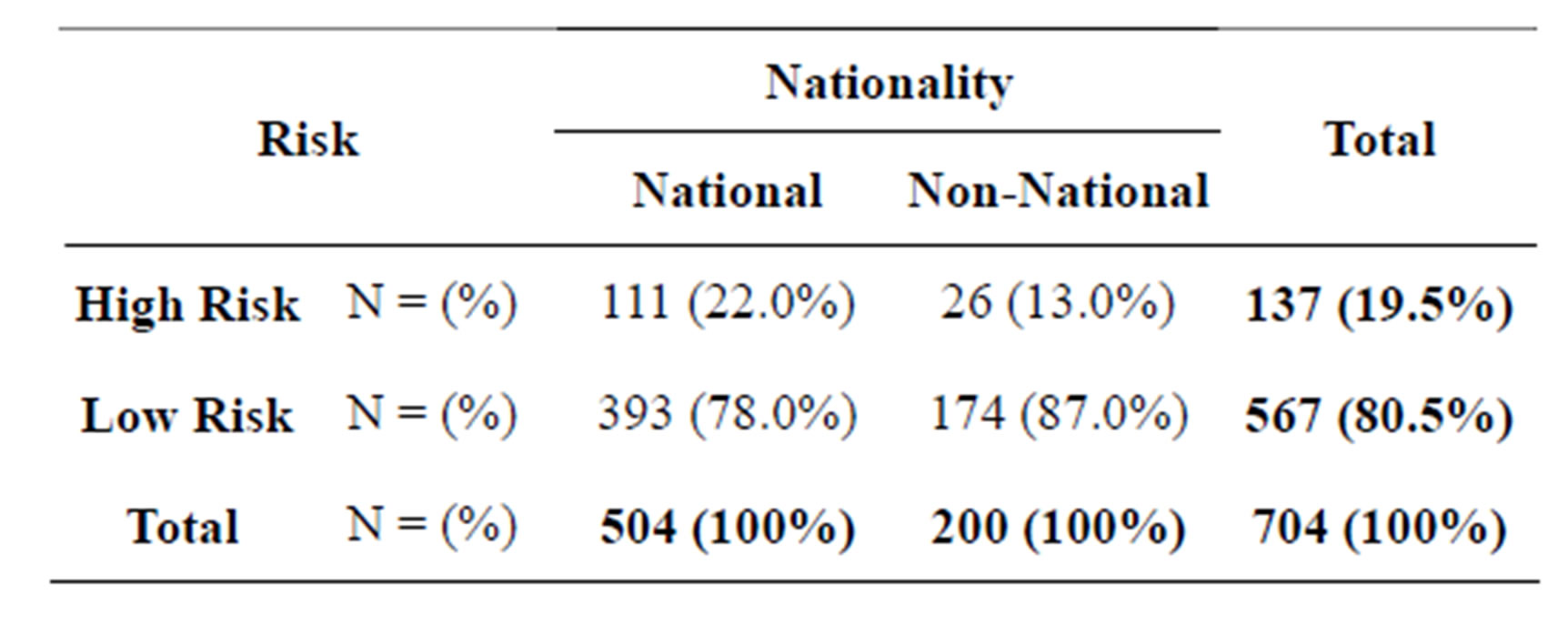
Table 3. Prevalence of risk of OSAS by nationality.
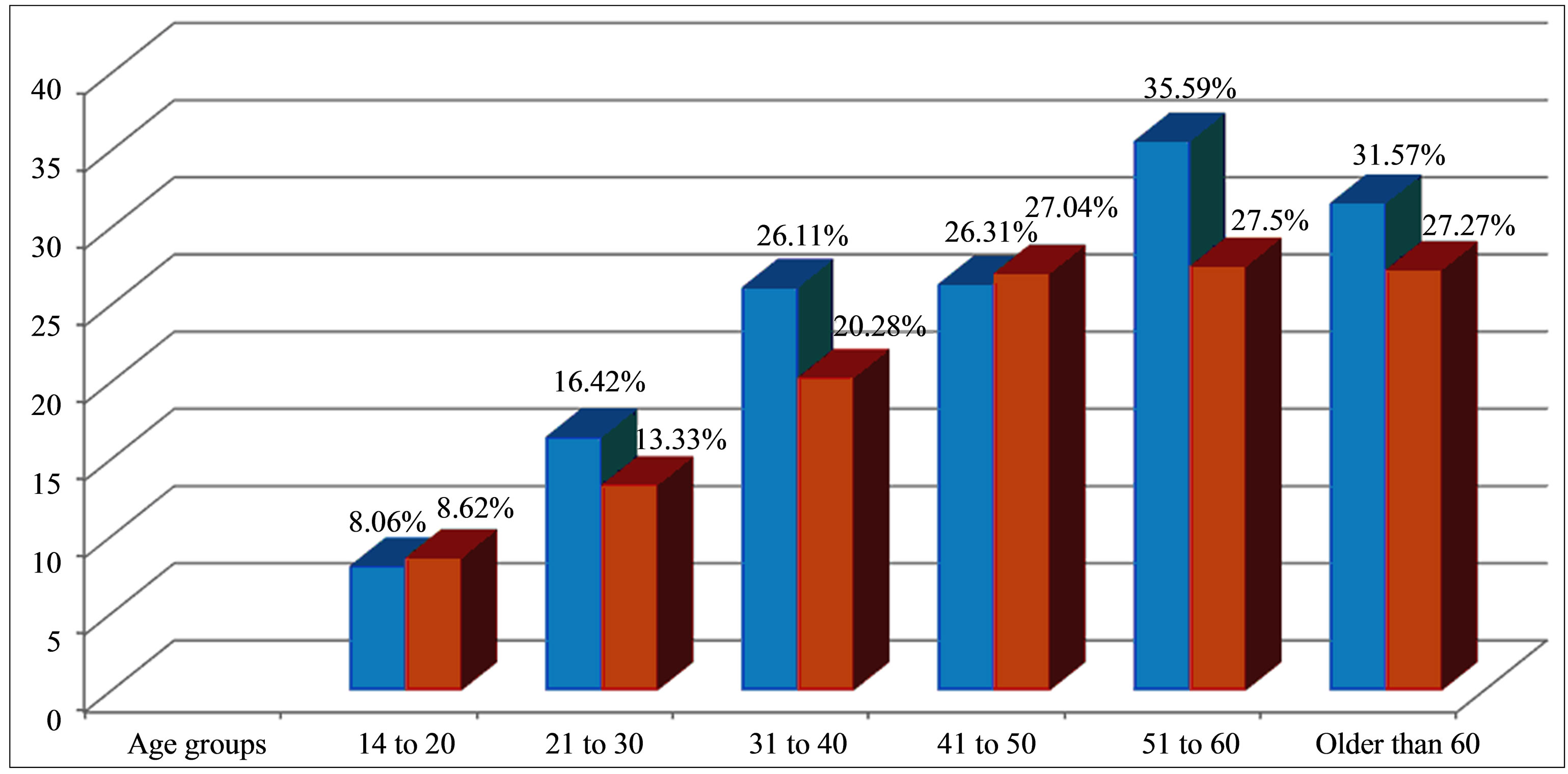
Figure 1. Prevalence of high-risk Berlin Questionnaire scores by age for males (blue) and females (red).
ness, and other features associated with OSA in female population including both local and expatriates patients and it demonstrates that OSAS is highly prevalent in the female population of Dubai, as it is in other countries with nearly 19.5% of the females respondents have been categorized as high risk of OSAS.
Association of male gender with risk of OSAS is well described. However, many recent studies has reported high prevalence of OSAS in elderly females and this proportion is rising through out the world including middle east. Community-based studies from western countries have reported that OSAS is more common in males compared with females. In Jordan, the high risk of OSAS was present in 106/554 (19.1%) of men and in 96/651 (14.7%) of women (P = 0042) [8]. In Iran, similar type of study based on Berlin Questionnaire found that high risk for OSAS exists in 12.95% of men (v/s 8.3% of women) and about 51.5% females suffered from snoring [12]. The finding of our study is really striking showing higher prevalence of OSA in the female respondents compared to other studies in Gulf region (prevalence of high risk for OSAS in female respondents was 19.5% in our study v/s 14.7% in Jordanian study) which indicates that the females in Dubai (predominantly UAE nationals) are more prone to OSAS risk with consequences of OSA compared to other females in the middle east or other regions in the world and we conclude that even OSAS is a male dominant disorder but we noticed a higher prevalence of OSAS in the female respondents in Dubai. This finding should be taken in to account when planning the women and health strategies in UAE with emphasis upon early diagnosis and management of obesity and OSA.
Obesity was a strong predictor of OSAS risk: A population-based study in the United States revealed that obesity was a strong predictor of OSAS risk [13]. Among obese subjects (BMI ≥ 30 kg/m2) 59% of subjects were at high risk of OSAS. While in another study from Korean population it showed that a significant percentage of the subjects were not obese but still had OSAS. They speculated that other risk factors, such as contents/distribution of body fat and anatomical structure of upper airway, may be responsible for the higher prevalence of OSAS in Korean population. Our study also revealed a close association between high BMI and the risk of OSAS in the population of Dubai, among obese subjects (BMI ≥ 30 kg/m2) 70% were at high risk of OSAS and nearly 75% of the low risk group have BMI < 30 kg/m2, which indicates obesity is a very strong predictor of OSAS risk in Dubai. However we did not find craniofacial abnormality as an important factor predisposing to high risk of OSA. Hormonal factors could play an important role in the development of obesity in females with consequent OSAS, Obesity is more common in female respondents: Obesity in general is more common in women than men [14]. In the USA, 24.9% of women versus 19.9% of men had a BMI greater than 30. In Saudi Arabia, women are significantly more obese than men with a prevalence of 44% and 26.4%, respectively. In our study, we found that women in Dubai are significantly more obese than men (similar to Saudi Arabia) with a prevalence of 39.63% and 32.61%, respectively and the highest BMI of the respondents was noticed in elderly female respondents. The female respondents in age group of >60 years had the highest BMI among the female population with a mean BMI of 35.44 ± 7.80 kg/m2. This pandemic of obesity could be contributed by the rapid westernization of life style, lack of physical exercise, unknown genetic factors, hot and humid climate preventing outdoor activities in this country and the traditional dress in the Middle East (wearing of loose, flowing garments such as the dish-dash or abayas) excess weight gained goes relatively unnoticed and they notice obesity only when it starts giving problem in day to day life viz. breathlessness, less exercise capacity or when it manifests as diabetes or hypertension or other medical issue or when diagnosed by the physician.
The highest prevalence of high risk for OSAS was noticed between age group 51 - 60 years in female population. The overall mean age of the high risk for OSAS female respondents was 39.95 ± 11.73 years and the prevalence is increasing with aging and the highest prevalence was notice between age 51 to 60 years in female gender, and the high risk of OSAS was present in 27.5% of women in this age group.
Limitations of the study: There are some limitations to consider, we did not independently confirm or refute reporting of snoring or day time sleepiness by the respondents. However the concordance between patient selfreporting and bed-partner reporting of snoring and apneic episodes is sufficiently high to believe that there might not be over reporting of these symptoms [15]. The study did not include information on the utility of the Berlin questionnaire with regards to patient outcome.
The Berlin Questionnaire does not capture all information that a physician might want or seek, nor does it substitute for direct measurements of breathing during sleep (polysomnography), however, the self-report format is convenient, simple and cost effective, and may be more uniform in presentation compared to face-to-face screening.
We know that’s sleep questionnaires despite being useful in assessing risk for OSA, are not interchangeable with polysomnography and cannot quantify the severity of disease. Thus, the prevalence of people at high risk for OSA based on questionnaires cannot be simply converted into the prevalence of OSA.
5. CONCLUSIONS
In the PHC setting, the prevalence of symptoms/high risk of OSAS among adult females in UAE is very high and this is a real serious public health threat. Patients who are at high risk of Sleep apnea may benefit from proper screening, evaluation and appropriate counseling by the PHC physicians. Polysomnography is labor intensive, time consuming and not easily available to all patients especially with insurance limitations. Hence screening of patients with Berlin Questionnaire along with proper sleep history is essential in order to find out the patients who are at high risk of OSAS.
Given the high prevalence of OSA in the female population, it is important that public awareness program with administrative collaboration including new health policies for obese females may play a very important role to control the prevalence of obesity and consequent OSAS in Dubai, UAE.
REFERENCES
- Punjabi, N.M. (2008) The epidemiology of adult obstructive sleep apnea. Proceedings of the American Thoracic Society, 5, 136-143. http://dx.doi.org/10.1513/pats.200709-155MG
- Streib, L. (2007) World’s fattest countries. Forbes, New York.
- Al-Haddad, F.H. and Little, B.B. (2005) Childhood obesity in United Arab Emirates schoolchildren: A national study. Annals of Human Biology, 32, 72-79.
- Dement, W.C. and Netzer, N.C. (2000) Primary care: Is it the setting to address sleep disorders. Sleep Breath, 4, 1-6. http://dx.doi.org/10.1055/s-2000-11529
- Young, T., Peppard, P.E. and Gottlieb, D.J. (2002) Epidemiology of obstructive sleep apnea: A population health perspective. American Journal of Respiratory and Critical Care Medicine, 165, 1217-1239. http://dx.doi.org/10.1164/rccm.2109080
- Young, T., Palta, M., Dempsey, J., et al. (1993) Te occurrence of sleep-disordered breathing among middle-aged adults. The New England Journal of Medicine, 328, 1230- 1235. http://dx.doi.org/10.1056/NEJM199304293281704
- Sharma, S.K., Vasudev, C., Sinha, S., Banga, A., Pandey, R.M. and Handa, K.K. (2006) Validation of the modified Berlin questionnaire to identify patients at risk for the obstructive sleep apnea syndrome. Indian Journal of Medical Research, 124, 281-290.
- Basheer, Kh. and Mohammad, Gh. (2009) Symptoms and risk of obstructive sleep apnea in primary care patients in Jordan. Sleep Breath, 13, 227-232. http://dx.doi.org/10.1007/s11325-008-0240-4
- Netzer, N.C., Stoohs, R.A., Netzer, C.M., et al. (1999) Using the Berlin questionnaire to identify patients at risk for the sleep apnea syndrome. Annals of Internal Medicine, 131, 485-491. http://dx.doi.org/10.7326/0003-4819-131-7-199910050-00002
- Netzer, N.C., Hoegel, J.J., Loube, D., et al. (2003) Prevalence of symptoms and risk of sleep apnea in primary care. Chest, 124, 1406-1414. http://dx.doi.org/10.1378/chest.124.4.1406
- (2000) Reprinting of the Berlin questionnaire. Sleep Breath, 4, 187-192.
- Khazaie, H., Naja, F., Rezaie, L., Tahmasian, M., Sepehry, A.A. and Herth, F.J.F. (2011) Prevalence of symptoms and risk of obstructive sleep apnea syndrome in the general population. Archives of Iranian Medicine, 14, 335- 338.
- Hiestand, M., Britz, P., Goldman, M., et al. (2006) Prevalence of symptoms and risk of sleep apnea in the US population: Results from the national sleep foundation sleep in America 2005. Chest, 130, 780-786. http://dx.doi.org/10.1378/chest.130.3.780
- Redline, S., Kump, K., Tishler, P.V., et al. (1994) Gender differences in sleep disordered breathing in a community-based sample. American Journal of Respiratory and Critical Care Medicine, 149, 722-726. http://dx.doi.org/10.1164/ajrccm.149.3.8118642
- Kump, K., Whalen, C., Tishler, P.V., et al. (1994) Assessment of the validity and utility of a sleep-symptom questionnaire. American Journal of Respiratory and Critical Care Medicine, 150, 735-741. http://dx.doi.org/10.1164/ajrccm.150.3.8087345
ABBREVIATIONS
BMI: Body Mass Index;
OSAS: Obstructive Sleep Apnea Syndrome;
DHA: Dubai Health Authority;
PHC: Primary Health Care;
NOTES
*Conflict of Interest Statement: None of the authors have a conflict of interest to declare in relation to this work.